Article Text

Abstract
Background Patients with rib fractures require analgesia, oxygen supplementation and physiotherapy. This combination has been shown to reduce morbidity and mortality due to rib fractures. There has been movement towards the use of high-flow nasal prong (HFNP) oxygen. However there are no studies demonstrating the effectiveness of HFNP in this population. The aim of this study was to compare HFNP to venturi mask (VM) in rib fracture patients.
Methods Randomized controlled trial. Patient population included patients with rib fractures and high-risk features (three or more rib fractures, flail segment, bilateral rib fractures, smoker or chronic obstructive pulmonary disease). Exclusion criteria included initial mechanical ventilation and contraindications to HFNP. Patients were randomized to HFNP or VM. Primary outcome was deterioration requiring mechanical invasive/non‐invasive ventilation, or unplanned admission to intensive care unit. Secondary outcomes included mortality, length of stay, high dependency length of stay, comfort levels, breathing exertion levels (as measured by Borg Scale), oxygen saturation, respiratory rate, heart rate, chest X-ray and arterial blood gas parameters.
Results 220 patients (average age 60 years and average of four rib fractures each) were randomized to HFNP (n=113) and VM (n=107). There was no statistically significant difference in the primary outcome comparing HFNP and VM (6.2% vs. 6.5%, p=1.0). There were also no statistically significant differences in the secondary outcomes except for PaCO2 (43.6 vs. 45.5, p=0.039)
Conclusion HFNP oxygen supplementation does not appear to be more effective than VM oxygen supplementation in patients with rib fractures.
- oxygen inhalation therapy
- rib fractures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Rib fractures occur commonly as a result of blunt chest trauma and are associated with significant morbidity and mortality due to respiratory failure and pneumonia.1–3 These complications affect up to 25% of patients with rib fractures, and resulting in escalation of care, admission to intensive care units (ICU) and increased length of hospital stays.4 5 Rib fractures are frequently associated with intrathoracic injuries including pulmonary contusions, hemothorax, pneumothorax and aortic injury. Factors that increase the risk of complications from rib fractures include increasing age, number of rib fractures and pre-existing respiratory disease.3 6–8
The two main goals of therapy are pain management and pulmonary care and support. There is strong evidence for providing good analgesia to facilitate volume expansion treatment and chest physiotherapy, aiming for deep breathing and effective cough to reduce secretions and prevent atelectasis.2 8–10 Oxygen supplementation is often included as supportive therapy added to bundles of care for patients with rib fractures.10–12
High-flow nasal prong (HFNP) oxygen (O2) was first developed for neonates and has gained increasing use in adult patients for prevention and treatment of respiratory failure.13 High-flow humidified oxygen with flow rates from 30 to 100 L/min with high fraction of inspired oxygen (FiO2) is able to be delivered.14 There have been proposed benefits of using HFNP O2 including increased comfort, tolerance and increased mucociliary clearance.15–17 Positive end-expiratory pressure can be generated, preventing alveoli collapse. The washout of carbon dioxide (CO2) and replacement with enriched O2 purportedly decreases work of breathing and increases breathing effectiveness.13 14 17–19
There is a significant cost associated with HFNP O2, including the humidifier and the disposable delivery system as well as staff training and labor cost for the management of device.
Although there are studies examining the use of non-invasive ventilation (NIV) for blunt chest trauma,20 there are no studies examining the optimal method of oxygen supplementation in preventing complications related to rib fractures.
The aim of this study was to compare high-flow oxygen therapy to venturi oxygen supplementation in preventing respiratory complications related to rib fractures and also assess patient’s tolerance and comfort with the use of the devices.
Methods
Study design
The study was a single-center, prospective randomized controlled trial aimed to assess the efficacy of HFNP therapy in trauma patients with risk factors for respiratory deterioration. Patients were allocated to receive HFNP therapy or oxygen via a venturi mask (VM) according to a computer-generated randomization program. Permuted block randomization was used.
Setting and participants
All trauma patients presenting to a level 1 trauma center in Sydney, New South Wales, Australia, were assessed for eligibility. The inclusion criteria were patients with rib fractures confirmed with CT imaging and one or more risk factors for respiratory deterioration: age greater than 55 years, three or more rib fractures, bilateral rib fractures, flail segment, smoker or known underlying respiratory disease. Exclusion criteria include: intubation prehospital or in emergency department, contraindication to HFNP (base of skull fracture, unstable facial fractures) and inability to consent (confusion, non-English speaking background).
Intervention
Patients were randomly allocated using a computer-generated sequence in a 1:1 ratio to either receive HFNP therapy or oxygen via a VM. VM was selected instead of nasal prongs so FiO2 could be accurately delivered.21 All patients were admitted to a high dependency surgical or trauma unit. FiO2 was initiated at 0.4. For patients allocated to HFNP, flow rate was initiated at 60 L/min. All other treatment was as per standard hospital protocol including continuous monitoring in a high dependency unit (HDU), daily chest physiotherapy, analgesia including: paracetamol, non-steroidal anti-inflammatory drugs if not contraindicated, opioids via patient-controlled analgesia device and regional anesthesia as determined by the acute pain service. Patients underwent surgical stabilization of their rib fractures as determined by the attending trauma surgeon. FiO2 for both HFNP and VM was titrated to maintain oxygen saturation (SpO2) ≥95. Patients with advanced chronic obstructive pulmonary disease were given supplementary O2 for SaO2 88% to 92%. For the HFNP cohort, the flow rate was maintained at 60 L/min for at least 24 hours and then until SpO2 was maintained on FiO2 of 0.21.
Outcomes
The primary outcome was a composite endpoint of unplanned transfer to ICU due to respiratory deterioration, escalation of ventilation support, including NIV and intubation for mechanical ventilation. These patients were ICU medically reviewed and then accepted for admission to ICU due to their increasing respiratory distress and failure.
Secondary outcomes included mortality, hospital length of stay (LOS), HDU LOS and development of pneumonia. Daily measurements were recorded for arterial pH, partial pressure of oxygen in arterial blood (PaO2), partial pressure of carbon dioxide in arterial blood (PaCO2), peak flow and O2 saturations. Comfort levels with the different modes of oxygen delivery were measured with the Likert scale.21 22 The perceived effort of breathing was measured with the modified Borg Scale.23 24 Results for the daily measurements were averaged during the first 3 days after hospital admission.
Statistical analysis
All statistical analyses were performed using Statistical Package for Social Sciences (SPSS) Predictive Analytics Software (PASW) V.24.0 (SPSS). Continuous data are presented as means and SD or medians and IQR (range from the 25th to the 75th percentile). χ2 test or Fisher’s exact test was used to compare proportions and to test for trends. The Student’s t-test and Mann-Whitney U test were used to compare unpaired groups of continuous data. Univariate analysis identified any significant differences. For all analyses, actual p values were reported and where possible, 95% CIs presented. All tests were two tailed. Differences were considered to be statistically significant at a p<0.05 level.
The sample size was calculated to detect a 15% difference in the primary outcome with α=0.05 and power 80%.
Results
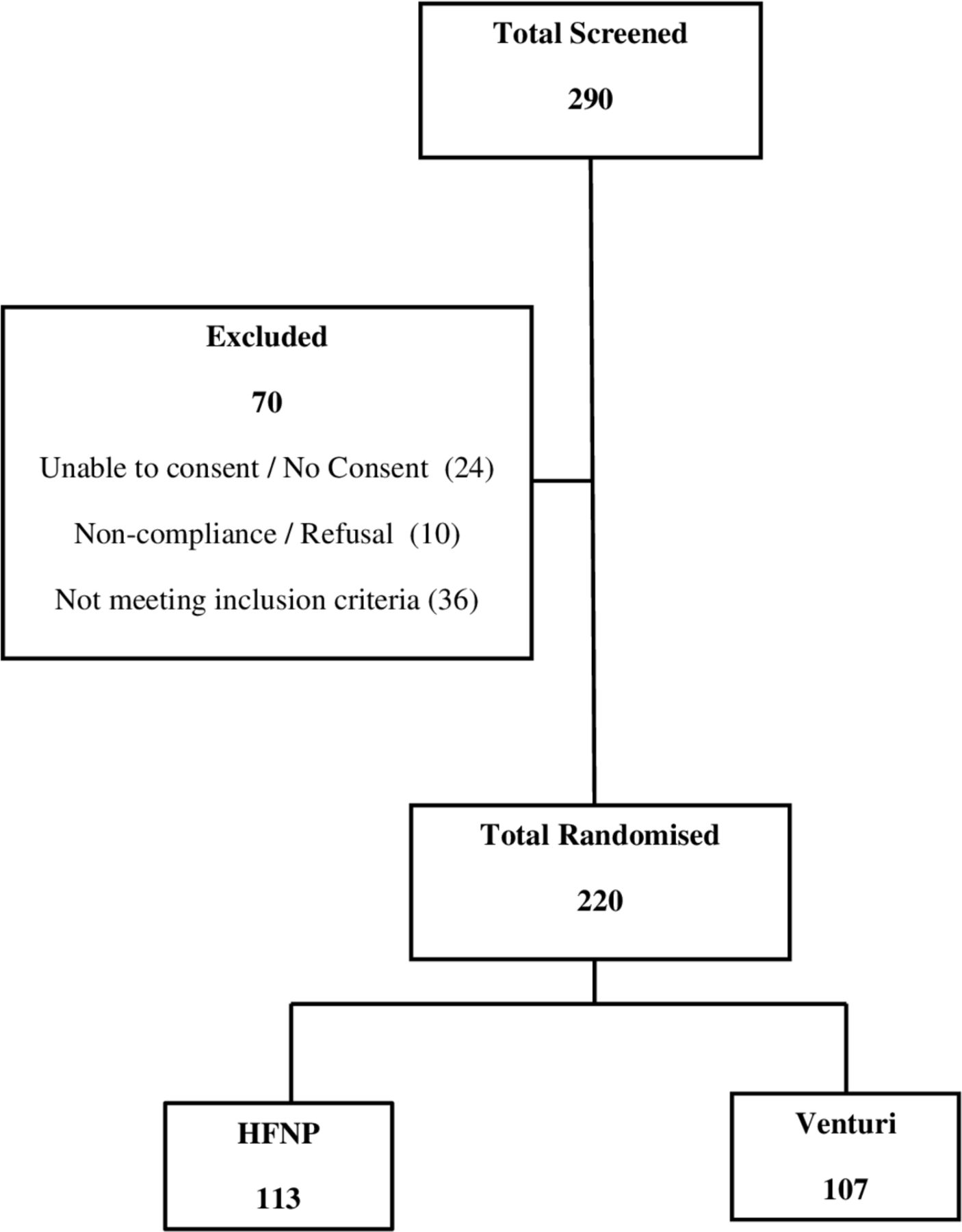
During the study period 290 patients were screened for inclusion to the study (figure 1). Seventy patients were excluded in total. Thirty-six were excluded due to not meeting study inclusion criteria; 24 patients were unable to be consented; 10 patients refused or were not compliant with HFNP or VM after recruitment and were excluded from the study. On post hoc analysis, none of these exclusions achieved the primary outcome, that is, unplanned admission to ICU/escalation of O2 therapy to invasive ventilation or NIV. Secondary outcome measures were unobtainable due to the patient refusing the required investigations. Therefore, the total number of study participants was 113 in HFNP group and 107 in VM group.
Table 1 demonstrates the demographics and clinical characteristics of included patients.

{kind=link}
Randomization screening and exclusion flow diagram. HFNP, high-flow nasal prong.
Table 2 shows there was no difference in the rates of unplanned transfer to ICU and/or escalation of ventilatory support between the HFNP group (6.2%) and VM group (6.5%), p=1.0.
There was no difference in mortality, high dependency LOS or total hospital LOS, between the two groups. There was no difference in the Likert comfort scale or the modified Borg Scale of perceived breathlessness between the two groups. Respiratory rates and oxygen saturations were no different between the two groups.
Arterial blood gas results showed no difference in pH or PaO2. PaCO2 for HFNP group was lower (43.6 mm Hg, SD=5.6) compared with the VM group (45.5 mm Hg, SD=6.5). This was a statistically significant difference (p=0.032). Peak flow measurement for both groups was not significantly different.
Discussion
This randomized controlled trial failed to demonstrate a difference in the primary outcome. HFNP did not show a decrease in respiratory complications when compared with oxygen delivery via a VM in trauma patients with rib fractures.
Of the secondary outcomes there was only found to be a slight decrease in PaCO2 level in patients receiving HFNP, with a difference of 2 mm Hg between the averages of the groups. The clinical relevance of this is likely to be minimal.
Overall, a low rate of respiratory complications was observed in both groups (6.2% in the HFNP and 6.4% in the VM group). The effective management of rib fractures requires a bundle of care involving appropriate analgesia from acute pain care team and aggressive early interventions of physiotherapy and pulmonary toilet targeting enhancement of the patient’s functional capacity.4 25
There are no existing studies examining the optimal method of oxygen supplementation for patients with rib fractures. A previous systemic review analyzing nine studies concluded that in appropriately chosen patients early use of NIV in patients with blunt chest trauma might decrease respiratory complications and prevent intubation.26 27 HFNP O2 failed to show benefit in the prevention of respiratory complications over conventional O2 therapy in high-risk respiratory patients with abdominal surgery.27 28
There may be a theoretical benefit with the use of HFNP O2, with increased positive pressure, and humidified oxygen promoting expectoration of secretions. The results of our study suggest that these theoretical benefits may not translate to a clinically significant effect.
It was also hypothesized that the HFNP system would be more comfortable for patients, as only nasal cannulae were required as compared with a mask. However, again, our results would suggest that patients tolerate both systems equally well.
In the setting of modern healthcare, fiscal discipline is required to counter the ever-increasing introduction of technological advancements. Although a formal cost-benefit analysis was not performed, there is a cost difference between the HFNP O2 system and the VM system ($A92.25 vs. $A1.90; approximate at time of writing). The extra costs associated to HFNP are attributed with the disposable items of tubing, humidification system, water for irrigation and the HFNPs of the HFNP devices. VMs are cheaply manufactured and sold.
Limitations
Power calculations were based on a higher incidence of respiratory deterioration. There was an unexpectedly lower incidence of respiratory deterioration in this study than the incidence used for power calculation.
The study was not blinded to either patients or the treatment team, which may have introduced bias with the decision to escalate therapy. However, the secondary outcomes do not support any significant differences between the groups. This study was also performed in an urban tertiary trauma hospital, hence might not be applicable to smaller centers.
Conclusion
Oxygen supplementation with HFNP O2 compared with VM oxygen was not shown to be more effective for oxygen supplementation to decrease respiratory complications in trauma patients with rib fractures and high-risk features for respiratory deterioration. There should be consideration for further research to determine if there are any particular groups which may benefit from particular oxygen supplementation systems.
Acknowledgments
Thanks to all the doctors and nurses at the Westmead Trauma Service and Westmead Hospital HDUs who helped obtain the data and gave advice regarding running of this randomized controlled trial.
References
Footnotes
Contributors All authors contributed to the research project and article writing. JMH: conception of project, submission of ethics and governance approval, data analysis, article writing, review of submission. PTC: conception of project, submission of ethics and governance approval, article writing, review of article. LEC: concept of research project, submission of ethics and governance approval, review of data, article writing, review of article. MW: conception of research project, submission of ethics and governance approval, data collection, article writing, submission of research project for publishing.
Funding Funding for publication was provided by the Westmead Trauma Research Trust Fund.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Western Sydney Human Research Ethics Committee (AU RED HREC/15/WMEAD/509).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Database securely stored and is available on request.