Article Text

Abstract
Background Vascular injuries in combat casualty patients are common and remain an ongoing concern. In civilian trauma centers, vascular surgeons are frequently available to treat vascular injuries. Within the military, vascular surgeons are not available at all locations where specialty expertise may be optimal. This study aims to determine if a visiting surgeon model, where a general surgeon can visit a civilian trauma center, would be practical in maintaining proficiency in vascular surgery.
Methods All vascular trauma relevant cases done by any surgical service were identified during a 2-year period at Saint Louis University Hospital between October 1, 2016 and September 30, 2018. These included cases performed by trauma/general, thoracic, vascular, and orthopedic surgery. Predictions on the number of call days to experience an operative case were then calculated.
Results A total of 316 vascular cases were performed during the time period. A surgeon on call for five 24-hour shifts would experience 2.1 urgent vascular cases with 95% certainty. To achieve five cases with 95% certainty, a surgeon would have to be on call for 34 24-hour shifts.
Discussion A visiting surgeon model would be very difficult to maintain to acquire or maintain proficiency in vascular surgery. High-volume trauma centers, or centers with significant open vascular cases in addition to trauma, may have more reasonable time requirements, but would have to be evaluated using these methods.
Level of evidence Economic and value-based evaluations, level II.
- general surgery
- education
- vascular system injuries
- war-related injuries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Military trauma is significantly different from civilian trauma, with different wound patterns and different resources for the deployed surgeons.1–6 Surgical skill maintenance is a top priority within the military medical community. With active-duty, memory-of-combat casualty care fading when combat operations eventually cease, the ability to maintain a certain degree of surgical readiness will become even more of an issue. Options to train and maintain skills will be critically looked at. One option that has been used is the visiting surgeon model, where surgeons visit civilian institutions to obtain combat casualty care relevant skills. One combat casualty skill that will be in high demand due to battlefield prevalence will be vascular surgery skills.7
Previous research has suggested that a visiting surgeon method to maintain currency would not be prudent to obtain vascular surgery competence and readiness.3 A limitation to this previous study was that only procedures performed by vascular surgeons were counted. Similar trauma procedures can be performed by multiple surgical specialties and may be available for educational and military readiness purposes. To evaluate the potential for other services to supplement the vascular readiness of deployed surgeons and make the visiting surgeon method viable, a level 1 trauma center’s vascular case load was reviewed and a predictive model applied.
Methods
After an institutional review board non-research determination, trauma data were reviewed to determine the number of vascular relevant cases performed at Saint Louis University Hospital between October 1, 2016 and September 30, 2018. Saint Louis University Hospital is an American College of Surgeons level 1 trauma center. A vascular relevant case and subsequent organization was defined based on previously reported literature on military vascular trauma cases.7 Previous studies used the International Classification of Diseases (ICD)-9 codes, whereas the Saint Louis University Hospital data were recorded using ICD-10 codes. To ensure capture of all urgent vascular relevant cases using the new codes consistent with previous studies, all 11 389 surgical cases were manually reviewed and any ICD-10 codes that included an operation on fascia, procedures to expose vascular structures, or an operation directly on a vascular structure were included. Multiple services, including orthopedics, vascular surgery, trauma/general surgery, and thoracic surgery, performed vascular operations defined by ICD-10 codes.
Predictions to experience a relevant, urgent, operative vascular case were based on previous prediction models published for general trauma cases.8 Urgent was defined as happening within a calendar day, consistent with previous publications. An identical methodology was used to calculate the number of 24-hour shifts or the number of cases expected after a certain number of shifts in this study.
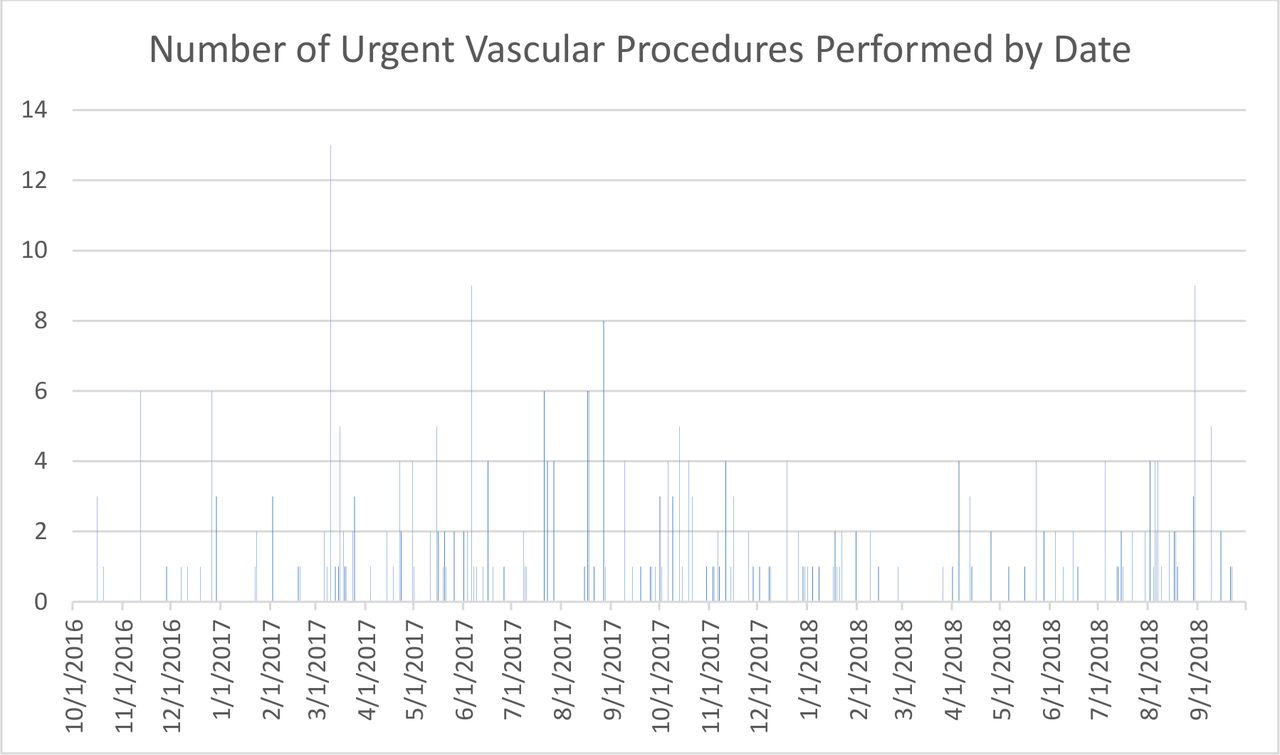
Operations may have seasonal patterns according to previously published research.8 To investigate whether there were significant differences in the volume of vascular operations among seasons, negative binomial regression was used to analyze the observed 2-year data with year, season, and season by year interaction in the model (figure 1). No statistically significant variables were found, and the remaining analysis was done without regarding seasonality.

{kind=link}
Timeline visually demonstrating the distribution of urgent vascular cases between October 1, 2016 and September 30, 2018.
Non-parametric bootstrap simulation methods were used to evaluate the distribution of the observed data set, which is assumed to represent the population and future years. Bootstrap samples do not make assumptions on a specified distribution, but instead follow the distribution of the observed data set; therefore, the sample sets are estimated based solely on the observed data, which we assume are representative of the population and future years. The observed data were resampled with replacement 10 000 times to estimate a sampling distribution.
The first scenario of interest was to predict the number of cases that are expected to be seen during 5, 10, 12, and 20 24-hour call periods. These were estimated using the bootstrap resampling methods. The second scenario of interest was predicting the number of 24-hour call days needed for a surgeon to experience 5, 10, and 20 urgent cases, also estimated using the bootstrap samples. The bootstrap simulation method is a commonly used, effective method in estimating statistics when there is not a clear analytical solution to a problem.
For scenarios estimating the number of cases to be expected during varying lengths of 24-hour call periods, the expected numbers, along with their respective 95% CIs, were predicted. For the second scenario requiring a preset number of cases and estimating how many 24-hour call periods would be required to see that number of cases, the number of call periods required was determined to be the number at which the minimum number of a one-sided 95% CI was the preset number of cases (5, 10, and 20). The upper bound of the one-sided 95% CI was estimated and determined to be the expected maximum number of days it would take to see at least 5, 10, and 20 cases with a 95% level of confidence. All analyses were done for vascular cases overall, cases that require a graft, and fasciotomy.
Results
A total of 316 urgent vascular procedures were performed at Saint Louis University Hospital between October 1, 2016 and September 30, 2018. The total number of cases performed by services other than vascular surgery was 105, representing a 49.8% increase over the 211 procedures performed by vascular surgery alone. The majority of procedures performed were on the upper and lower extremities; however, most procedures were not specifically related to the blood vessel itself, but mainly related to maneuvers to expose and assess the vascular supply. This exposure is considered to be a critical skill in vascular trauma. This is reflected in the number of unspecified procedures being high at 150 procedures (table 1). Direct procedures on named blood vessels were 109; of these, only 79 were either a graft or repair. Of the repairs, the vast majority were autogenous grafts, at 28.
Breakdown of vascular trauma cases by location and type performed at Saint Louis University Hospital by trauma/general surgery, orthopedic, and vascular surgery between October 1, 2016 and September 30, 2018
The number of 24-hour shifts required to achieve a specific number of vascular cases with 95% certainty was calculated for multiple sets of days. Additionally, the expected number of vascular cases after a set of potential number of shifts was calculated. Specific types of cases were also examined and calculations for these representative types of cases demonstrated (table 2). The listed number of 24-hour shifts and the number of cases are arbitrary and can be exchanged for different numbers for any future analyses and institutional comparisons.
Number of cases per several possible number of shifts and number of shifts to achieve a specific number of cases
Discussion
Military combat casualty care providers encounter many vascular injuries and require operative proficiency to manage these injuries in potentially austere situations.7 Although vascular shunts are not complex procedures and are often used in damage-control surgery, they are not permanent solutions. In situations of prolonged field care, vascular analogous tissue grafts will be required. Without trained and competent general surgeons or vascular surgeons to perform these tasks, the success rate of these operations can be expected to be low. Proficiency in vascular surgery is required for military surgeons.
This study demonstrates that a visiting surgeon model to experience urgent vascular trauma cases and develop proficiency through many repetitions is unlikely to be practical at some level 1 trauma centers, even if multiple services are contributing to the case total. The number of shifts required to obtain even a few cases with a near guarantee of likelihood is very high. The number of shifts does not consider time requirements for the visiting surgeon, such as travel time, rest, administrative tasks, and so on. Setting realistic numbers of required shifts, likewise, will result in such few cases that real proficiency should not be expected. If specific cases such as a graft repair or fasciotomies are predicted at Saint Louis University Hospital, the number of shifts would be astronomical just to obtain a handful of cases. This does not necessarily mean that all institutions may not be able to support a visiting surgeon model. Extending the definition of a vascular trauma case to other services increased the case pool by 49.8%. If another potential institution has very robust vascular trauma numbers, a similar increase in the case pool may make them viable. Another caveat to support the visiting surgeon model is the failure of this analysis to incorporate elective or non-elective open vascular procedures. Non-traumatic vascular cases may serve as a reservoir of near relevant cases for technical competence for non-vascular surgeons. Although the confounding factors such as distorted tissue planes and concomitant polytrauma may not be present, functional tasks such as vascular anastomosis, vein preparation, and so on would be similar and useful. This option may still not be practical as the number of open vascular cases drops relative to endovascular procedures.9 10 If pursued, careful analysis and predictability of an institution’s elective cases, along with impact on trauma skills, will have to be done. Without determining the relevancy of non-trauma vascular procedures to trauma skills, relevancy should not be assumed. Additionally, elective cases are often available at military inpatient facilities and potentially in the local community, making distant travel requirements unnecessary.
The military has not defined what a ready surgeon is. Despite multiple lines of effort dedicated to readiness and evidence that trauma skills diminish with disuse, a means of measuring capability and the effect of readiness programs to maintain it has not been completed.11 Although the visiting model may be impractical at Saint Louis University, what is shown is that a substantial number of vascular trauma procedures can be performed by other services. In this study 33% of the cases were not performed by vascular surgeons. This increase may be a common finding at multiple institutions and affect predictions made using these methods. If, for example, it could be determined that familiarity with vascular trauma techniques is all that is required for proficiency, perhaps as few as two vascular trauma cases over five 24-hour shifts is adequate. If familiarity is all that is required, it is likely that a visiting model may be appropriate at an institution such as Saint Louis University Hospital or more appropriately at a higher volume center.8
The idea to have a visiting surgeon exposed to trauma for a short time would seem on the surface to be a good idea. This would allow for a distinct time period to be set aside, enabling a surgeon to plan his life and clinical practice. Practically, however, this method of maintaining readiness may not be the best option. In multiple studies it has been shown that to have any guarantee of a substantial number of urgent trauma cases in several specialties, an inordinate amount of time would be required at any given location. The authors suspect the best option to achieve combat casualty care readiness would likely be embedding surgeons within civilian institutions. When embedded, military surgeons will be continually exposed to trauma and vascular cases. Although the total case numbers may never be high, both urgent and non-urgent cases may occur with enough frequency to allow for the development and maintenance of proficiency. Embedding military surgeons presents issues of reimbursement, military integration, and military career progression, which can all affect retention of skilled surgeons and cannot be addressed in this analysis. Military–civilian relationship issues can be mitigated, whereas the mathematics of trauma case loads cannot be effectively altered.
The weaknesses of this study include a likely high false positive rate of vascular procedures at this institution. This was due to inclusion of many cases that were simple exposure of vasculature or operation on an unnamed vessel and a manual review. Although methods to expose vasculature are important skills, they do not necessarily equate to the core vascular competency of shunting and repair, which would be most useful on the battlefield. Even with a high false positive rate, the number of shifts required to achieve a few cases with near guarantee is very high. We expect the number of truly open vascular repairs to be even less. An additional weakness is the lack of verification of probability. Accuracy tests of the methodology were done for trauma/general surgery and orthopedics and found that accuracy did depend on service, with orthopedics being less accurate.8 The accuracy of these predictions may not achieve 95% certainty, but the authors suspect the time requirements to achieve any guaranteed level of physician exposure would be prohibitive. Finally, this is a single-institution study. It is known that this institution has fewer trauma cases in general than other institutions, and if detailed analysis is done at other institutions more viable locations could be identified.8
This study does not address any method of gauging at what defines ‘competence’ in a specific skill set or what level surgical skills are currently at within the military general surgeon population. This is currently being addressed at high levels through the Knowledge Skills and Abilities project and others, but it has not been completed.12 The military may determine that familiarization with vascular surgery is all that is required. General surgery residency may be adequate to perform vascular skills at a familiarization level after the Accreditation Council for Graduate Medical Education (ACGME) minimum of 10 cases is reached in residency. In the combat casualty care population, where over 6.5% of the cases require vascular skills, being familiar with vascular surgery may not be adequate.7 If true proficiency and expertise are required, constant exposure and practice should be the standard. The best interest of soldiers is having care provided by those that excel above a minimal standard.
Conclusion
Gaining or maintaining proficiency in managing urgent, traumatic, vascular injuries cannot be expected with a visiting surgeon program. It may be theoretically possible at a location with a predictable and routine elective open vascular program in combination with high-volume trauma, but careful identification of centers would be required. The best option to maintain or gain proficiency would be embedding military surgeons in civilian centers for lengthy periods of time.
Footnotes
Contributors AH contributed to design, data gathering, interpretation, and writing. IQ contributed to data analysis and writing. KB contributed to data gathering. JG contributed to data interpretation and writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Air Force, the Department of Defense, or the US Government.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The research was done using data obtained after non-human research determination at Saint Louis University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Data can be obtained through the Saint Louis University Hospital Trauma Registry.