Article Text

Abstract
This is a case report of a patient who sustained a stab wound to the right axilla with injuries to the right axillary artery and vein. The patient had near-exsanguination in the field and no recordable blood pressure upon admission to the trauma center. Resuscitation was performed with endotracheal intubation, a left anterolateral resuscitative thoracotomy with cross-clamping of the descending thoracic aorta, and the rapid infusion of crystalloid solutions and packed red cells. In the operating room, the third portion of the right axillary artery and the adjacent right axillary vein were found to be transected. As part of a ‘damage control’ procedure, the ends of the right axillary vein were ligated. A 14 French intra-arterial shunt was inserted into the transected ends of the right axillary artery to restore the flow to the right upper extremity. The patient’s postoperative course was complicated by a coagulopathy, adult respiratory distress syndrome (ARDS), and anuria. The coagulopathy and anuria resolved within the first 48 hours, but the patient’s ARDS was slow to resolve. On the 10th postinjury day, the patient was returned to the operating room for a definitive repair of the right axillary artery. After the intra-arterial shunt was removed, a reversed greater saphenous vein graft was inserted between the ends of the right axillary artery in a medial intermuscular (extra-anatomic) tunnel. The patient made an uneventful recovery and was discharged home on the 16th postinjury day.
The following principles of advanced trauma care were part of the management of this patient: (1) occasional need for resuscitative thoracotomy with cross-clamping of the descending thoracic aorta in a patient without a thoracic injury; (2) ‘damage control’ operation with ligation of the right axillary vein and placement of a temporary intra-arterial shunt to restore the flow to the right upper extremity; and (3) vascular reconstruction with an extra-anatomic bypass in a previously contaminated field.
- extremities
- wounds, penetrating
- arm injuries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
History
A young patient was stabbed in the right axilla and had near-exsanguination in the field. The patient was barely responsive and covered with blood when the emergency medical service arrived. A pressure dressing was quickly applied to the wound in the right axilla. During transport to the trauma center, there was no audible blood pressure for the last 3 minutes of the trip.
Examination
The patient was unresponsive, his clothes were soaked with blood, and there was no palpable pulse, though there was an obvious tachycardia on the monitor. The dressing over the stab wound in the right axilla was saturated with blood.
Question
After intubation, the most appropriate next step in management is:
Left anterolateral thoracotomy.
Insertion of a REBOA device.
Application of a tourniquet.
Insertion of a transradial artery balloon.
Management
The patient was thought to be in a near-arrest state from exsanguination, and a left anterolateral thoracotomy with cross-clamping of the descending thoracic aorta (barely palpable pulse) was performed. Large-bore intravenous catheter were inserted into the left upper extremity for resuscitation. A tight pressure dressing was applied to the stab wound in the right axilla, and the patient was moved rapidly to the operating room with the aortic cross-clamp in place.
After preparation and draping of the entire anterior chest, the right axilla, and the right groin and thigh, the pressure dressing on the stab wound was removed. The stab wound was extended superiorly into the right infraclavicular area and inferomedially into the right biceps-triceps groove. The third portion of the right axillary artery (lateral border of pectoralis minor muscle to inferior border of teres major muscle) and the adjacent axillary vein were both transected.
Question
The most appropriate next step in management is:
Ligation of all four ends of the transected vessels.
Insertion of autogenous saphenous vein grafts.
Ligation of the vein ends and shunt into artery.
Insertion of endovascular stent grafts.
Management
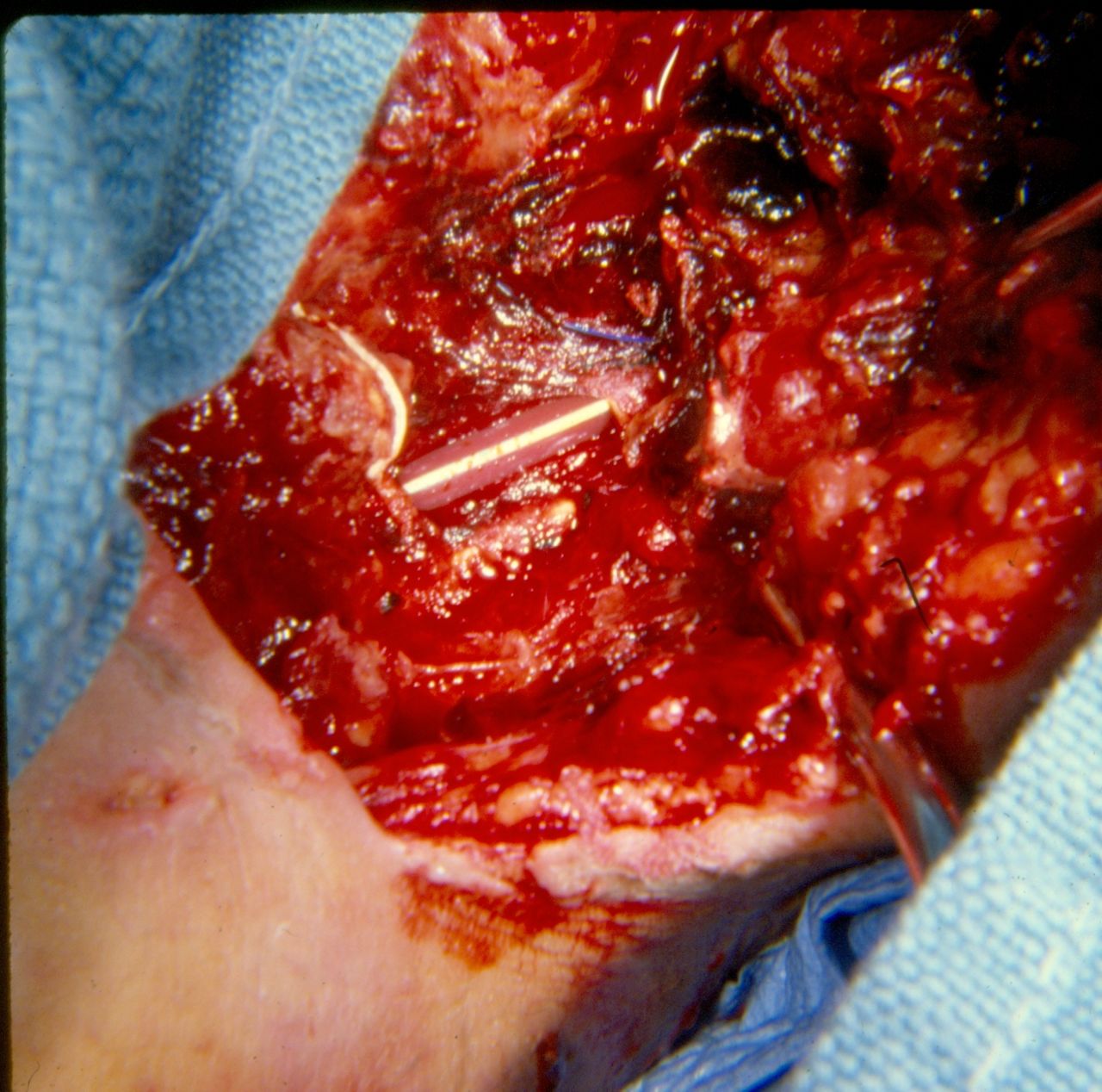
Both ends of the transected right axillary vein were ligated. A 14 French (Fr) Argyle intra-arterial shunt was inserted into the ends of the transected right axillary artery and held in place with 2-0 silk ties at either end (figure 1). A barely palpable right radial pulse was noted immediately.

{kind=link}
14 French (Fr) Argyle shunt in third portion of the right axillary artery.
As transfusion of type-specific packed red cells and fresh frozen plasma continued and intermittent intravenous boluses of epinephrine were administered during operation, the patient’s systolic blood pressure rose to 100 mm Hg. The cross-clamp on the patient’s descending thoracic aorta was gradually released and then removed. Despite the presence of diffuse oozing, two 38 Fr thoracostomy tubes were inserted into the left hemithorax and the left anterolateral thoracotomy incision was closed in layers. In addition, the skin of the laceration/incision in the right axilla was closed with a continuous suture.
The patient’s early postoperative course in the intensive care unit was complicated by the coagulopathy, early-onset adult respiratory distress syndrome (ARDS), and anuria. The coagulopathy and anuria resolved during the first 48 hours after continuing resuscitation, whereas the ARDS gradually improved during the next 1.5 weeks. The right radial pulse was palpable throughout this period.
After 10 days, however, the patient remained ventilator dependent. He was returned to the operating room, the right axillary laceration/incision was reopened, and systemic anticoagulation was initiated with a bolus of unfractionated heparin.
An extra-anatomic intermuscular tunnel was created through the medial right axilla using a large Bakes dilator as a segment of the right greater saphenous vein was removed from the groin. The saphenous vein graft was then filled with heparinized saline and passed through the intermuscular tunnel tied to the dilator. After removal of the shunt, a No 4 Fogarty balloon catheter was passed through both ends of the right axillary artery without any thrombus being retrieved. The extra-anatomic saphenous vein bypass was completed by end-to-end anastomoses to the proximal and distal ends of the right axillary artery. A right radial pulse was palpable after removal of the vascular clamps.
The patient was extubated on the 12th postinjury day and was discharged home on the 16th postinjury day.
Discussion
The choice of a resuscitative thoracotomy would be controversial in the modern era, particularly in a patient with a peripheral rather than a thoracic vascular injury. Rapid insertion of a REBOA device, rapid blood transfusion, and application of a new pressure dressing on the right axilla would have been the preferred management in some centers.1 In this patient with no blood pressure during the latter stages of transport and no palpable pulse in the trauma room, a cardiopulmonary arrest appeared imminent. For this reason, a resuscitative thoracotomy with cross-clamping of the descending thoracic aorta was chosen.2
Ligation of the right axillary vein rather than insertion of a temporary intraluminal shunt was another controversial choice in management of this patient. Significant injuries to the axillary vein, however, have been managed with ligation rather than complex reconstruction for many years in urban trauma centers. Although edema of the ipsilateral upper extremity may occur in the hospital, it essentially always resolves after several days of elevation. This is related to the extensive venous collateral network around the axilla as follows: (1) venae comitantes of the brachial artery; (2) profunda brachii, posterior humeral circumflex, and circumflex scapular venae comitantes; (3) subscapular and suprascapular veins; and (4) external jugular vein.3
The history of the use of temporary intraluminal vascular shunts has been summarized in several publications during the past decade.4 5 While there are multiple possible indications for insertion of a shunt (box 1), the majority are inserted in patients with Gustilo IIIC open fractures or in those with a significant vascular injury and the need for ‘damage control’.
Possible indications for insertion of a temporary vascular shunt after trauma*
Complex repair of the internal carotid artery in zone III of the neck.
Need for distal perfusion as a complex revascularization is performed.
Gustilo IIIC open fracture of an extremity.
Perfusion of an amputated part of an upper extremity prior to replantation.
‘Damage control’ for the patient with near-exsanguination from a peripheral vascular injury.
‘Damage control’ for the patient with multiple intra-abdominal injuries including an abdominal vascular injury.
‘Damage control’ for the patient with a cervical, truncal, or peripheral vascular injury and a surgical team with an overwhelming number of casualties, limited resources, or limited experience with vascular injuries (military triage).
*Adapted from Feliciano and Subramanian.5
The largest possible shunt should be inserted into the transected or debrided ends of the vessel. In the largest civilian series from one institution, the peripheral arteries most commonly shunted were the superficial femoral and popliteal.6 Over 50% of the shunts inserted into these vessels were either 14 or 12 Fr Argyle.
When dealing with pediatric arterial injuries, a 5 or 8 Fr feeding tube can be used. The peripheral veins most commonly shunted in the same review were the popliteal and femoral, and over 55% of the shunts inserted into these vessels were either 14 or 12 Fr Argyle. For larger veins such as the common femoral, external iliac, axillary, or subclavian, an Argyle thoracostomy tube can be used.
The length of the shunt to be inserted should be 4 cm longer than the gap between the two ends of the vessel.5 Also, a 2-0 silk tie should be placed around the midpoint of the shunt for orientation during and after insertion. The shunt is clamped at its midpoint with a hemostat and placed 1.5 cm into the proximal open end of the transected artery (or the end nearest the foot or hand of the transected vein) and fixated in place with a 2-0 silk tie. The hemostat is removed to verify the flow through the shunt and then replaced. After insertion of the distal end of the shunt 1.5 cm and fixation with a 2-0 silk tie, the hemostat is removed. The flow through an arterial shunt is verified by palpable or Doppler-audible pulsations beyond the shunt. Dilatation of the vein beyond the shunt or Doppler-audible continuous flow confirms patency of the shunt.
There are no convincing data that systemic or locally injected anticoagulation lowers the 5% to 10% postoperative rate of thrombosis of intra-arterial shunts.7 8 In addition, anticoagulation would be contraindicated in many of the patients with multiple injuries and/or ‘damage control’ patients in whom temporary intravascular shunts are inserted. The cumulative experience with shunts during the past 25 years suggests that early postoperative occlusion is most frequently due to one of the following: small shunt size (failure to dilate end of artery in spasm before insertion); or loss of venous outflow from proximal ligation or venous thrombosis related to the original injury or a narrowed repair, particularly in the lower extremity. Thrombosis of a postoperative arterial shunt is often predictive of the need for later amputation of an injured extremity.
Many shunts in patients with Gustilo IIIC fractures are removed at a first operation after orthopedic fixation allows for an easier vascular reconstruction.9 Patients with a ‘damage control’ indication, however, most commonly leave the operating room with the shunt in place. In the aforementioned large civilian review from Grady Memorial Hospital, Atlanta, Georgia, in 2008, the average ‘dwell’ time for a shunt was 23.5±15.7 hours (2–71).6 A more recent civilian multicenter review of 213 shunts in 201 patients from seven level I trauma centers over 9 years (2005–2013) listed the following dwell times: less than 6 hours—61.4% of all shunts; 24 hours—86.5%; and 48 hours—95.9%.10 The longest ‘dwell’ time for an arterial shunt in the American literature (10 days) is the patient described in this report.11
In all patients with significant injuries to a vessel managed with a shunt, bone, and soft tissue in an extremity, an extra-anatomic bypass should be considered at the time of removal of the shunt and vascular reconstruction. This approach decreases the risk of a saphenous vein graft or suture line (vessel-plastic graft) blowout secondary to later infection at the site of injury.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This is a case report describing the clinical management of a single patient. This is not a research study, and, therefore, no Institutional Review Board approval was sought before submitting the article as the patient cannot be identified by publisher or readers.
Provenance and peer review Not commissioned; internally peer reviewed.