Article Text

Abstract
Injury is a major global health issue, resulting in millions of deaths every year. For decades, trauma registries have been used in wealthier countries for injury surveillance and clinical governance, but their adoption has lagged in low-income and middle-income countries (LMICs). Paradoxically, LMICs face a disproportionately high burden of injury with few resources available to address this pandemic. Despite these resource constraints, several hospitals and regions in LMICs have managed to develop trauma registries to collect information related to the injury event, process of care, and outcome of the injured patient. While the implementation of these trauma registries is a positive step forward in addressing the injury burden in LMICs, numerous challenges still stand in the way of maximizing the potential of trauma registries to inform injury prevention, mitigation, and improve quality of trauma care. This paper outlines several of these challenges and identifies potential solutions that can be adopted to improve the functionality of trauma registries in resource-poor contexts. Increased recognition and support for trauma registry development and improvement in LMICs is critical to reducing the burden of injury in these settings.
- accident prevention
- electronic health records
- public health
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Injuries kill approximately 4.8 million people a year and account for 10% of deaths worldwide—32% more than the number of deaths from tuberculosis, malaria, and HIV/AIDS combined.1 2 It is estimated that another 973 million people sustain injuries that require some form of healthcare,2 many of whom come from low-income and middle-income countries where the burden of injury is highest.
These numbers signal a global health crisis with devastating consequences, but it does not have to be this way. The majority of these injuries are preventable, and the strategies that aid in this regard are relatively inexpensive to implement and have been backed by rigorous scientific evidence. Dollar for dollar, injury prevention and mitigation have been shown to be the most effective way to address injury,3–5 and efforts to improve trauma care through quality assurance (QA) and quality improvement (QI) programs—which include activities such as “the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps”—(Quality assurance and quality improvement refer to “activities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps”.6) have also played a critical role in this regard.6–8
The establishment of trauma systems in high-income countries (HICs) tackles injury through both of these avenues. Trauma systems address the complex organizational problem of injury on the local, regional, and national scale through the coordination of numerous resources and services required for effective trauma management.9 They represent a coordinated public health response to injury control through prevention and treatment and have proven highly effective in reducing rates of injury morbidity and mortality in HICs.10–13
A critical first step in the development of these trauma systems is the collection and analysis of injury data in the form of a trauma registry.14 Trauma registries record information related to the injury event, process of care, and outcome of the injured patient.9 15 These data are vital to informed decision-making across the entire continuum of trauma care from injury prevention and mitigation to pre-hospital and hospital care, and finally rehabilitation and community care.
While HICs have built their trauma systems on the foundation of trauma registry data, LMICs have struggled to do the same.14 One of the major reasons is that implementing and operating a trauma registry is costly. Many hospitals in LMICs simply do not have the human or financial resources necessary to implement trauma registries in the same capacity as HICs. Consequently, the number of trauma registries in LMICs remains few, although this is slowly starting to change.16 Traditional resource challenges to trauma registry implementation in LMICs have recently begun to be answered with novel, cost-effective solutions that are, in many ways, leap-frogging some of the inefficiencies of trauma registries in HICs.17–20 As a result, trauma registry development in these countries has begun to grow.20 A 2019 scoping review of trauma registries in low-resource settings estimates that there are 27 trauma registries operating in low-income countries and 38 in middle-income countries.20 In just 7 years, these numbers have more than quadrupled for low-income countries and have doubled for middle-income countries.16
Although a trauma registry movement has undoubtedly begun to take hold in LMICs, emerging trauma systems have not benefited as greatly from trauma registries compared with HICs. We argue that numerous developmental and operational challenges such as missing or incomplete data, poor dissemination of registry findings, and large variations in what, how, and on who the data are collected have inhibited trauma registries in LMICs from reaching their full potential. Overcoming these barriers may represent one of the biggest opportunities in global public health given the magnitude of this injury crisis. The purpose of this paper is to therefore identify the most salient of these challenges and explore potential solutions to address them. We start with a brief history of trauma registry development in LMICs, then discuss the major barriers and opportunities for their use in informing injury prevention and mitigation efforts in the pre-injury phase, as well as improving quality of trauma care in the post-injury phase (figure 1).
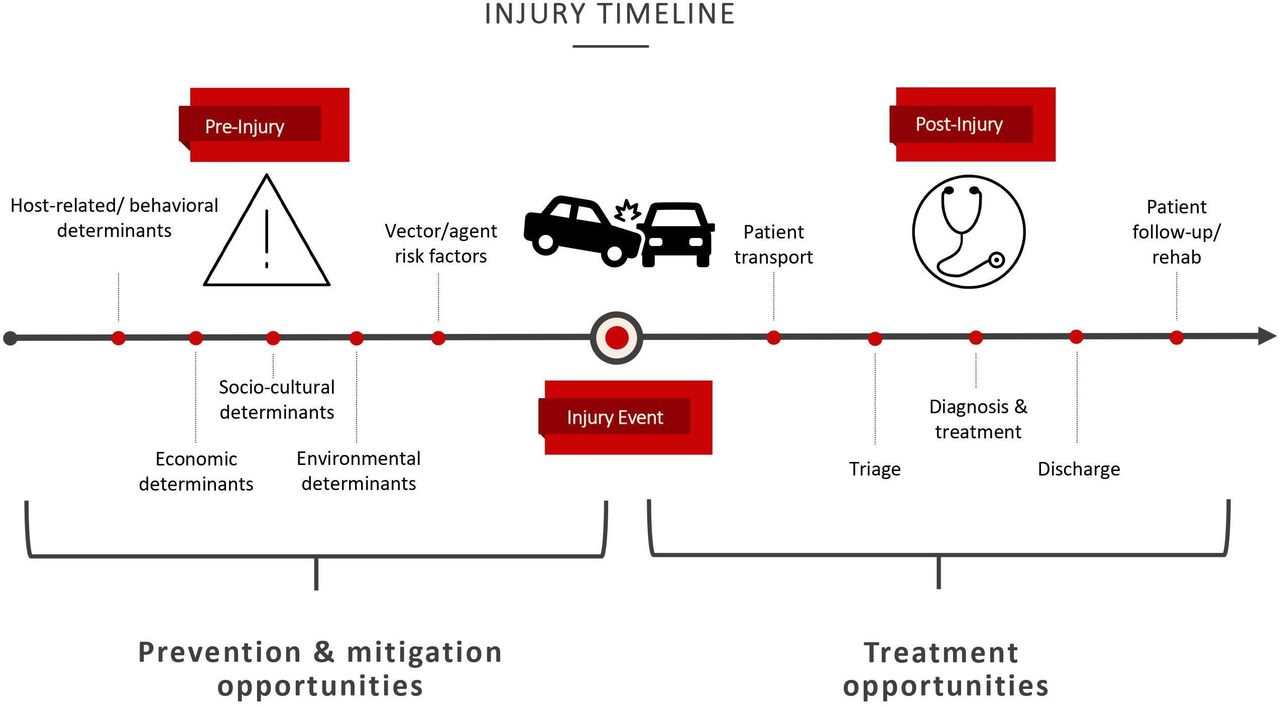
Injury timeline. This figure displays the three phases of injury (as informed by the Haddon Matrix). On the left side is the pre-injury phase, where a variety of interrelated factors can increase the risk of an injury event. Injury risk factors leading up to the injury event can be targeted and addressed through injury mitigation to reduce the magnitude of severity of the injury, or through injury prevention to stop it from happening altogether. On the right side is the post-injury phase. The typical process of care for an injured patient is shown. Measures to improve quality of trauma care (ie, quality assurance, quality improvement) can be taken at every step during the process of care to improve injury outcome. Data from trauma registries help to inform these above efforts to tackle injuries both before and after they occur.
However, before we begin, we must acknowledge our biases as researchers hailing from mostly HICs writing about the healthcare systems of LMICs. While our arguments are built from the foundation of research coming out of LMICs on trauma registries, we recognize that we cannot possibly have all the answers to this pressing problem without involving the voices of experts from each of these LMICs. Nor can we fully know and account for the nuances of such diverse systems. Instead, we hope that this paper can serve as a jumping off point for additional research and funding of trauma registries in LMICs by synthesizing and critically assessing the body of knowledge that has emerged from this field so far.
Trauma registry development in LMICs
In the early 1990s, several fixed-trial studies began to explore injury epidemiology, patient care, and outcome in several LMICs in Africa. However, it was not until 1999 that the first ongoing trauma registry was developed at Mulago hospital and Kawolo hospital in Uganda as part of an effort to establish a national injury surveillance system.17 21 This registry differed from its high-income counterparts in two key ways. First, the registry only collected the minimum number of variables it deemed necessary to meet its objectives. Given that many hospitals in LMICs are understaffed, this innovation has since proven to be an essential time-saving strategy for prospectively kept registries, helping to reduce the time and energy clinicians or other health professionals would spend collecting data. Second, the registry adopted a new, validated injury severity scoring tool, called the Kampala Trauma Score (KTS), which differs from more commonly used scores like the Injury Severity Score (ISS) or Revised Trauma Score (RTS). The ISS and the RTS have important limitations in lower-resource settings such as complex calculations and age specifications. The KTS on the other hand is much simpler to calculate and is also applicable to all ages—both of which are particularly well suited for LMIC environments where healthcare worker time is at a premium and pediatric hospitals are uncommon.17
Together, these adaptations have allowed the registry to flourish in an environment where both financial and human resources are limited and has paved the way for other registries to follow suit. In the years since, a grassroots movement has evolved, with more hospitals in LMICs looking to develop their own trauma registries in ways that confront the unique barriers inherent to these countries. Yet, several facets of these registries have limited their full potential.
In the following sections, we explore two principal outcomes of trauma registries—(1) injury prevention and mitigation, and (2) quality of trauma care—and the challenges and opportunities associated with them (table 1). While we recognize that trauma registry development and implementation in LMICs has numerous barriers, we have chosen to focus our discussion on those roadblocks that are common across many contexts and specifically inhibit the potential of trauma registries to develop effective injury mitigation and prevention strategies.
Challenges and opportunities to maximizing trauma registry potential in LMICs
Injury prevention and mitigation
Several challenges exist to improving the potential of trauma registries with regards to informing injury prevention and mitigation. Two major issues include the type of data being collected and the ways in which the findings from the trauma registry are disseminated. This section outlines these challenges and proposes several solutions to address these issues.
Challenges
A survey of the literature on trauma registries in LMICs indicates that over half of all papers published that use data extracted from a LMIC trauma registry focused on the injury epidemiology of incoming trauma patients.16 20 Such information forms the basis for injury prevention and mitigation. However, in many cases the data being collected (eg, age, sex, occupation… etc) only superficially characterizes the burden of injury in a region.20 Other information such as where the injury occurred or the type of activity the individual was engaged in at the time of the injury are collected much less frequently. However, these are the questions that provide the type of information needed for a much more nuanced understanding of injury risk and, subsequently, the injury prevention and mitigation measures that can target these risks in the pre-injury phase.
Furthermore, injury prevention and mitigation initiatives targeting the pre-injury phase require that such knowledge be translated and disseminated to the right stakeholders. Arguably, publishing results of injury epidemiology in the scientific literature is one way to disseminate these findings. However, more often than not, the divide between evidence and policy in LMICs remains large.22–24 For some trauma registries, government instability and a rotating cast of stakeholders within the respective Ministry of Health have made it challenging to disseminate their findings, especially if the value of injury surveillance research needs to be re-cultivated among the new cohort or if authorities only want results that confirm their administrative or political performance.25–27 For other registries, especially those strongly driven by foreign collaborators, there is a possibility that publication in the scientific literature is given higher priority than efforts to disseminate results more locally.25 28 The “publish or perish” paradigm retains a strong hold over many academic researchers that may, in some cases, overshadow efforts to disseminate the data with local stakeholders. Regardless of reason, failure to translate or disseminate findings from the trauma registry to a receptive audience represents a large missed potential for developing evidence-based preventative strategies in these settings.
Opportunities
Injury epidemiology has been a foremost focus of trauma registries in LMICs as evidenced by the high percentage of research articles published on the subject.16 20 Characterizing the burden of trauma on a local scale is vital for improving resource allocation and preparedness in hospitals.15 It is also the first step in identifying vulnerable groups of individuals who are at a higher risk for injury, the types of injury most prevalent among these groups, and the environments that are most conducive to injury. However, to inform injury prevention and mitigation strategies, research on injury epidemiology needs to dig deeper than traditional statistical foci. Questions regarding where injuries most frequently occur, what the major risks (behavioral, socioeconomic, cultural… etc) associated with injury are, and how these risks differ between groups are essential. This type of information can allow us to go beyond simple characterization of the trauma burden to a more nuanced understanding of the injury epidemic, helping to form the basis of evidence-based prevention and mitigation initiatives.
While the use of minimal data is expected in resource-constrained settings, the inclusion of a few additional fields regarding the injury event could allow for a more in-depth analysis and, subsequently, prove more useful for informing injury prevention and mitigation strategies. In particular, the use of spatial data to identify injury hotspots within the context of the built environment has potential to be especially beneficial for informing prevention efforts.29–31 For example, in rural Kenya, a health center–based injury surveillance system that incorporated GPS data was able to identify environmental correlates at the locations of injuries through geographic information systems (GIS) software and analyses.31 Distance to major roads proved to be a major determinant of injury in this area. Another study used spatial data to identify and map the main hotspots of injury for patients reporting to Groote Schuur Hospital in Cape Town, South Africa.18 The analysis identified the informal townships surrounding the city as the areas where injury most frequently occurs, suggesting a strong link between injury rates and poverty.
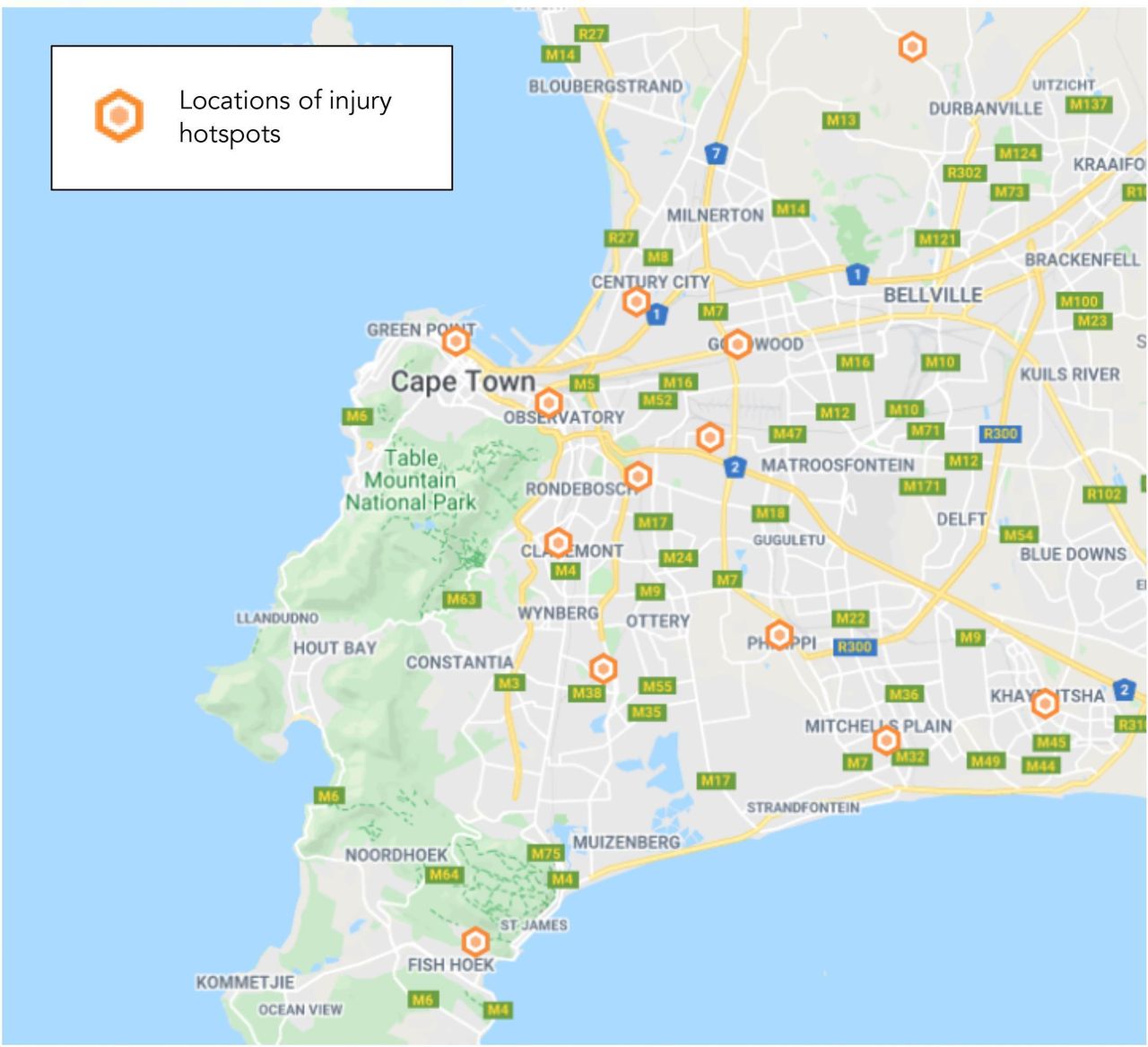
While GIS is a powerful way to analyze data, software can be costly—as are the backend requirements including server space, processing power, and human resources to perform the analyses. However, cheaper—and sometimes even free—options are increasing in popularity, helping resource-constrained trauma registries to capitalize on such tools. A pilot study at Groote Schuur Hospital in Cape Town, South Africa sought to show the utility and feasibility of free alternative methods using GeoWeb applications, which run similar injury-focused analyses. In particular, the study showed how hotspot mapping using these free applications can be used to explore patterns in the spatial distribution of injury at multiple scales, as well as visualize patterns of patient referral from surrounding healthcare facilities (figure 2).32

{kind=link}
{kind=link}
Hotspot mapping. This map identifies injury hotspots from data collected by the Groote Schuur Trauma Registry in Cape Town, South Africa. This map was adapted and simplified from the original,32 which was created using BatchGeo—an inexpensive GeoWeb application. Open-source report generators that incorporate aspects of spatial analysis can also be used to create similar maps reducing both the time and expertise needed for such efforts.
Equally important in shaping prevention efforts is the responsibility of trauma registries to disseminate these findings to receptive stakeholders. Peer-reviewed publication is an important form of communication. However, if findings are to be applied locally, reports to government and select community-based organizations should also be prioritized. Regular reporting on the trauma registry data is a means of building relationships with potential policy-makers and administrators. Identifying and establishing relationships with the right stakeholders (ie, those that have the power to effect change and institute preventative action) is just as important. The Ministry of Health or other regional forms of government may be natural partners for the dissemination of registry results. However, trauma registry stewards should also consider community-based organizations (CBOs) or civil service organizations (CSOs), especially in areas where politics and governance are turbulent and prone to change. Prior research in Uganda has highlighted these organizations as key stakeholders in knowledge translation efforts, as they are well situated to represent and advocate for the communities they serve.33 Moreover, because of their position in these communities, CSOs and CBOs often have a unique understanding of how prevention and mitigation initiatives would most effectively be implemented given the social, economic, and cultural context of their communities and mobilize resources accordingly.33 34 Finally, reports and analyses should be communicated to these stakeholders in a manner that can be easily understood and acted on. Tools like GIS software or GeoWeb applications mentioned previously can serve alongside graphs and other visuals as an important way to communicate injury data in an easily interpreted format, helping to bridge the gap between researchers and stakeholders more effectively.32 Development of an open-source report generator that works with any of the standard databases being used would also help facilitate this, greatly reducing the time and energy needed to create the maps and graphs included in each report.
Quality of trauma care
Aside from challenges affecting the potential of trauma registries to inform injury prevention and mitigation strategies, there also exists barriers impeding the potential of trauma registries in LMICs for use in improving quality of trauma care. Two such examples are missing or incomplete data and lack of trauma registry standardization. This section discusses these challenges and proposes several solutions to address these issues.
Challenges
Regardless of context, missing or incomplete data seems to be among the most commonly reported challenges of trauma registry operation in LMICs.18 35–42 Moreover, it seems to be most problematic for data collected on the process of care and outcome of the injured patient in the post-injury phase, and least problematic for data collected on demographics and the pre-injury phase.35–37 42 For example, in the implementation of a femur fracture registry at Komfo Anokye Teaching Hospital in Ghana, the percentage of completed data was highest (>77%) for those fields collected soon after patient admission (ie, pre-injury phase data), such as gender, home region, date of injury, and mechanism of injury. However, for data fields related to treatment and discharge, collection rates dropped substantially (<50%); data fields related to outcome were not collected at all despite being present on the form.37 In another study that examined the descriptive statistics of patient data collected by the Ugandan Trauma Registry, the percentage of missing data was consistently higher for all diagnostic and outcome-related fields compared with demographic or injury event-related fields.36 In one extreme instance for this trauma registry, the field “surgical procedure performed” was recorded less than 32% of the time.36
While data can be missing for several reasons, research has shown that certain fields fare worse than others. Fields with free-text options or long checklists are less likely to be completed in time-pressed situations compared with binary data fields.43 44 Furthermore, fields that are collected closer to the end of a patient’s stay compared with the beginning often show reduced rates of completion given the challenges some settings face in tracking patient flow through the hospital—an issue clearly demonstrated in the examples previously mentioned.27 37 45 46 Finally, fields that require the data collector to possess a certain level of training or education to answer also fare poorly compared with more basic fields.26 37 42 Interestingly, fields related to the care and outcome of the injured patient, which are typically collected further along in a patient’s stay and often rely on medical knowledge for accurate collection, are most often omitted.36 37 That is, fields that would help inform QA/QI efforts are those that are the least consistently collected.
One of the consequences of missing data is reflected in the publishing record of many of these trauma registries. In a 2019 scoping review on trauma registry implementation and operation in LMICs, it was found that of the 107 papers published that used the data extracted from a LMIC trauma registry, 58 papers used the data for injury epidemiology studies, 18 used the data for internal comparison studies, another 18 used the data for external comparison studies (ie, benchmarking), and just 5 used the data for quality improvement studies.20 Similar ratios of publication content were found in an earlier study by O’Reilly et al in 2013.47 While a focus on injury epidemiology is certainly important, the paucity of research on benchmarking trauma care and, to an even greater extent, evaluating the quality of trauma care indicates an overwhelming potential for refining trauma care efforts that is being left untapped.
Missing data is only partly to blame for this research gap. Another key consideration has to do with the heterogeneity of trauma registries being developed in LMICs. As trauma registry development in these contexts is largely the result of grassroots efforts that are not monitored nationally or internationally (as opposed to the typical government mandated nature of HIC trauma registries), there have been no standards or best practices in place for the collection of data in these settings. Patient eligibility criteria for the registry, how fields are defined, and the injury severity scoring measures used all vary widely.20 47 When these decisions are kept consistent within the registry, internal benchmarking and quality improvement analyses are unaffected. However, when these differ between trauma registries, valid external benchmarking becomes challenging and thereby limits an important source of information on the quality of trauma care being provided.
Furthermore, the choices surrounding what fields a trauma registry collects and the quality indicators they measure are also highly variable, and often context driven. Use of a minimal dataset has proven to be an advantageous adaptation of trauma registries in LMICs, greatly reducing the time needed for data collection. However, minimal data collection necessitates careful consideration of which fields “make the cut”. Surprisingly, no public resource is readily available to help fully navigate these choices. While the WHO’s Injury Surveillance Guidelines have reportedly been used by many trauma registries in LMICs, it only guides choices on the fields that should be collected to assess injury epidemiology, with little information on the fields that should be collected to assess pre-hospital and hospital care or patient outcome.48 Some papers have tried to fill this gap by documenting the fields being collected by other existing trauma registries in these contexts; however, no consensus has been reached to define which fields should comprise this dataset and how such fields should be defined.20 47
Opportunities
Recently, the collection of data electronically through iPads or tablet devices for trauma registry purposes in LMICs has increased. Among numerous other benefits, this new method of electronic charting has been shown to improve compliance with data entry and facilitate better patient tracking as they move throughout the hospital.29 49 In one case, missing data were reduced by 25% on average from a previous paper-based charting system.29 Data collectors have found that the apps developed for these purposes are easier and quicker to populate compared with paper-based methods, often making use of convenient drop-down menus or prompts that remind the user of a blank field.29 49 50 Furthermore, the capability for a system administrator to view data-entry in real time has improved quality control efforts and, consequently, data compliance.49 Likewise, since the data collected are already in a digital format (and not handwritten), it eliminates the need for someone to manually enter the data into the trauma database, greatly improving efficiency.
In 2013, Groote Schuur Hospital in Cape Town, South Africa implemented the electronic Trauma Health Record (eTHR)—an app that allows clinicians to collect and securely upload data to a concurrent trauma database. In addition to improving data capture and being a timelier means of data collection, the eTHR has allowed Groote Schuur Hospital to capture a much greater number of fields in the same amount of time, where previously only a minimum dataset was collected.19 29 While obviously of benefit to trauma QI initiatives, such a capability can also be of help in going beyond the superficial characterization of the injury burden that was discussed previously with reference to injury prevention and mitigation challenges.
Though benefits are many, implementing electronic charting is a costlier alternative than paper-based methods. However, a rapidly developing technology sector has driven down prices significantly from only a short time ago, and open-source software systems have also helped minimize costs, making electronic charting a much more financially feasible option than ever before.51 In Pakistan, development and implementation of an electronic charting system for the Karachi Trauma Registry cost US$9600 and was achieved using local resources only.38 Another electronic charting system in Pietermaritzburg, South Africa, reported the upfront cost of implementation at US$15 720.49 Typically, hardware and software costs are what often come to mind when implementing electronic data collection; however, other expenses like technician salaries, security, and the cost of operating a temperature-controlled server room also drive up costs and must be factored in. Though these costs are relatively low in the world of healthcare budgets, we recognize that they still may be out of reach for some lower-resource settings with competing healthcare priorities.
In addition to cost, there exist many other considerations for the effective implementation of electronic data collection, including the need for reliable electricity and internet access. Since trauma registries contain sensitive and confidential patient information, a secure network and a secure platform for the tablets is also essential. The use of a non-US-based cloud server should especially be considered to protect patient information given the newly enacted US CLOUD (Clarifying Lawful Overseas Use of Data) Act, which allows the US government to compel any US-owned technology company to provide them with data stored on their servers (regardless of where those servers are located). Despite these stipulations, electronic charting still remains a viable option for many LMIC trauma registries looking to improve efficiency and quality of data collection.
Standardization of trauma registry fields is another opportunity to improve quality of care efforts. While the inclusion of context-driven fields is arguably a very important aspect of conducting nuanced trauma research—and we acknowledge the value that this variability allows for—we recognize that for trauma registries to effectively benchmark results against other registries regionally, nationally, or even internationally, standardization of patient eligibility criteria and the variables collected is of utmost importance. A standardized minimum dataset, with the ability to add on more variables when appropriate, would allow for increased external benchmarking of outcomes and consequently provide more data to inform QA efforts. Such a dataset can also function as a resource for new trauma registries, identifying fields that are absolutely essential for collection in low-income and middle-income contexts. As not all trauma registries have the resource capacity to prioritize external benchmarking, this additional outcome of standardization is especially important and highlights how trauma registries in LMICs at both ends of the resource capacity spectrum can benefit by developing this standardized minimum dataset.
So, how can we address issues of standardization? And what fields necessitate collection? The answers are not so simple. While a top-down approach by WHO or another leading global body could force harmonization of such an initiative, and indeed incentivize collection of trauma registry data in the first place, the value of mobilizing a consortium of trauma registry advocates from LMICs to address issues of standardization and establish a minimal dataset should not be ignored. Such a grass-roots approach aligns with the development of trauma registries in LMICs so far, and more importantly is better positioned to identify and address the context-specific needs and challenges in developing these standards. There thus exists a tension between these two approaches that would ideally be addressed by a partnership of both a top-down and grassroots development structure. More can also be learned by looking to how other similar fields are handling these issues. A recent review in 2019 by an international, multidisciplinary working group examining emergency care registries in LMICs proposes a simple yet effective organizational framework to develop a more parsimonious list of variables for registry collection—a framework which could possibly be adapted to define what a minimum trauma registry dataset might look like.52
Conclusion
Trauma registries in LMICs represent a largely untapped opportunity to better understand and address the injury epidemic on a global scale. However, numerous barriers have so far hindered the potential of injury prevention, mitigation, and quality of trauma care improvement efforts, including missing data, lack of standardization, and poor dissemination of findings. Based on the current literature, we strongly believe that to improve the global uptake and sustainability of trauma registries, the following should be prioritized. First, there needs to be a collective effort from both the WHO and local trauma registry activists to address issues of standardization and the creation of a true minimum trauma registry dataset that is modular, dynamic, and scalable. This will help to accommodate a large spectrum of settings and allow for continued growth. Digital technologies can also help in making this objective more feasible. For new trauma registries or registries with low resource capacity, a minimum dataset will serve as an invaluable steppingstone for sustainable registry operation, as no resource like this currently exists. For registries with greater resource capacity, the adoption of this standardized minimum dataset will allow for increased external benchmarking of their findings, allowing them to identify areas where improvements in quality of care can be made. Second, the issue of poor data quality must be addressed. Missing or incomplete data greatly hinders the capacity for high-level research that can effectively inform injury prevention and mitigation programs. The introduction of inexpensive and innovative technologies into this sector has the power to drastically improve data collection. Use of these technologies in more settings should be further explored. Third, there needs to be greater dissemination of trauma registry findings to key stakeholders. CSOs and CBOs are uniquely positioned to affect change in their communities and should not be neglected in the large network of potential stakeholders that registry findings are disseminated to. Lastly, there must be a change in the global health landscape as a whole—one that more fully recognizes the injury crisis that is occurring, and the profound effect injury prevention can have on injury prevalence. Increased support for the development and improvement of trauma registries in LMICs is absolutely necessary if we are to address this injury epidemic.
References
Footnotes
Contributors LR, NS, and MH conceived of this manuscript; LR wrote the manuscript; NS, CA, AN, and MH critically revised the paper and provided valuable feedback. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area, or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests MH is a founder at T6 Health Systems, a company that specializes in electronic health record software.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.