Article Text

Abstract
Background Trauma patients with penetrating vascular injuries have a higher rate of venous thromboembolism (VTE). The objective of this study was to determine the risk of VTE formation in penetrating femoral and popliteal vascular injuries and the effects of endovascular management of these injuries.
Methods A retrospective study of Pennsylvania Trauma Outcome Study registry was conducted during a 5-year period (2013–2017). All adult patients with a penetrating mechanism with femoral/popliteal vascular injuries were studied. Primary outcome was incidence of VTE in patients with isolated arterial injuries versus combined arterial/venous injuries. Secondary endpoints were intensive care unit (ICU) length of stay (LOS), hospital LOS and mortality. Statistical comparisons were accomplished using Fisher’s exact tests, and parametric two-sample t-tests or non-parametric Wilcoxon rank-sum tests for categorical and continuous variables, respectively.
Results Of the 865 patients with penetrating extremity vascular injuries, 207 had femoral or popliteal artery injuries. Patients with isolated arterial injuries (n=131) had a significantly lower deep venous thrombosis (DVT) rate compared with those with concurrent venous injuries (n=76) (3.1% vs. 13.2%, p=0.008). There were 14 patients in the study who developed DVTs. Among the four patients with isolated femoral or popliteal arterial injuries who had developed DVTs, three had an open repair. Among patients with isolated arterial injuries, those with DVT spend significantly more time on the ventilator (median=2 vs. 0, p=0.0020) compared with patients without DVT. Patients with DVT also had longer stay in the hospital (median=17.5 vs. 8, p=0.0664) and in the ICU (median=3 vs. 1, p=0.0585).
Conclusions Risk of DVT exists in patients with penetrating isolated femoral and popliteal artery trauma. Open repair was associated with significantly higher DVT rates in isolated arterial injuries.
Level of evidence Level IV therapeutic care/management.
- venous thromboembolism
- penetrating trauma
- femoral artery
- popliteal artery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The incidences of venous thromboembolism (VTE) are found to be higher in trauma patients.2 3 A combination of Virchow’s triad with prolonged immobility due to multiple injuries, hypercoagulable states from blood product transfusion and hemorrhage and endothelial injury from direct trauma leads to this increased risk. Patients with vascular trauma are further predisposed to a higher risk of developing VTE due to direct vascular injury, blast injury and vessel manipulation during repair of vascular injuries.5 6 Penetrating vascular injuries have an even higher prevalence of VTE events (40.5%), with 73.5% of these involving gunshot injuries.7 Venous injuries have the highest incidence of VTE.
The most commonly injured vessels in the lower extremities are femoral and popliteal vessels. Knudson et al indicated in their review of trauma patients of the National Trauma Data Bank that having a venous injury was an independent risk factor for VTE with an OR 3.56 with a p value <0.0001.1 This group identified the following characteristics: age greater than 40 years, pelvic fracture, lower extremity fracture, spinal cord injury with paralysis, head injury, time on the ventilator for more than 3 days, venous injury, shock at admission and major surgical procedure, increase the risk of developing VTE.1 Frank et al demonstrated that having a venous injury significantly increases the risk of having VTE.8 Karcutskie et al validated in their study of 813 patients with blunt and penetrating injuries, that patients with repair or ligation of vascular injuries, Abbreviated Injury Scale (AIS) for the abdomen greater than 2, and aged 40–59 years were at risk for VTE.7 However, there is a paucity of literature which demonstrates specific rates of VTE with isolated penetrating lower extremity arterial injuries.
The indication for operative intervention in penetrating vascular injuries is well studied.11 With the advancement of endovascular techniques, extremity penetrating vascular injuries have been managed using these techniques. The PROOVIT registry was a multicenter review of 542 patients that described the current trends of endovascular management in patients with arterial injuries. Of these 542 patients, 7.4% underwent endovascular repair.2 Other studies have also demonstrated an increase in endovascular management of arterial injuries, especially in blunt trauma.3–5 However, the risk of VTE events after endovascular intervention has not been well studied.
The objective of this study was to determine the risk of VTE formation in penetrating femoral and popliteal vascular injuries and the effects of endovascular management of these injuries. The focused hypotheses of this study were as follows: (1) In the setting of femoral and popliteal penetrating arterial injuries, isolated arterial injuries also have a significant risk of VTE. (2) Using an open technique to manage isolated penetrating femoral and popliteal arterial injuries may increase risk of VTE as compared with an endovascular approach.
Methods
Study design and population
After approval from both the Institutional Review Board of Crozer-Keystone Health System and the Research Committee of the Pennsylvania Trauma System Foundation (PTSF), the prospectively collected Pennsylvania Trauma Outcome Study (PTOS) registry was retrospectively queried. (The data were provided by the PTSF, Mechanicsburg, PA. The Foundation specifically disclaims responsibility for any analyses, interpretations, or conclusions.) The PTOS registry is compiled via controlled, mandatory reporting from all trauma centers in the state of Pennsylvania. The PTOS registry is maintained by dedicated trauma registrars and undergoes the highest levels of validation both locally and at the state level.
The data used in this analysis were collected during a 5-year period (2013–2017). A total of 865 patients with isolated penetrating extremity vascular injuries were identified during this period. The following data points were abstracted for each patient: age (years), sex (male, female), race, injury type, injury time, transfer in time, Injury Severity Score (ISS), AIS, Trauma and Injury Severity Score (TRISS), time to CT scan, emergency department (ED) vital signs (systolic blood pressure (SBP), heart rate (HR), Glasgow Coma Scale (GCS)), hospital length of stay (LOS), intensive care unit (ICU) LOS, step-down LOS, ventilator days, mortality, discharge status, number of blood units, use of massive transfusion protocol (MTP), in-hospital complications, in-hospital procedures, and time for vascular intervention.
Inclusion and exclusion criteria
All trauma patients who were above the age of 18 with isolated penetrating extremity vascular injuries were identified for the study. Only patients with femoral and popliteal artery and/or vein injuries were included. The International Statistical Classification of Diseases, Ninth Revision and 10th Revision (ICD-9 and ICD-10) procedure codes were used to identify patients with extremity vascular injuries (ICD-9 codes: 904.1, 904.2, 904.41, 904.42; ICD-10 codes: any codes starting with S75, S85.0, S85.5). Exclusion criteria included patients who were pregnant, were identified as prisoners, and with concurrent non-extremity vascular injuries (figure 1).

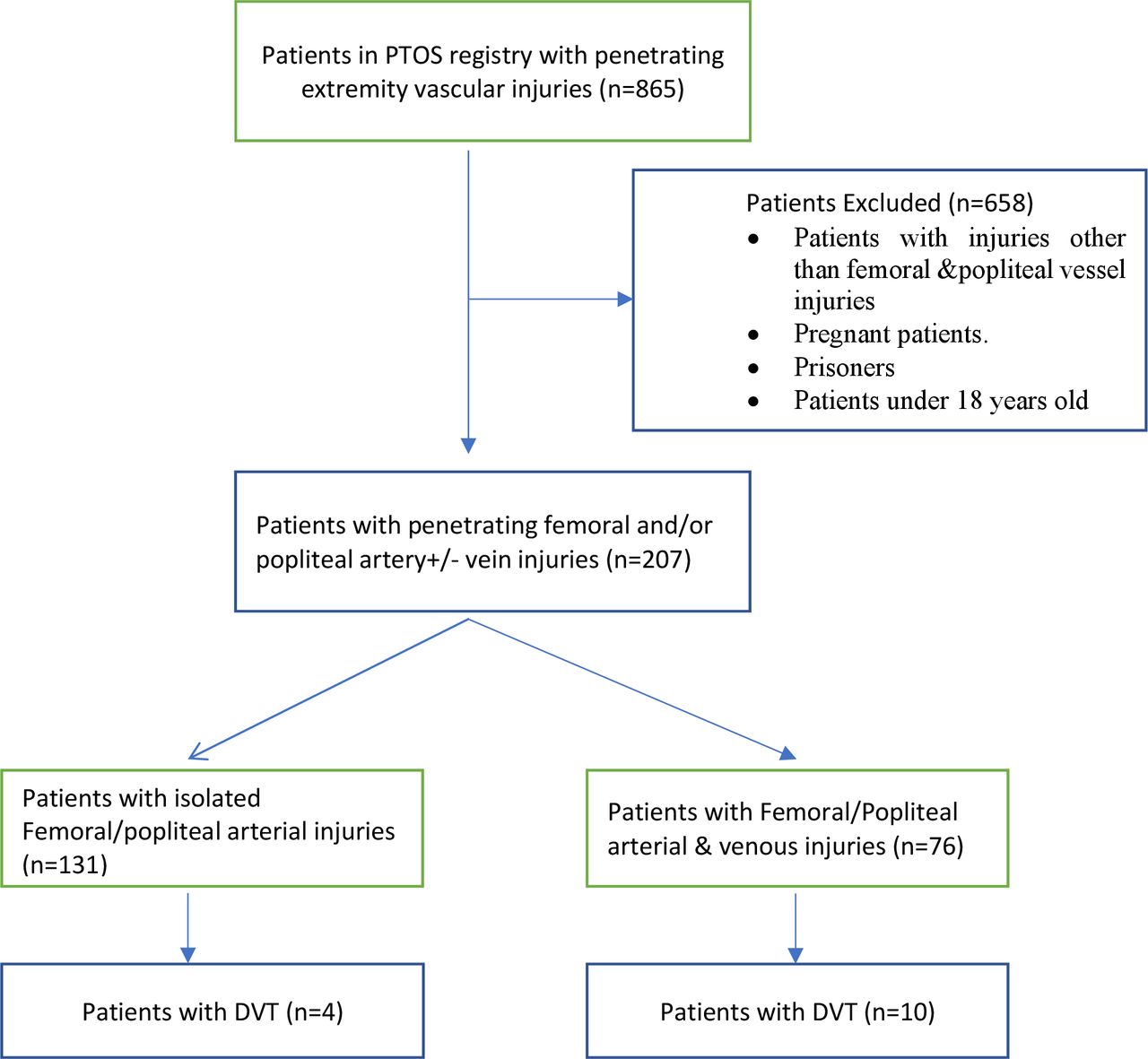{kind=link}
Flow diagram of patient selection. Two hundred and seven patients matched the inclusion criteria. The DVT rates were compared in patients with isolated femoral/popliteal arterial injuries and patients with concomitant femoral/popliteal venous and arterial injuries. DVT, deep venous thrombosis; PTOS, Pennsylvania Trauma Outcome Study.
Patient stratification
The patients studied were those who sustained penetrating femoral and popliteal vascular injuries. The two groups compared were patients with femoral and popliteal combined venous and arterial injuries and patients with just isolated arterial injuries. We evaluated patients in each group who underwent open, endovascular, and combined open/endovascular (hybrid) repair of their injuries. We also compared patients who developed femoral-popliteal deep venous thromboses (DVT) to patients without DVT. The PTSF defines DVT as ‘the formation, development, or existence of a blood clot or thrombus within the vascular system, which may be coupled with inflammation’. The diagnosis of DVT must be confirmed with a venogram, ultrasound or CT. The definition of DVT was adopted using the National Trauma Data Bank definition in 2011.
Outcomes
Our primary outcome measure was a dichotomous variable indicating presence or absence of DVT between the isolated arterial injury group versus the concomitant arterial and venous injury group. DVT rates based on surgical methodology (open, endovascular, or hybrid) were also studied. Outcomes were further stratified by ICU LOS, hospital LOS, step-down LOS, ventilator days, number of blood units, use of MTP and mortality rate.
Statistical analysis
Descriptive statistics (means, SD, medians, IQRs (Q1, Q3), percentages, counts) were used to characterize this sample of patients with penetrating femoral and popliteal vascular injuries. Distributions of the primary and secondary outcomes were compared across the following groups of patients: (1) patients with femoral-popliteal venous and arterial injuries versus those with isolated arterial injuries, (2) patients with femoral-popliteal injuries who had DVT versus those without a DVT, (3) patients with femoral-popliteal isolated arterial injuries who have a DVT versus those with no DVT, and (4) repair techniques (open, endovascular, hybrid) among patients with isolated femoral-popliteal isolated arterial injuries. Two-sample t-tests or non-parametric Wilcoxon rank-sum tests, as appropriate, were used for two-group comparisons of continuous variables; analysis of variance or non-parametric Kruskal-Wallis tests, as appropriate, were used for comparisons of continuous variables across three groups. Lastly, statistical comparisons involving categorical variables relied on Fisher’s exact tests. Statistical significance was taken at the p<0.05 level recognizing there was no adjustment for multiple comparisons and there may be clinically significant differences that do not demonstrate statistical significance due to lack of power or small sample size. Thus, significance was concluded within the context of clinically meaningful differences, and themes, across the various inferential comparisons, combined with statistically significant findings at the p<0.05 level.
The small sample sizes provide power to detect medium to large effect sizes. The primary endpoint of observed DVT rates for the two groups is 3.1% (isolated arterial injury group) versus 13.2% (concomitant arterial and venous injury group). For group sample sizes of 131 and 76 (total n=207), respectively, this study has 77% power to detect a difference of 10.1% in DVT rate using a χ2 test statistic and a type I error rate of 5%. When comparing DVT rate by procedure, a sample size of 207 achieves 38% power to detect a small effect size (W) of 0.1429 using a χ2 test with 3 df and a significance level of 0.05. Similarly, when comparing DVT rates by procedure among those with isolated arterial injuries, a sample size of 131 achieves 88% power to detect a medium effect size (W) of 0.3205 using a χ2 test with 3 df and a significance level of 0.05.
Results
Eight hundred and sixty-five trauma patients with penetrating extremity vascular injuries were identified. Of those, 207 patients had femoral and popliteal penetrating injuries that matched our inclusion and exclusion criteria. There were 135 (65.2%) with femoral artery injuries and 81 (39.1%) patients with popliteal artery injuries. Patients with both femoral and popliteal artery injuries were included in both counts. Of the 207 patients with femoral or popliteal artery injuries, 76 (36.7%) had concurrent femoral or popliteal vein injuries. Patient demographics, injury parameters and ED vital signs in the isolated arterial injuries and femoral-popliteal venous and arterial injury groups are summarized in table 1. There were no statistically significant differences in age, HR, SBP in ED, gender and race between the isolated arterial and concomitant arterial and venous injury groups. Patients with concomitant arterial and venous injuries had a significantly lower median TRISS (p=0.017) compared with the isolated arterial injury group. However, there were no significant differences in median ISS and AIS between the two groups.
Patient characteristics by femoral or popliteal arterial and venous injuries (n=207)
The concomitant arterial and venous injury group had a higher DVT rate of 13.2% (n=10) compared with the isolated arterial injury group of 3.1% (n=4) with a p value of 0.0083. Patients with concomitant arterial and venous injuries had longer median ICU LOS (p=0.0016), more days on the ventilator (p=0.005) and longer overall median hospital LOS (p=0.0124) (table 1). Patients with concomitant arterial and venous injuries required higher amount of blood transfusions (p=0.0002) and a higher MTP requirement with a rate of 37.8%, compared with patients with isolated arterial injuries (14.1%, p=0.0060).
In comparing patients with DVT to those without DVT, there were no statistically significant differences in age, gender and race (table 2). There were no statistically significant differences in ED SBP and GCS. In patients with DVT, the ICU LOS was significantly longer compared with the countergroup (p=0.0008). The ventilator days (median 1.5 vs. 0, p=0.0007) and total hospital LOS (median 17.5 vs. 9, p=0.0013) were significantly longer in the DVT group compared with the non-DVT group. However, there were no statistically significant differences in mortality rates found (p>0.9999). As shown in table 3, among patients with isolated arterial injuries, those with DVT spend significantly more time on the ventilator (median=2 vs. 0, p=0.0020) compared with patients without DVT. Patients with DVT also had longer stay in the hospital (median=17.5 vs. 8, p=0.0664) and in the ICU (median=3 vs. 1, p=0.0585) compared with those without DVT.
Patient characteristics for those with femoral or popliteal arterial and venous injuries with and without DVTs (n=207)
Patient characteristics with isolated arterial injuries with and without DVTs (n=131)
Using the same cohort of patients, we further compared groups who underwent endovascular, open and hybrid techniques (open and endovascular combined technique) of vascular repair. The surgical techniques performed were identified using ICD-9 and ICD-10 procedure codes. In the isolated femoral/popliteal arterial injury group, 22.9% of the patients had endovascular repair, 13.7% had open repair and 26.0% had hybrid repair. 37.4% (n=49) of the patients in this group had no intervention performed for their injuries. In patients with concomitant venous and arterial injuries, 14.5% had endovascular repair, another 14.5% had open repair and 27.6% had hybrid technique used. There were 43.4% (n=33) of the patients in the concomitant venous and arterial injury group who did not undergo any intervention. The incidences of DVT in the isolated arterial injury group who had no intervention were 2.0% (n=1) and 6.1% (n=2) in the concomitant arterial and venous injury group (p=0.5618).
In comparing patients who developed DVTs and the type of procedure which was used to address the vascular injury, among the four patients with isolated arterial injuries, three (75.0%) underwent an open repair and one (25.0%) received no intervention. Of the 10 patients with concomitant arterial and venous injuries, one (10.0%) underwent an open repair, two (20.0%) underwent an endovascular repair, five (50.0%) underwent a hybrid, and two (20.0%) received no intervention.
In the isolated arterial injury group (table 4), there were no statistically significant differences in patient demographics such as age, gender and race between the techniques of vascular repair. There were no statistically significant differences in ISS and AIS between the groups. There were no differences in amount of blood units transfused and MTP requirements between the groups. In the isolated arterial injury group, patients who underwent an open repair had a significantly longer median ICU LOS (p=0.0185) and ventilator days (p=0.002) compared with patients who had endovascular repair. The open repair and hybrid repair groups had a longer hospital LOS than the endovascular repair group (p=0.0150), but no statistically significant differences in hospital LOS were observed between the open and endovascular groups (p=0.1026)
Patient characteristics with isolated femoral and popliteal arterial injuries by repair technique (n=131)
Discussion
Trauma patients with direct vessel injury are at greater risk of developing DVTs. In this analysis of patients with penetrating femoral and popliteal vascular injuries in a state-wide database, we have found a significant increase in rate of DVTs in patients with penetrating concomitant arterial and venous femoral and popliteal injuries. It is also interesting that patients with isolated arterial injuries also developed DVTs (3.1%). The majority of the patients in the isolated arterial injury group who had DVT had an open repair. There were no significant demographic differences in characteristics between the isolated arterial injury group and concomitant venous and arterial injury groups. Therefore, the incidence of DVTs in this group is suspected due to the blast effect of the missile and/or manipulation of the associated vein during open repair.
It is known that there is a rising trend in managing these injuries in endovascular and hybrid techniques.2–5 Although the literature describes treatment of blunt and non-compressible torso vascular injuries using endovascular or hybrid techniques, we found in our study that penetrating lower extremity vascular injuries are also being managed using endovascular techniques. In this study, we did not find significant differences in ED vital signs between the groups of patients who underwent open, endovascular and hybrid techniques. There was no evidence in this cohort that patients with hemodynamic instability had open operations. Even with blood transfusion requirements endovascular or hybrid techniques were in use.
When comparing patients in the isolated femoral and popliteal arterial injury group based on surgical technique (open, endovascular and hybrid) there were no differences in patient characteristics. Patients with isolated arterial injuries who had an open repair were found to have a significantly longer ICU stay, hospital LOS, and longer days on the ventilator compared with the patients who had endovascular repairs. A significant risk of developing a DVT was identified in patients with isolated arterial injury who had open repair. As demonstrated by our data, having a DVT increases ICU LOS and hospital LOS and prolongs the number of days on the ventilator. This drives resources and costs needed to treat DVTs with anticoagulation. We did not find an increased risk of mortality from developing a DVT in our cohort but we were not powered for this particular question. Recognizing the risk of DVT formation in this group with isolated femoral and popliteal arterial injuries who had an open repair is likely meaningful for the practicing surgeon.
There are major factors in trauma patients with multiple injuries that increase their risk of DVTs. It is well known that having a venous injury increases the risk of DVT. As demonstrated in our study, there is a risk of DVT even in isolated arterial injuries. Having an open repair increased the risk of having a DVT in this cohort. Consideration should be given to early and consistent chemical VTE prophylaxis in this group of patients, to mitigate resources associated with prolonged hospital stay and long-term anticoagulation.
In this study examining DVT rates in patients with penetrating lower extremity vascular injuries, we acknowledge that it has several limitations. This is a retrospective review which carries its inherent limitations. Review of a state data bank leads to absence of clinical granularity. We were not able to study the timing and method of VTE prophylaxis administration as chemical prophylaxis practice patterns differ in various institutions and that data are not available to review. We were also not able to identify the site of DVT in relation to the femoral/popliteal injuries due to lack of such data in the state registry. Diagnostic criteria used to identify DVTs, whether screening methods were employed or if DVTs were symptomatic, were not available for review. All DVTs reported in this study were in-hospital occurrences. There is a small sample size of patients who developed DVTs in this cohort. Further investigation is required to study the screening methods and treatment of DVT in this cohort of patients. Additionally, other limitations of the study were the relatively small sample sizes supporting the various hypothesis tests as well as the lack of control for multiple comparisons. As such, significance is concluded within the context of clinically meaningful differences, and themes, across the various inferential comparisons, combined with statistically significant findings at the 0.05 level of significance. Despite the above limitations, the risk of DVT in isolated femoral and popliteal arterial injury group exists and is understudied. Future consideration should be given to using a larger data bank or performing a multicenter trial to study this cohort of patients and effects of endovascular repair on DVT rates in penetrating lower extremity vascular injuries.
Conclusions
In conclusion, patients with penetrating lower extremity vascular injuries, even those with isolated arterial injuries, are at risk of developing DVTs. Consideration must be given for early and consistent chemical DVT prophylaxis. In the era of increased utilization of endovascular and hybrid repair of vascular injuries, open repair of isolated femoral and popliteal arterial injuries carries a higher risk of DVT development.
Footnotes
Contributors AR, OP, SN, and SD performed the literature search. AR, SN, SD, and NM created the study design. AR, OP, SN, and SD participated in data collection. AR, NM, AL, DS, and AH performed data analysis and data interpretation. AR, NM, SD, AL, DS, and AH participated in writing and critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Institutional Review Board of Crozer-Keystone Health System and the Research Committee of the Pennsylvania Trauma System Foundation (PTSF).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data from the PTOS registry were deidentified.