Article Text

Abstract
Background The Brain Injury Guidelines provide an algorithm fortreating patients with traumatic brain injury (TBI) and intracranial hemorrhage(ICH) that does not mandate hospital admission, repeat head CT, orneurosurgical consult for all patients. The purposes of this study are toreview the guidelines’ safety, to assess resource utilization, and to proposeguideline modifications that improve patient safety and widespreadreproducibility.
Methods A multi-institutional review of TBI patients was conducted. Patients with ICH on CT were classified as BIG 1, 2, or 3 based on the guidelines. BIG 3 patients were excluded. Variables collected included demographics, Injury Severity Score (ISS), hospital length of stay (LOS), intensive care unit LOS, number of head CTs, type of injury, progression of injury, and neurosurgical interventions performed.
Results 269 patients met inclusion criteria. 98 were classifiedas BIG 1 and 171 as BIG 2. The median length of stay (LOS) was 2 (2,4)days and the ICU LOS was 1 (0,2) days. Most patients had a neurosurgeryconsultation (95.9%) and all patients included had a repeat head CT. 370repeat head CT scans were performed, representing 1.38 repeat scans perpatient. 11.2% of BIG 1 and 11.1% of BIG 2 patients demonstratedworsening on repeat head CT. Patients who progressed exhibited a higherISS (14 vs. 10, p=0.040), and had a longer length of stay (4 vs. 2 days;p=0.015). After adjusting for other variables, the presence of epiduralhematoma (EDH) and intraparenchymal hematoma were independent predictors ofprogression. Two BIG 2 patients with EDH had clinical deteriorationrequiring intervention.
Discussion The Brain Injury Guidelines may improve resourceallocation if utilized, but alterations are required to ensure patientsafety. The modified Brain Injury Guidelines refine the originalguidelines to enhance reproducibility and patient safety while continuing toprovide improved resource utilization in TBI management.
- brain injuries, traumatic
- head injuries, closed
- practice guideline
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Traumatic brain injury (TBI) is responsible for the utilization of vast healthcare resources, with an estimated cost of $76.5 billion in 2010 in the USA.1 In 2013, TBI was diagnosed in more than 2.8 million emergency department (ED) visits and 282 000 hospital admissions.2 Most protocols governing patient care for TBI with intracranial hemorrhage (ICH) mandate an inpatient or intensive care unit (ICU) admission, a neurosurgery consult, and at least one repeat head CT scan.3–11 The allocation of resources is at the forefront of the current discussion regarding healthcare. Decreasing unnecessary hospital and ICU admissions, reducing consults of questionable utility and minimizing CT scans of limited clinical relevance are all potential sources for dramatic cost savings.
The Brain Injury Guidelines (BIG) provide a method to stratify and treat mild TBI. BIG 1 injuries are <4 mm subdural hematomas (SDH), <4 mm epidural hematomas (EDH), <4 mm intraparenchymal hemorrhages (IPH) or “trace” subarachnoid hemorrhages (SAH). Patients with BIG 1 injuries are observed for 6 hours in the emergency department (ED) and do not receive a planned neurosurgery consultation or repeat head CT. BIG 2 injuries are 4 to 7 mm SDH, 4 to 7 mm EDH, 4 to 7 mm IPH or “localized” SAH. These patients are admitted to the hospital, but do not receive a neurosurgery consultation or a repeat head CT. BIG 3 injuries are >8 mm SDH, >8 mm EDH, >8 mm IPH, or “scattered” SAH and are managed with admission, a neurosurgery consultation and at least one scheduled repeat head CT.12 13 The complete criteria by which patients are categorized as BIG 1, 2, or 3 are outlined in the definitions section below.
This algorithm represents a departure from the standard practice at most centers. The potential cost savings for a healthcare system that adopts this strategy is immense. In addition to the direct financial benefits, reallocating hospital beds, optimizing neurosurgeon time-utilization, and increasing CT availability divert limited healthcare resources toward patients who are more likely to benefit from their use.
The BIG do have some drawbacks. The guidelines have only been validated at the institution at which they were developed. Although both prospective and retrospective analyses have been completed, further independent validation is required before the guidelines can be widely implemented.12 13 The BIG are often vague in defining specific aspects of the management algorithm. Any attempt to implement these guidelines would require speculation regarding several of the pertinent components making uniform, widespread, utilization impossible.
The purpose of this study is to analyze accuracy of the BIG at identifying ICH with low risk of progression and to assess the resource savings that may follow implementation of these guidelines. Additionally, a modified version of the BIG that are generalizable and improve patient safety is proposed. The hypothesis behind this analysis was that the BIG are accurate at identifying low risk patients with ICH, can lead to a significant improvement in resource allocation if implemented, and that with some clarification, they can be widely put into practice.
Methods
A retrospective analysis was performed of all patients with TBI from January 1, 2014 to December 31, 2016 admitted to one of three trauma centers, UCHealth Memorial Hospital Central in Colorado Springs, CO, Loyola University Medical Center in Maywood, Illinois, and Medical Center of the Rockies in Loveland, CO, using the trauma registry and electronic medical record at each respective institution. Patients greater than 18 years old with findings of an ICH or skull fracture on initial head CT scan and no abnormalities on neurologic examination were classified as BIG 1, 2, or 3 based on the BIG.12 13 An abnormal neurologic examination was defined as a Glasgow Coma Scale score (GCS) of 12 or less at admission or the presence of focal neurologic or abnormal pupillary findings on examination. This definition is consistent with the BIG. A review of CT scan imaging was performed by the contributing authors. Progression on CT scan was defined as an increase in the size of the ICH consistent with the definition used in the BIG. Interpretation of unclear aspects of the BIG was performed by the contributing authors. Patients with more than one type of intracranial injury were classified according to the most severe injury rather than as BIG 3 as in the original guidelines. BIG 3 patients were excluded from further analysis as the care of these patients does not deviate from the current standard of care at each institution. Additional exclusion criteria included penetrating injuries, patients who presented greater than 48 hours after injury, patients transferred from outside hospitals without available images from initial CT, previous brain operation, intubation within the first 6 hours of presentation, withdrawal of care or comfort measures initiated within the first 48 hours of presentation, patients with missing values, and patients who did not receive a repeat head CT. Variables collected using the trauma registries and electronic medical record at the respective institutions included demographics, admission GCS, admission neurologic and pupillary examination findings, ethyl alcohol level, anticoagulation or antiplatelet therapy, Injury Severity Score (ISS), hospital length of stay (LOS), ICU LOS, number of repeat head CTs, type and severity of injury, presence of radiographic and/or clinical progression of injury, and neurosurgical interventions performed.
Definitions
BIG 1—SDH≤4 mm, EDH≤4 mm, IPH≤4 mm, SAH-trace, no skull fracture, no anticoagulation/antiplatelet therapy, or no intraventricular hemorrhage (IVH).
BIG 2—SDH 4 to 7 mm, EDH 4 to 7 mm, IPH 4 to 7 mm, SAH-localized, non-displaced skull fracture, no anticoagulation/antiplatelet therapy, or no IVH.
BIG 3—SDH≥8 mm, EDH ≥8 mm, IPH≥8 mm, SAH-scattered, displaced skull fracture, on anticoagulation/antiplatelet therapy, or an IVH.
Statistical analysis
Categorical variables were compared using χ² test or Fisher’s exact test where appropriate and presented as proportions. Continuous variables were analyzed using Wilcoxon Rank Sum test and presented as median (IQR). To explore the relationship between significant covariates, variables with p<0.2 on univariable analysis were selected for model building. Logistic regression with exact conditional analysis was used to account for correlated data and intrafacility clustering. Statistical analysis was performed using SAS V.9.4 (SAS Institute, Cary, North Carolina) with significance was established at p<0.05. Institutional Review Boards at each respective institution approved the study.
Results
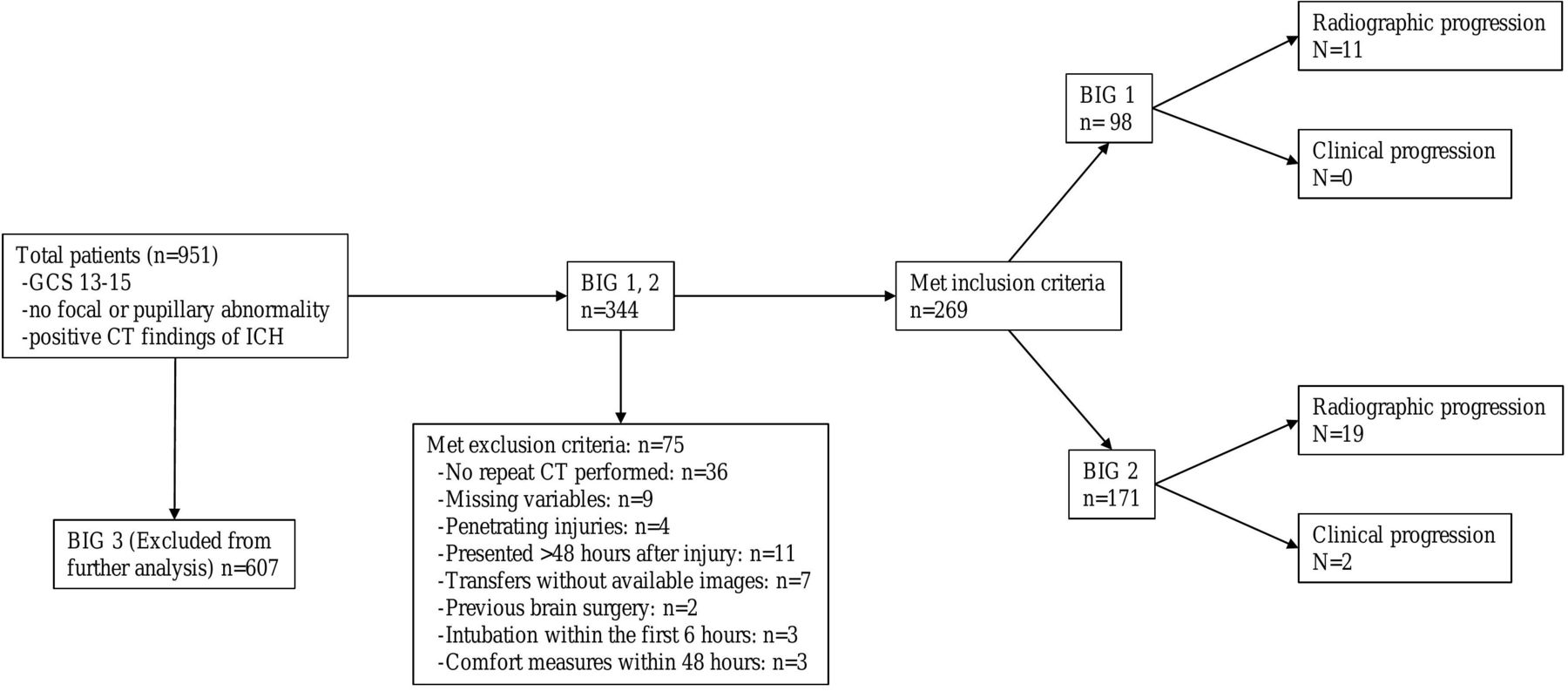
During the 36-month study period, 951 patients met the initial inclusion criteria. A total of 607 patients were classified as BIG 3 and were excluded from further analysis. Of the remaining 344 patients, 75 met additional exclusion criteria (figure 1). A total of 269 patients were included in the final analysis, 98 were classified as BIG 1, and 171 were classified as BIG 2 (figure 1). Overall, the median age was 53.0 (31.0 to 67.1) years old. The patient population was predominantly male (55.3%) with a median ISS of 10 (8 to 16). The median LOS was 2 (2 to 4) days and the median ICU LOS was 1 (0 to 2) day. The vast majority of patients had a neurosurgery consultation (95.9%) and all patients included had a repeat head CT. The most common findings on CT were SDH (51.3%) and SAH (52.0%). Few clinical differences were seen between the study cohorts (table 1).
Demographics of total study and BIG groups

Study eligibility. BIG, Brain Injury Guidelines; GCS, Glasgow Coma Scale score; ICH, intracranial hemorrhage.
BIG 1 patients spent a median of 3 (1 to 4) days in the hospital days per patient. Of those hospital days, the BIG 1 cohort spent a median of 1 (0 to 2) ICU day per patient. The BIG 2 cohort a median of 1 (0 to 2) day in the ICU per patient.
All patients included received an initial head CT scan and at least one repeat head CT scan. Some patients received more than one repeat head CT and a total of 370 repeat head CT scans were completed. This represents 1.38 repeat CT scans per patient after the initial scan at admission. Overall, 30 patients had worsening radiographic findings on repeat head CT. By study cohort, 11.2% of BIG 1 patients and 11.1% of BIG 2 patients had radiographic progression. Patients with radiographic progression had similar demographics to those that did not progress but, were more severely injured, more likely to have an EDH, and more likely to have an IPH. Patients who progressed had a longer ICU LOS and a longer overall LOS (table 2). Univariable and multivariable logistic regression identified EDH and IPH as independent predictors of progression (table 3).
Comparison progression to no progression (increased hemorrhage)
Logistic regression univariable and multivariable analysis for independent predictors of radiographic progression of injury
Two BIG 2 patients had clinical decompensation and required neurosurgical operative intervention. Both patients had EDH and a worsening of neurologic examination as well as expansion of the EDH on repeat head CT. No other BIG 1 or 2 patient had a worsening of neurologic examination or required operative intervention.
Discussion
The BIG attempt to deliver more efficient care by limiting hospital and ICU admissions to patients who truly require them, decreasing unnecessary radiographic testing, and reserving specialist consultation for appropriate scenarios. This study attempts to assess how accurate the BIG are at identifying patients that may be eligible for this less aggressive management algorithm. The findings of this project suggest that EDHs have a high risk of both radiographic and clinical progression. Those patients that had clinical decompensation were both EDHs who were identified on examination and progressed within the first 24 hours of admission. Both required neurosurgical intervention. Otherwise, the original BIG were accurate at identifying low-risk patients with mild TBI at the three institutions participating in this project.
Currently, most patients who suffer a TBI with ICH will be admitted to the hospital. Under the BIG, patients who fall into the BIG 1 category do not require an inpatient admission and instead are discharged after a 6 hour observation period in the ED. Utilization of these guidelines during the study period could have led to a 98 fewer admissions with a potential decrease of 339 hospital days for those patients. This represents a tremendous source of potential cost savings if the guidelines were widely implemented.
The concept that neurosurgical consultation is not warranted in all patients with traumatic ICH is not new.5 6 8–10 14 The question as to which patients need a neurosurgical consultation and which patients can be managed solely by trauma surgeons has been difficult to answer.9 10 14 The BIG offer a framework by which this question can be systematically approached.12 13 Neurosurgeons would be free to focus on those patients that are most likely to need their operative services, avoiding costly and time-consuming consults for patients with relatively minor head injuries.
The question of whether all patients with mild TBI (GCS 13 to 15) and ICH need a repeat head CT has been posed for several years.3 7 9 11 15–20 This emerging literature suggests that the selective use of repeat CT scan in TBI is safe, but a consensus as to which patients do not require repeat CT has not been reached. Using GCS alone to estimate the severity of TBI is inadequate.21 The BIG use the size of ICH to analyze the need for scheduled repeat head CT and save repeat head CT for the largest volume ICH or for patients that have a change in neurologic examination. Implementation of the BIG during the study period would have resulted in 370 fewer CT scans which is an average of 1.38 repeat CT scans per patient. Widespread adoption of these guidelines has the potential to significantly impact the vast sums spent on TBI each year, merely from the decrease in CT scans obtained.
Improvements in resource allocation are of no utility if patient safety is not preserved. When considering TBI, the potential sequelae of missed progression of injury are so devastating that they must be kept to an absolute minimum. This retrospective analysis found that more stringent criteria with regard to EDH are warranted to ensure that injury progression is not missed. Additionally, the BIG lack clarity regarding several of the components. Any attempt to implement the guidelines across institutions would require speculation as to how to define some important aspects of the algorithm.12 13
Proposal of modified Brain Injury Guidelines
Based on the findings of this study and an assessment into the reproducibility of the original BIG, the modified Brain Injury Guidelines (mBIG) are proposed (figure 2). These modifications to the original guidelines were created by a combined effort from the trauma and neurosurgery departments at the participating institutions. Overall, the modifications can be categorized as changes to either increase patient safety or to allow for consistent, widespread utilization of the guidelines.

{kind=link}
{kind=link}
Modified Brain Injury Guidelines. BIG, Brain Injury Guidelines; ED, emergency department; EDH, epidural hematoma; EtOH, blood alcohol level; fx, fracture; GCS, Glasgow Coma Scale score; ICH, intracranial hemorrhage; IPH, intraparenchymal hematoma; IVH, intraventricular hemorrhage; mBIG, modified BIG; SAH, subarachnoid hemorrhage; SDH, subdural hematoma; TBI, traumatic brain injury.
The original BIG retrospective analysis found radiographic progression in 0% of BIG 1 patients and 2.6% of BIG 2 patients.12 The current study found the rate of radiographic progression to be much higher at 11.2% for BIG 1 patients and 11.1% for BIG 2 patients. Although the rate of radiographic progression was higher in this analysis, radiographic progression alone was not clinically significant. This is consistent with the findings of the original BIG retrospective review. Deterioration on neurologic examination was a much more important clinical indicator.
The most critical component of the mBIG that differs from the original BIG is that all EDH are classified as mBIG 3. This study suggests that EDH carry an unacceptable risk for clinical progression of injury. Two patients with EDH, both of whom qualified as BIG 2, had both clinical and radiographic decompensation and required decompressive craniectomy. Although there is debate as to the utility of craniectomy, these are the only BIG 1 or 2 patients that experienced a deterioration in neurologic examination.22–25 In addition, patients with EDH were more than eight times more likely to have a radiographic progression of CT findings on multivariable analysis, although this study did evaluate a small sample size. In the interest of patient safety, the mBIG classify any EDH as a mBIG 3.
The original BIG classify any patient taking aspirin, warfarin, or clopidogrel at the time of injury as BIG 3. In addition to those three medications, the mBIG include direct oral anticoagulants (DOACs), including oral factor Xa inhibitors and direct thrombin inhibitors, as an indication to classify the patient as mBIG 3. DOACs are becoming more commonplace and the risk of progression of hemorrhage after ICH in patients taking these medications is not clearly understood but may be significant.26–28
In order for any set of guidelines to be implemented, they must be generalizable across different providers and institutions. Several of the definitions used in the original BIG require clarification to be widely implementable.
The original BIG define SAHs as “trace,” “localized,” or “scattered” to qualify as BIG 1, 2, or 3, respectively.12 These definitions are vague and cannot be consistently applied without clarification. The mBIG propose new definitions based on the number of involved sulci and hemispheres that are easily reproducible and can be consistently applied across institutions and practitioners.
The original guidelines suggest that “intoxication” excludes a patient from consideration as BIG 1; however, they do not define intoxication. The mBIG define intoxication as a blood alcohol level of 80 mg/dL or greater, consistent with the legal limit for driving in the USA.29 Due to the lack of a reliable timeline from ingestion to positive test in patients with positive urine toxicity screening, use of other illicit drugs was not considered an indication to exclude a patient from consideration as an mBIG 1. Patients are required to have a normal neurologic examination to be classified as mBIG 1 or 2, as in the original guidelines. Any patient under the influence of drugs with an abnormal neurologic examination would be considered mBIG 3 due to altered mental status.
Treatment algorithms in the original BIG are clear for BIG 1 patients, but are lacking for BIG 2 patients. The original guidelines merely state that BIG 2 patients should be admitted to the hospital without a repeat head CT or neurosurgical consultation.12 13 There is no discussion of the duration or location of admission. The mBIG algorithm clarifies that mBIG 2 patients are admitted for 24 to 48 hours with neurologic assessments every 2 hours for the first 6 hours and every 4 hours thereafter. Since no patient in this review experienced a clinical decompensation other than those with EDH, 24 to 48 hours of observation is sufficient to ensure clinical stability and to allow for discharge as part of the team’s normal workflow. Unlike the original guidelines, all mBIG 1 and 2 patients must have a GCS of 15 to be discharged. As with the original guidelines, any deterioration in neurologic examination immediately elevates any patient classified as mBIG 1 or 2 to the mBIG 3 arm of therapy with a repeat head CT, neurosurgical consultation, and hospital admission.
There are several limitations to this study. As a multicenter retrospective, database study, it is subject to the limitations inherent to this type of study, including a reliance on correct coding and the variability in patient management across providers and institutions. The analysis into resource utilization is limited due to the dearth of data on true hospital costs. Ideally, the hospital costs incurred by these patients could have been directly analyzed and reported; however, this information is not readily available for publication. Without reliable data regarding average hospital costs, assigning monetary values to potential cost savings is not possible. Additionally, concomitant injuries undoubtedly played a role in some hospital and ICU admissions, but the ability to accurately quantify that role is limited in a retrospective review. Clinical decision making processes at the time of admission, hospitalization, and discharge are not always readily apparent when looking retrospectively. This project highlights the potential for great cost savings with the implementation of these guidelines, but the exact cost reduction cannot be accurately analyzed from a retrospective review.
Conclusion
The BIG provide a novel and exciting proposition to alter the manner by which TBI with small to medium volume ICH is managed. Implementation of the guidelines has the potential to provide tremendous cost savings should they be widely used. An external review of these guidelines found that the original guidelines are reasonably accurate at identifying low-risk patients with ICH; however, some minor alterations are necessary. The mBIG refine the original BIG to enhance patient safety and to clarify some definitions, making universal and widespread implementation easier. A multicenter, prospective trial is needed to validate the mBIG and for the potential cost savings to be realized.
References
Footnotes
Contributors All authors have made substantial contributions to study design, drafting, critical revision, and approval of the final article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This project was approved by the Institutional Review Boards at UCHealth (#17-6101) and at Loyola University Medical Center (#209254) prior to beginning data collection.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. This is not a clinical trial and data are not available.