Article Text

Abstract
Background Pancreatic pseudocysts may develop after high-grade pancreatic injuries in children. Many resolve without intervention, and the management of symptomatic pseudocysts that persist remains controversial, with various open, percutaneous and laparoscopic approaches to intervention described. Successful endoscopic cyst gastrostomy has been reported in children with pancreatic pseudocysts of mixed etiology.
Methods The trauma registry and electronic medical record of a level 1 pediatric trauma center were queried for children with a symptomatic pseudocyst following pancreatic trauma over a 12-year period, from 2008 to 2019.
Results We describe a case series of five consecutive children with persistent symptomatic pancreatic pseudocysts following blunt abdominal trauma all successfully treated with endoscopic cyst gastrostomy.
Discussion Endoscopic cyst gastrostomy appears to be safe and effective in the management of symptomatic pancreatic pseudocysts in children following pancreatic trauma.
Level of evidence 5 – retrospective case series.
- abdominal injuries
- pediatrics
- pancreas
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Pancreatic injuries are unusual, constituting 0.3% of pediatric trauma admissions and 2%–5% of admissions for blunt abdominal trauma.1 2 Overall, 76% of pancreatic injuries are managed non-operatively.1 Most pediatric pancreatic injuries do not involve a ductal injury and are managed non-operatively. Approximately half of pancreatic ductal injuries are managed non-operatively as well.1 3 4 An estimated 30%–80% of patients with a pancreatic ductal injury develop a pseudocyst and about 35% of them will undergo an intervention to drain the collection.2 5 Indications for intervention include persistent pain or anorexia, obstruction and infection.6 Options for intervention include open or laparoscopic anastomosis to nearby bowel segments (typically the stomach) and percutaneous or endoscopic drain placement. Literature documenting endoscopic drainage for mixed etiology pseudocysts in children reports a success rate of > 90%.3 7–16 Here, we describe five cases of symptomatic traumatic pseudocysts successfully treated with endoscopic cyst gastrostomy.
Methods
Demographic and clinical data on consecutive patients with a persistent post-traumatic pancreatic pseudocyst were extracted from the trauma registry of a level 1 pediatric trauma center over a 12-year period. Data analyzed included age, gender, mechanism of injury, nutritional approach, time to intervention and indications, periprocedural care and long-term outcome. Results were reported using the CAse REport (CARE) guidelines for case series.17
Results
From 2008 to 2019, 10 807 trauma patients were admitted, 29 of whom suffered a pancreatic injury (0.2 %), 12 of which (41 %) were high grade. Nine of these were treated non-operatively (75 %), and five developed traumatic pancreatic pseudocysts (42 %) that failed to resolve with non-operative management and underwent an intervention. Mechanisms of injury were four bicycle handlebar impacts and one fall onto rocks.
Nutrition
All patients received parenteral nutrition (PN) prior to intervention. The approach to diet was variable. Three patients were discharged home prior to their intervention: one patient on a bland diet with PN supplementation, one nil per os (NPO) on full PN support after failing nasojejunal feeding in the hospital and one on a low-fat diet before being readmitted secondary to pain and anorexia. This patient then failed a trial of nasojejunal feeding in the hospital and was limited to PN prior to intervention. Two patients remained in the hospital until intervention was performed: one transferred from an outside hospital on PN only and the other on PN only after failing nasojejunal feeds. All patients underwent intervention for similar indications: enteral feeding intolerance, abdominal pain and failure of their pseudocysts to resolve.
Intervention
Three patients underwent endoscopic cyst gastrostomy with placement of two 10-french double-pigtail stents. This was the only intervention for two of them, while the third had previously undergone a sphincterotomy and unsuccessful pancreatic duct stent placement earlier in his hospital course.
Secondary to concern about debris in the pseudocyst, two patients underwent placement of a 10 mm diameter expanding metal stent, and this was the only intervention for one patient. The other initially underwent endoscopic pancreatic duct stent placement soon after injury followed a week later by percutaneous abdominal drain placement for free pancreatic ascites. This patient developed a pseudocyst that was then managed with endoscopic cyst gastrostomy.
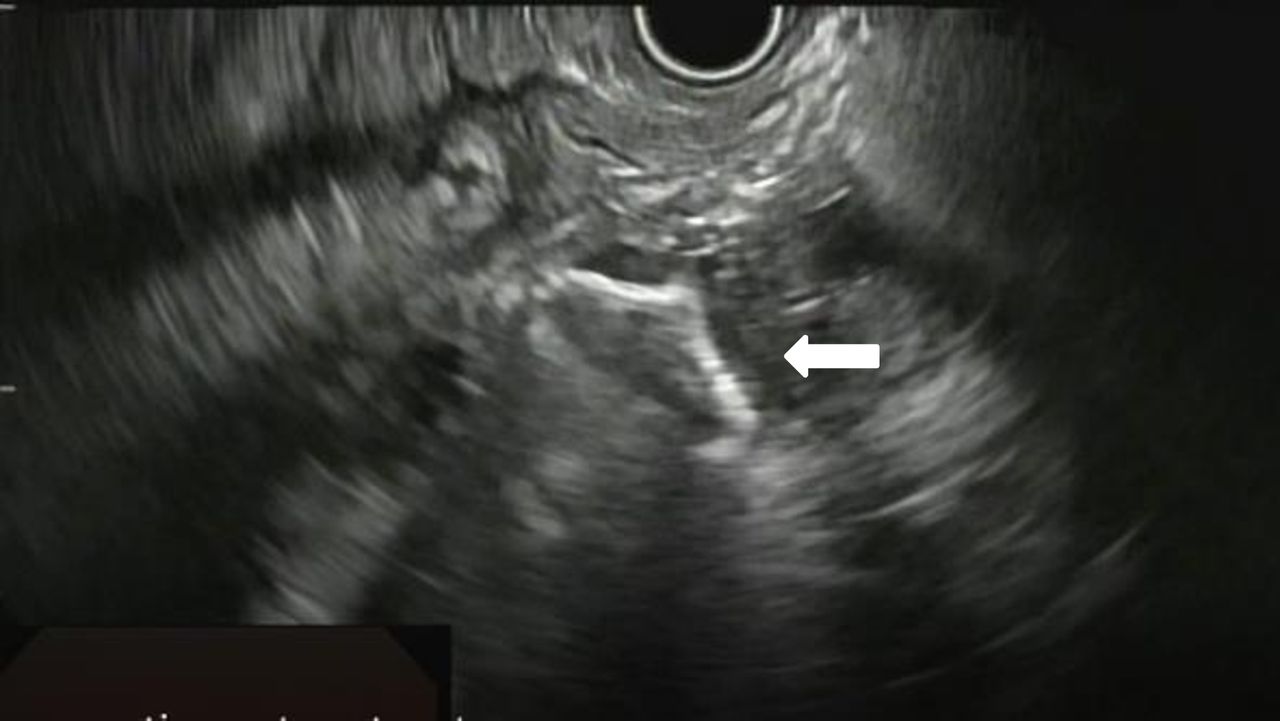
Procedures were performed using an endoscope with the aid of endoscopic ultrasound (EUS). Figure 1 demonstrates the use of EUS to visualize the pseudocyst containing debris. The deploying stent can be seen in figure 2. The endoscope was used to verify correct placement of the intraluminal portion of the metal stent (figure 3). A metal cystgastrostomy stent can be seen in proper position on an abdominal film (figure 4). Pseudocysts, at the time of drainage, varied in size from 4×3×7 cm to 8×14×9 cm.

EUS demonstrating pseudocyst filled with debris posterior to the stomach.
Deployment of expanding metal stent between pseudocyst and stomach lumen.

Metal stent in position, visualized from stomach with endoscope.

Abdominal X-ray demonstrating stent position with overlying air in stomach.
Stents were placed from 5 weeks to 7 weeks after injury and were removed as an outpatient from 3 weeks to 18 weeks later. Poststent removal ultrasound was performed, which demonstrated complete resolution of the pseudocyst (figure 5). Follow-up has ranged from 4 months to 72 months. All patients have had complete resolution of their pseudocysts on follow-up imaging and have transitioned back to a full fat regular diet with no indication of pancreatic insufficiency in any patient. One patient had lingering vague abdominal complaints 4 months from injury but with no evidence of pancreatic insufficiency. That patient returned again at 18 months with frequent stools, but again, testing for pancreatic insufficiency was negative. Individual patient characteristics and treatment timelines are shown in table 1.
Patient characteristics and treatment timelines

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abdominal US showing resolution of fluid collection. US, ultrasound.
Discussion
Pancreatic fluid collections are common following pancreatic trauma, especially when non-operative management is used; however, not all will develop into a pseudocyst.2–5 The revised Atlanta classification defines a pseudocyst as a collection present 4 weeks or more postinjury.6 Approximately 15%–18% of patients managed non-operatively will develop pseudocysts and approximately 10%–33% of pseudocysts will require subsequent drainage.2 3
Historically, laparotomy has been the preferred procedure for drainage of pseudocysts in the pediatric population. Laparotomy for drainage is typically successful but may bear significant morbidity and a risk of surgical complications.18
Laparoscopic cyst gastrostomy has had limited use in the pediatric population. A case report of two patients, one with acute pancreatitis and one with blunt trauma, with subsequent pseudocyst formation, underwent successful laparoscopic cyst gastrostomy without complication.18 This technique has been deemed useful due to its ability to definitively drain the pseudocyst, and its minimally invasive nature makes it advantageous over a laparotomy; however, there is a 10% risk for conversion to an open procedure in adults.6
Percutaneous drainage may be successful but typically is associated with longer time to resolution and higher failure rates in both children and adults.3 19 20 Risks include the development of a pancreatico-cutaneous fistula, reaccumulation of fluid and inadequate evacuation of viscous cyst contents.3 14
Endoscopic cyst gastrostomy for the drainage of pancreatic pseudocysts in the pediatric population has been reported, but most cases are from outside of the USA and were performed for non-traumatic etiologies. During the procedure, an endoscope alone, or with the addition of EUS, is used to visualize the optimal site for access to the pseudocyst, where an extramural bulge is seen protruding into the stomach wall. An endoscopic needle is used to puncture the cyst and, using the Seldinger technique, a wire and either double pigtail stents or an expanding metal stent are placed.7–14 16 Cyst contents may be seen emptying into the gastric lumen.
Patients experienced complete resolution of the pseudocyst after stent placement. Stents are removed in 6–12 weeks if not passed spontaneously, with few reports of repeated intervention.7–16 One study reported pseudocyst recurrence after stent removal in a trauma patient who subsequently underwent open cyst gastrostomy.7 Another describes a trauma patient with effective drainage of a pseudocyst with endoscopic cyst gastrostomy who then developed a second collection, which resolved with endoscopic cyst duodenostomy.8
Few complications following endoscopic cyst gastrostomy have been reported among the pediatric population. None of the patients reported here suffered any complications.
Conclusion
Endoscopic cyst gastrostomy provides long-term resolution of pediatric post-traumatic pancreatic pseudocysts with minimal procedural morbidity.
References
Footnotes
Contributors All authors contributed to the development and design of the study, data interpretation and critical revision of the manuscript. BJF additionally contributed to the data collection and initial drafting of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This research was approved by the Boston’s Children’s Hospital Institutional Review Board (IRB-P00015971).
Provenance and peer review Not commissioned; internally peer reviewed.