Article Text

Abstract
Background Resuscitative endovascular balloon occlusion of the aorta (REBOA) should be safely placed at zone 1 or 3, depending on the location of the hemorrhage. Ideally, REBOA placement should be confirmed via fluoroscopy, but it is not commonly available for trauma bays. This study aimed to evaluate the accuracy of REBOA placement using the external measurement method in a Japanese trauma center.
Methods A retrospective review identified all trauma patients who underwent REBOA and were admitted to our trauma center from 2008 to 2018. Patient characteristics, REBOA placement accuracy, and complications according to target zones 1 and 3 were reviewed.
Results During the study period, 38 patients met our inclusion criteria. The in-hospital mortality rate was 57.9%. REBOA was mainly used for bleeding from the abdominal (44.7%) and pelvic (36.8%) regions. Of these, 30 patients (78.9%) underwent REBOA for target zone 1, and 8 patients (21.1%) underwent REBOA for target zone 3. The proportion of abdominal bleeding source in the target zone 1 group was greater than that in the target zone 3 group (56.7% vs. 0%). Overall, the proportion of REBOA placement was 76.3% in zone 1, 21.1% in zone 2, and 2.6% in zone 3. The total REBOA placement accuracy was 71.1%. At each target zone, the REBOA placement accuracy for target zone 3 was significantly lower than that for target zone 1 (12.5% vs. 86.7%, p<0.001). No significant associations between non-target zone placement and patient characteristics, complications, or mortality were found.
Conclusions The REBOA placement accuracy for target zone 3 was low, and zone 2 placement accounted for 21.1% of the total, but no complications and mortalities related to non-target zone placement occurred. Further external validation study is warranted.
Level of evidence Level IV.
- trauma/ critical care
- resuscitation for shock
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Resuscitative endovascular balloon occlusion of the aorta (REBOA) may be useful for temporary hemorrhage control as a bridge to definitive hemostasis. In recent years, REBOA is more commonly used than aortic cross clamp with thoracotomy in Japan.1 However, the details about REBOA, such as positioning, time, catheter brand, and balloon size, in clinical practice are unknown. One of the proposed REBOA management options is the anatomic zone concept for REBOA placement.2 This concept was theoretically created with consideration of the bleeding area and blood supply of abdominal organs. An animal study demonstrated that response to arterial blood pressure and lactate is extremely different with REBOA placement between zone 1 and zone 3.3 Most of the REBOA guidelines recommend that REBOA should be placed at zones 1 and 3, depending on the location of the hemorrhage or hemodynamic status.4–6 Placement at zone 2 should be always avoided for preservation of gastrointestinal perfusion. Gastrointestinal hypoperfusion is not only considered the cause of intestinal necrosis but also the trigger for acute respiratory dysfunction syndrome and multiorgan failure associated with hemorrhagic shock.7 8 Aside from gastrointestinal ischemia, REBOA insertions and placement can cause serious complications, such as kidney failure, vascular injury, spinal cord injury, and limb ischemia.9 10 Thus, REBOA should be placed at an appropriate location to preserve visceral blood flow and to avoid complications.
Several studies and endovascular management courses describe REBOA deployment technique, but the proper REBOA placement still remains a challenging procedure.2 11 Ideally, the catheter position for REBOA placement should be confirmed via fluoroscopy, but it is not commonly available in emergency trauma bays and a prehospital field. Therefore, several fluoroscopy-free methods using portable X-ray, ultrasonography, or fixed-distance model have been proposed.10–14 In our hospital, REBOA insertion length is estimated with the external measurement method using the REBOA catheter and target aortic zone (online supplementary file 1). This is a simple and easy method and can be performed by a single operator without using special equipment. Some CT morphometric and cadaver studies validated the usefulness of the external measurement method, but its accuracy and safety have not been validated in a clinical model.15–17 From the safety and accuracy perspectives, the optimal placement method for REBOA needs to be discussed. Thus, in this study, we aimed to describe our experience and evaluate the accuracy and safety of REBOA placement using the external measurement method in clinical practice.
Supplemental material
Patients and methods
Data source and patient selection
In this single-center retrospective descriptive study, all patients who underwent REBOA from April 2008 to December 2018 at a Japanese major trauma center authorized by Yokohama City Emergency Committee (Saiseikai Yokohamashi Tobu Hospital, Yokohama, Japan) were screened. Patients who underwent REBOA were identified from our prospectively maintained trauma registry, and patients who underwent fluoroscopy for REBOA placement were excluded.
Outcome and data collection
Patients were classified into two groups according to the target zone for REBOA placement: zone 1 and zone 3. We used an existing proposed aortic zone classification for REBOA.2 Demographics and injury-specific factors were collected and compared between the two groups. The following data were collected for this study: age, sex, mechanism of injury, systolic blood pressure (SBP), heart rate, Glasgow Coma Scale, Injury Severity Score (ISS), dead on arrival, main bleeding source, size of the catheter sheath, operator specialty or seniority, REBOA placement zone, complications, and mortality. In terms of operator seniority, we recorded the postgraduate year as when they performed the procedures because this was a long-term study. The REBOA placement zone was classified into zones 1, 2, and 3 and others for outcome. The primary outcome was the placement accuracy for the target zone. Moreover, we compared patients’ characteristics, technical characteristics, and clinical outcomes between the non-target zone placement and target zone placement.
Management and procedure of REBOA
All patients were treated according to the Advanced Trauma Life Support Course guidelines. The attending Japanese board-certified emergency physician determined the REBOA indication and placement zone by evaluating each patient comprehensively, taking the vital sign, physical examination, and imaging findings into consideration. The REBOA procedure was routinely performed by an emergency physician who was board-certified in surgery or interventional radiology. Our trauma center has a unique system based on physician specialties. Most emergency physicians have either surgery or interventional radiology as a subspecialty and are qualified in either specialist field. Before Stannard et al reported the concept of the aortic zones of occlusion, we did not have the zone concept.2 However, REBOA positioning using the external measurement method had not been changed. All REBOAs were placed above the diaphragm before the introduction of the zone concept. Therefore, REBOA target zone data in the early 4 years were translated to the current zone concept, which is also known as target zone 1. The target zone for the REBOA placement was extracted from the medical record.
The REBOA catheter was inserted through the more accessible femoral artery with Seldinger’s technique. There are two commercial products for REBOA: IABO Block Balloon︎ (MERA Tokyo, Japan with a 10 Fr sheath) and Rescue Balloon︎ (Tokai Medical Products, Aichi, Japan) with a 7 Fr sheath. The device was randomly chosen, depending on the stock status in our hospital.
After sheath placement, external measurement using the REBOA catheter was performed to estimate the catheter length (online supplementary file 1). For zone 1 placement, the center of the balloon was placed at the level of the nipples and extended to the access site through the umbilicus. For zone 3 placement, the center of the balloon was placed at 5 cm above the umbilicus and extended to the access site through the umbilicus. External landmarks were determined based on previous anatomic study results.18 19 After the measurement, the catheter tip was inserted until the estimated length. The balloon was immediately inflated without confirming the radiographical test if needed.
Evaluation of placement accuracy for REBOA
In our clinical practice, all trauma patients ultimately underwent chest and pelvic X-ray scanning, regardless of whether they were dead or alive, in a primary trauma care setting. The REBOA placement zone was confirmed through X-ray imaging. The location of the REBOA for evaluation was set as where the center of the balloon is. When the center of the balloon was placed beyond a targeted zone, this was considered non-target zone placement. All X-ray images were transferred to a computer workstation (Shade Quest View R, Yokogawa Electric Corporation, Tokyo, Japan) and reviewed to ensure agreement between an acute care surgeon (SM) and an experienced faculty board-certified radiologist (TF) who were unaware of the patient outcome.
Although the aortic zones were classified by the location of each artery branch, all patients did not undergo angiography. Therefore, we used the perceptible vertebral landmarks on electronic X-ray images as the main branches of the aorta to mark the boundary between each zone. These vertebral landmarks were set based on previous anatomic study results.20–24 The boundary of the zone on the X-ray image was defined as follows: (1) the superior boundary of zone 1 is the midlevel of the T4 vertebra; (2) the inferior boundary of zone 1 is the midlevel of the Th12 vertebra, (3) the inferior boundary of zone 2 is the L1–L2 intervertebral disc level; and (4) the inferior boundary of zone 3 is the midlevel of the L4 vertebra (online supplementary file 2). To evaluate a distribution, the REBOA position was measured at the vertebral level on electronic X-ray images. The positions were divided into 21 groups according to their deployed vertebral levels from the T5 level to the L3 level.
Supplemental material
Statistical analysis
Data are presented as medians with IQRs or as counts and percentages. Pearson χ2 test and Fisher’s exact test were used as appropriate to compare categorical variables. The results were reported as relative risk for non-target placement and 95% CIs. Quantitative variables were compared by the Mann-Whitney U test. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS for Windows V.24.0.
Results
Patient selection and characteristics
During the 11-year study period, a total of 38 patients met the inclusion criteria. The clinical characteristics of the patients are summarized in table 1. All patients underwent REBOA placement as an adjunct in the management of trauma hemorrhagic shock. Eleven operators (seven surgeons and four radiologists) performed the REBOA procedures. The mean number of REBOA deployment procedures per operator was 3.5±1.7. Of the 38 patients, 30 (78.9%) underwent REBOA for target zone 1 and 8 (21.1%) underwent REBOA for target zone 3. The population was predominantly male (71.1%) with a median age of 42 years (IQR 25–55) and a median ISS of 34 (IQR 23–45). The mechanism of injury was predominantly blunt trauma (92.1%). The median SBP at admission was 72 (IQR 40–95) mm Hg. With respect to the main bleeding source, REBOA was frequently used mainly for the abdominal (44.7%) and pelvic (36.8%) regions. At each targeted REBOA zone, the proportion of abdominal bleeding source in the target zone 1 group was significantly greater than that in the target zone 3 group (56.7% vs. 0%, p=0.001). On the contrary, the proportion of pelvic bleeding source in the target zone 1 group was significantly less than that of the target zone 3 group (20.0% vs. 100.0%, p=0.001). In addition, only patients in the target zone 1 group switched from resuscitative thoracotomy (30.0% vs. 0%, p=0.159). Beside these characteristics, no significant associations were found between the target placement zone and patient characteristics or technical characteristics.
Patient and injury characteristics
Accuracy of REBOA placement for the target zone
The REBOA zone placement and clinical outcomes are shown in table 2. Overall, the REBOA placement accuracy for the target zone was 71.1%. The accuracy did not remarkably vary during the study period (online supplementary file 3). The in-hospital mortality was 57.9%, and majority of deaths occurred within the first 24 hours (86.4% (19 of 22 patients)). At each target zone, the REBOA placement accuracy for target zone 3 was significantly lower than that for target zone 1 (12.5% vs. 86.7%, relative risk 6.56, 95% CI 2.54% to 17.0%, p<0.001). Overall, the proportion of REBOA placement was 76.3% in zone 1, 21.1% in zone 2, and 2.6% in zone 3. There was no placement other than the classified zones, but in two patients with zone 1 placement, a portion of the REBOA balloon was located above the superior boundary of zone 1. The target zone 1 group had a higher proportion of patients with REBOA-related complications (6.7% vs. 0%) and higher mortality (66.7% vs. 25.0%), but these differences were not statistically significant.
Supplemental material
Accuracy and clinical outcomes for REBOA placement
The distribution of REBOA placement is shown in figure 1. REBOA in the target zone 3 group was more proximally placed to the target zone; REBOA in the target zone 1 group was more distally placed to the target zone.
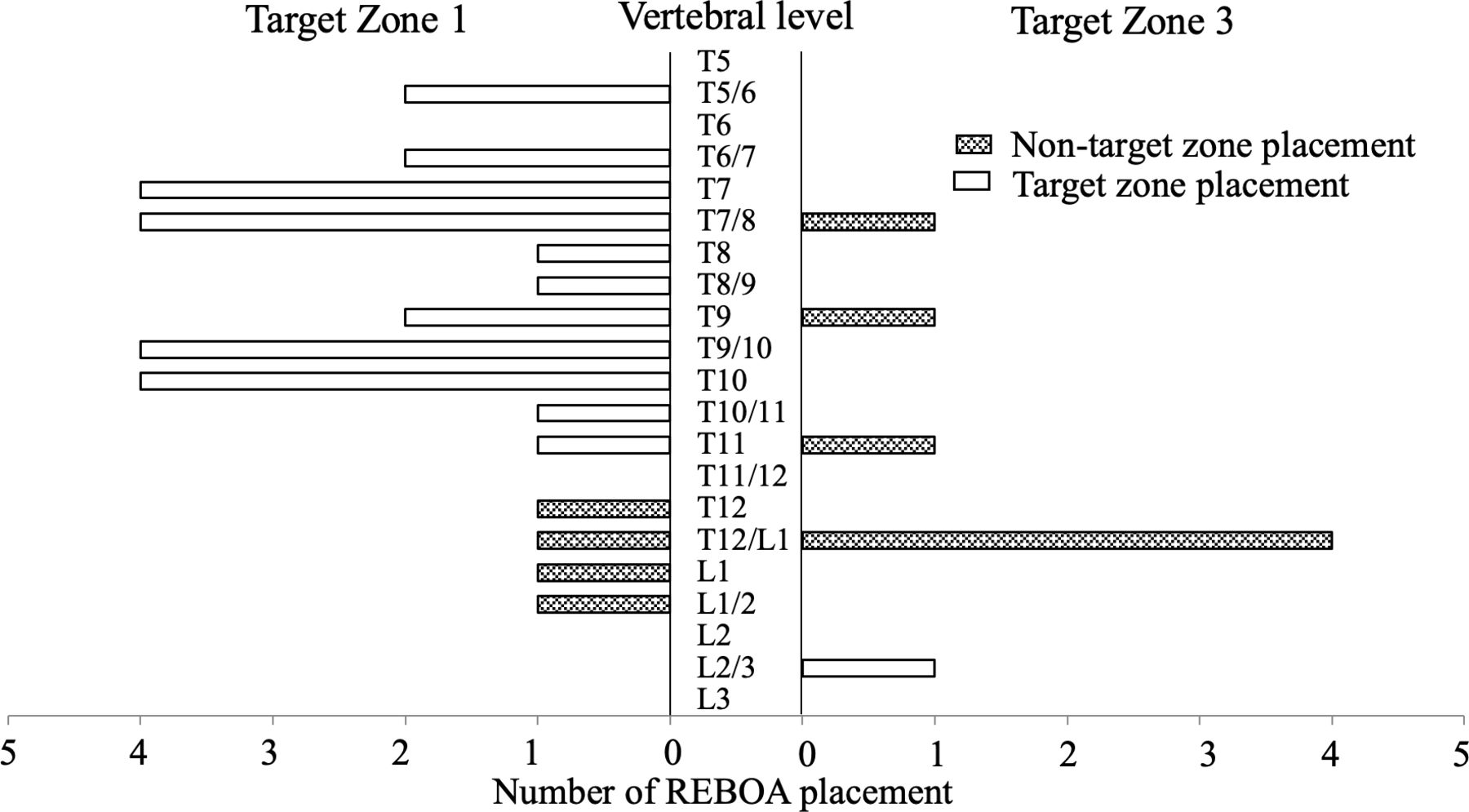
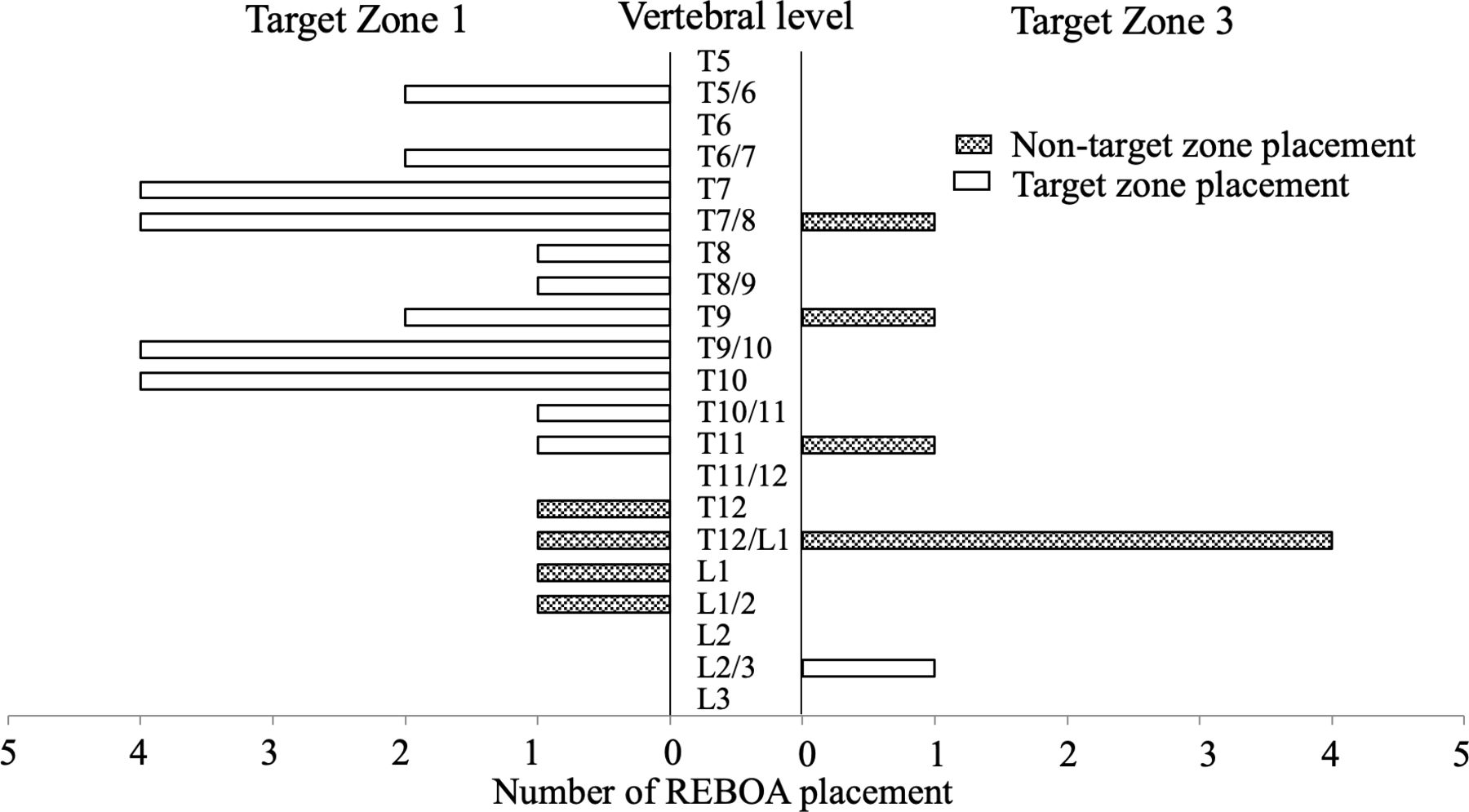{kind=link}
Distribution of REBOA placement using vertebral level on the electronic X-ray images. REBOA, resuscitative endovascular balloon occlusion of the aorta.
To assess the risk factor and clinical outcomes for non-target zone placement, table 3 shows the comparison between non-target zone and target zone placement groups. No significant associations were noted between the non-target zone placement and patient characteristics or technical characteristics. Two patients had REBOA-related complications. Each of the two patients had aortic dissection and compartment syndrome of the insertion side of the lower leg, respectively, both of which were not in the non-target zone placement. Moreover, the 24 hours and in-hospital mortality rates were not affected by non-target zone placement.
Comparison of clinical and procedure factors and outcomes between non-target zone placement and target zone placement.
Discussion
We described our experience of using REBOA by employing the external measurement method in 38 severe trauma patients in a Japanese major trauma center during an 11-year period. We also focused on the accuracy of REBOA placement using the external measurement method in the actual clinical practice. The results of this study showed that the REBOA placement accuracy was 71.1%. At the target zone, the accuracy of REBOA placement for target zone 1 was 86.7%, but the accuracy for target zone 3 was 12.5%.
In this study, 72.7% of the non-target zone placement (8 of 11) was located at zone 2, but there was no obvious intestinal ischemia. This study also showed that the non-target zone placement seems not to be related to survival outcomes and complications. However, we think that the mistaken zone 2 placement must have negative effects on outcomes. Although there are few reports about gastrointestinal ischemia caused by REBOA zone 2 placement, an animal study demonstrated that the difference in REBOA deployment location increased, required crystalloid fluid administration, and was associated with metabolic complications.3 Moreover, deployment at the level of the superior mesenteric artery (SMA) in zone 2 is thought to be pathophysiologically similar to acute SMA occlusion. In addition, balloon inflation times would significantly influence ischemic complications. Additional research is needed to analyze the negative effect of zone 2 placement.
Several methods for balloon positioning have been proposed. Each method has its own advantages and disadvantages (online supplementary file 4). Balloon positioning methods are roughly divided into imaging-guided method and blind method. Imaging-guided methods are more reliable than blind methods. However, the optimal method should be chosen depending on the situation and medical resources. These imaging-guided placements are also available in conjunction with the external measurement, but the combination may be helpful.
Supplemental material
The external measurement method and fixed-distance model can be used as a blind method for REBOA positioning. Both methods do not need any special equipment and are available in a prehospital setting. Several studies have proposed a fixed REBOA catheter insertion length with morphometric and cadaver anatomic analysis.14 25 26 A French study with CT morphometric analysis reported that REBOA placement using the fixed-distance method has a success rate of >94% in a general population.14 Considering our results, compared with the external measurement method, the fixed-distance model is expected to place the REBOA more accurately. Validation studies for the fixed-distance model in actual clinical practice are required.
This study shows that the external measurement method had low accuracy for REBOA placement in target zone 3. Several reasons are considered to explain this finding. First, zone 3 is anatomically shorter than zone 1. The length of zone 3 is <10 cm according to some morphometric studies.14 26 This short length is a difficult challenge for a blind procedure. Second, physicians may intentionally place REBOA at a more proximal position for fear of balloon inflation inside the iliac artery. Thus, this study may show that all non-target zone placements are more proximal in target zone 3 than in the target zone. Third, the landmark point for zone 3 placement (at 5 cm above the umbilicus) might be too deep. Several reports suggested that the anatomic landmark for zone 3 is the umbilicus.10 27 However, a morphometric analysis shows that 97.5% of the patients would have a portion of or all REBOA balloons placed within the iliac artery, if the center of the balloon was positioned at the umbilicus.16 Fourth, several factors, including ethnicity, age, body habitus, and medical background may have significant effects on the aortic morphometry.28
The external measurement method may cause large measurement deviation, depending on the operator skills. Technical skills are very important for a successful operation. Surgical subspecialty and the number of operations are surgeon-specific factors associated with good outcome.29 However, this study shows no associations between the non-target zone placement and operator specialty or seniority. This may be because the REBOA procedure itself is relatively simple and easy; it is not a common surgical procedure; and the number of REBOA procedure that each physician can perform is limited (mean 3.5±1.7 per physician in this study). Thus, physicians may find it difficult to acquire a lot of experience of using REBOA.
The primary limitations of this study are its small sample size and single-center retrospective design covering a long period. Although REBOA is currently one of the most popular resuscitative modalities in Japan, the small number of patients with REBOA (n=38) underpowered the study. Thus, the study result needs to be externally validated. A multi-institutional trial will be helpful in resolving this limitation. Second, the perceptible landmark used on X-ray image as the boundary between each zone may not be consistent with the real main branches of the aorta. For example, the inferior boundary of zone 2 in this study is the L1–L2 intervertebral disc level based on previous anatomic studies of renal artery origins.21 23 However, renal artery variations are common. The renal artery in approximately 60% of patients arose from the adjacent L1–L2 intervertebral disc level. The exact location of the renal artery is identified only with angiography or CT. Finally, our external measurement method may be different from other hospitals, particularly in the setting of the anatomic landmarks for REBOA placement.15 17 The sternal notch, xiphisternum, nipples, umbilicus, and pubic tubercle are common REBOA placement landmarks. Moreover, the estimated length differs, depending on whether the catheter is placed on a straight line or slightly bent through the umbilicus. Further studies are needed to clarify the optimal external measurement method for REBOA placement.
In conclusion, this study demonstrated that REBOA placement accuracy using the external measurement method for target zone 1 was high, but it was low for target zone 3. Zone 2 placement accounted for the majority of the non-target zone placements, but complications and mortalities related to non-target zone placement were not recorded. Our analysis suggests that the external measurement method appears to be unreliable for REBOA zone 3 placement. A novel procedure needs to be developed for REBOA placement for target zone 3, and further external validation of our study findings is warranted.
Acknowledgments
The authors gratefully acknowledge Ayaka Hayashi and Yayoi Miura from the Office of Research Administration at Saiseikai Yokohamashi Tobu Hospital for their assistance on drafting and critically editing this article.
References
Footnotes
Presented at This study was accepted as a poster presentation at the 78th Annual Meeting of the American Association for the Surgery of Trauma (AAST) in Dallas, Texas, on September 18, 2019. However, this was not presented due to a private issue.
Contributors SM, TK, and TF participated in the study design. SM and TO participated in the analysis and interpretation of data. SM, TM, and KS participated in drafting the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This retrospective study was approved by our institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. No data are available.