Article Text

Abstract
Background Early cholecystectomy (EC) for acute cholecystitis (AC) is standard. Often patients with cancer are not EC candidates and require non-surgical treatments. We analyzed factors associated with non-surgical treatments and progression to interval cholecystectomy (IC).
Materials and methods We performed a case–control study reviewing consults for AC from 2001 to 2017 in a tertiary cancer center. Study patients had cancer, abdominal pain, and positive imaging studies. Univariate analysis and regression modeling evaluated associations between non-surgical management, resolution of AC, and IC.
Results 206 patients met the criteria. 20 underwent EC, 132 took antibiotics (ABX), and were treated with 54 percutaneous cholecystostomy tubes (PCTs). AC resolution was higher with PCT versus ABX (94% vs. 80%, p=0.02). Univariate analysis revealed higher absolute neutrophil counts (ANCs) and longer length of stay in PCT, and logistic regression revealed independent associations of abdominal malignancy (OR=6.66, 95% CI 1.36 to 32.6, p=0.09), abdominal radiation (OR=0.09, 95% CI 0.02 to 0.53, p<0.01), and PCT with resolution of AC (OR=4.89, 95% CI 1.18 to 20.2, p=0.01). IC rate was 43%, and median time to IC after was 45 to 67 days. Multivariate analysis revealed nausea/vomiting and increasing platelets are independently associated with IC. Recent chemotherapy increases odds of IC in the presence of rising ANC (OR=1.14, 95% CI 1.00 to 1.30, p=0.05).
Conclusion PCT has a higher success rate of resolving AC than ABX. Abdominal malignancy increases odds of resolution; abdominal radiation decreases odds. Nausea/vomiting and recent chemotherapy, coupled with rising ANC are associated with IC, but less than 50% of patients return for operation. PCT may not be a bridge to IC in our population.
Level of evidence II.
- cholecystitis
- radiology, interventional
- treatment outcome
- general surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A free-standing cancer center still manages and treats general surgical problems but has the added complexity of patients with a cancer diagnosis. Patients with cancer represent a patient population that may not be candidates for early cholecystectomy (EC), and very little has been written about patients with cancer who present with acute cholecystitis (AC). Patients with cancer on active chemotherapy commonly present with neutropenia and thrombocytopenia, making them susceptible to impaired healing and bleeding. Neutropenic cholecystitis has been associated with higher postsurgical mortality rates, and thrombocytopenia can complicate operation due to difficulties with hemostasis.1 Technical factors associated with advanced-stage malignancy, such as tumor invasion of the gallbladder and porta hepatis, peritoneal carcinomatosis, and malignant ascites, present challenges to cholecystectomy, making certain patients ineligible for operation. Additionally, the poor prognosis of patients with advanced malignancy may alter surgical decision making as these patients may prefer non-surgical options over potential, postsurgical complications. The optimal management of patients with cancer with AC remains undefined.
In contrast, much is written about patients without cancer presenting with AC. The standard of care for most surgeons is to perform EC when patients present to the hospital. Unfortunately, patients who are not ideal surgical candidates due to delayed presentation and increased tissue inflammation, poor physiologic reserve, or functional capacity may prompt surgeons to treat such patients non-operatively on their initial encounter and pursue elective cholecystectomy after discharging the patient from the hospital. Although a recent meta-analysis showed that EC and interval cholecystectomy (IC) show no difference in morbidity and mortality, current evidence suggests that EC is favored because of reduced hospital stay and reduced risk of readmission.2–5 The advent of interventional radiology techniques introduced percutaneous cholecystostomy tubes (PCT) as valuable adjunctive treatment in patients who are poor surgical candidates.6 7 PCT placement works by decreasing distension of the gallbladder, mechanically draining bile, and allowing gallbladder wall inflammation and ischemia to subside. With the exception of sepsis from AC, large studies generally agree that PCT is an effective treatment for patients in whom cholecystectomy would not be considered.8–11 The need for IC has not been clearly demonstrated and data vary widely. Some authors have suggested IC will be needed due to recurrent symptoms from cystic duct obstruction in 21%–44% of patients, and others suggest that no further operation may be needed as the reported rate of success without relapse ranges between 55% and 88%.12–14 Thus, it is unclear if surgeons should perform cholecystectomy in potentially poor surgical candidates after PCT placement to prevent recurrent cholecystitis if less than half of patients experience a relapse in symptoms.
Our present study is exploratory, and its purpose was to compare the proportions of patients with cancer presenting with AC treated successfully with antibiotics (ABX) versus PCTs and their associated patient factors in our institution. Our secondary aim was to analyze the proportion of patients who returned for IC versus those who did not and their associated patient factors. We hypothesize that PCT, when compared with ABX alone, will be more effective in resolving AC in immunocompromised patients. We also hypothesize that PCT may be a bridge to IC.
Patients and methods
After obtaining institutional review board approval, billing records were used to extract patients who were consulted on for right upper quadrant pain, AC, or cholelithiasis between January 1, 2001, and August 31, 2017. Patients were included in the analysis if they had a cancer diagnosis, abdominal pain, and radiographic confirmation positive for AC. Imaging considered confirmatory for AC included at least one of the following: ultrasound demonstrating gallbladder wall thickening and/or pericholecystic fluid, CT or MRI demonstrating gallbladder wall thickening and/or pericholecystic fluid, or hepatobiliary iminodiacetic acid scan confirming a non-filling gallbladder. The presence of gallstones was not required for the diagnosis of AC as some patients only underwent CT scans, and cholelithiaisis may not appear on this modality, whereas gallbladder wall thickening and pericholecystic fluid do and are suggestive of AC. Although the presence of right upper quadrant pain alone could be considered as a variable for diagnosing and treating AC, nearly all patients had at least one imaging modality prior to surgical consultation, and positive imaging studies were oftentimes the reason for consultation. Thus, in our retrospective study, the presence of abdominal pain with a positive imaging study was considered diagnostic of AC.
Variable selection included age, sex, cancer history, the presence of nausea and vomiting, abdominal malignancy, abdominal radiation, length of stay (LOS), and American Society of Anesthesiologist (ASA) class. Age and sex have been associated with difficult cholecystectomy, and cancer type may affect whether abdominal operation is offered.15 Nausea and vomiting are common presenting symptoms of AC that may prompt surgeons to offer cholecystectomy as patients are not discharged if they cannot tolerate oral intake. The presence of abdominal malignancy was measured as otherwise physiologically fit patients may not be offered operation due to malignancy preventing safe access to the gallbladder. Similarly, the presence of abdominal radiation was measured as radiation changes to intestine raise concerns about safe manipulation of tissue, and may influence choosing a non-operative treatment course. LOS and ASA class are proxy variables for the general degree of illness among patients; sicker patients may have longer hospital stays and higher ASA classes.16
Our hypothesis is that mechanical decompression from PCTs, when compared with ABX alone, will increase the resolution rate of AC because it directly addresses the cause of AC. We also hypothesized that immunocompromised states would impair resolution of AC, as neutrophils are necessary for healing. As there is no formal definition of an immunocompromised state, we considered by the presence of hematologic malignancy, stem cell transplant, undergoing chemotherapy less than 6 weeks prior to presenting with AC, neutropenia, and steroid use to be reasonable proxy variables for immunocompromised patients. Being a tertiary cancer center with a high proportion of patients with hematologic malignancies, we felt it was important to look at variables specifically related to immunocompromised states in this population. Stem cell transplants are consolidative therapies to treat hematologic malignancies in remission, and they render patients immunocompromised until full engraftment of stem cells occurs. Recent chemotherapy was defined as having undergone chemotherapy less than 6 weeks prior to presentation per prior publications from our institution.17 A common side effect of chemotherapy is neutropenia; thus, recent exposure to chemotherapy prior to presenting with AC was measured. Neutropenia has been defined as an absolute neutrophil count (ANC) less than 1000 cells/μL; thus, we measured ANC as a potential covariate affecting resolution of AC.18 Steroid use has known immunosuppressive effects and is common in patients with graft-versus-host disease poststem cell transplant. Thrombocytopenia not only is a sign of malignancy but also can be associated with immunosuppressive chemotherapeutic agents, and may affect a surgeon’s decision to offer EC. Thrombocytopenia was defined as platelet count less than 50 000 platelets/μL.
Patients with AC who presented to the hospital were given three treatments, retrospectively, based on evaluation by the attending surgeon: observation on ABX, PCT placement in addition to ABX, and EC. The end of point of successful treatment was resolution of abdominal pain, toleration of oral intake, and discharge from the hospital. If abdominal pain did not resolve with the initially chosen treatment, surgeons changed to a different treatment. Success rates of initial treatment strategies were expressed as proportions of patients who did not require a change in treatment over all patients initially assigned to that specific treatment. EC was defined as cholecystectomy performed on the patient’s initial hospitalization. IC was defined as elective cholecystectomy after the patient’s initial hospital discharge after being managed non-operatively with ABX or PCT. IC was performed for recurrent abdominal pain, the presence of gallstones, cystic duct occlusion on post cholangiogram through the PCT, or in between cycles of chemotherapy to prevent disruption of ongoing chemotherapy regimens from recurrent cholecystitis. Post-PCT cholangiograms were performed 4–6 weeks postplacement per radiology protocol. The median time to IC after ABX or PCT was measured, because oftentimes cancer treatments are held by medical oncologists until the potential for recurrent episodes of cholecystitis is eliminated with IC.
Continuous data were compared using Student’s t-test for mean values or Wilcoxon rank-sum test for median values as indicated, and categorical data were compared using Fisher’s exact test given smaller number of observations. Multivariate logistic regression was used to analyze independent associations of resolution of cholecystitis to ABX versus PCT when adjusted for various patient factors. Univariate analysis between patients who underwent IC versus no IC was performed with Student’s t-test, Wilcoxon’s rank-sum test, and Fisher’s exact text where appropriate. Multivariate logistic regression was used to analyze independent associations of IC to baseline patient characteristics when adjusted for potential confounders. Regression modeling discrimination was tested with receiver operator curves. Kaplan-Meier survival analysis and Cox proportional hazards modeling was performed to look for significant differences in survival between ABX and PCT patients. A level of significance was specified as p<0.05.
Results
Of 340 consults for possible cholecystitis, 206 patients were studied based on the inclusion criteria of a cancer diagnosis, abdominal pain, and positive imaging studies. The majority of patients had hematologic malignancy (n=111, 54%), and specifically leukemia (n=43) (figure 1). One-fourth of the patients had abdominal malignancy (n=54, 26%), with the majority having pancreatic cancer (n=6).

Description of study population by underlying cancer diagnosis. Cancers making up less than 2% of the population: CNS, endometrial, gastric, sarcoma, adenoid, bladder, duodenal, esophageal, GIST, intestinal carcinoid, laryngeal, nasopharyngeal, osteosarcoma, prostrate, vulvar, Waldenstrom's macroglobulinemia. CNS, central nervous system; GIST, gastrointestinal stromal tumor; MDS, myelodysplastic syndrome; NET, neuroendocrine tumor.
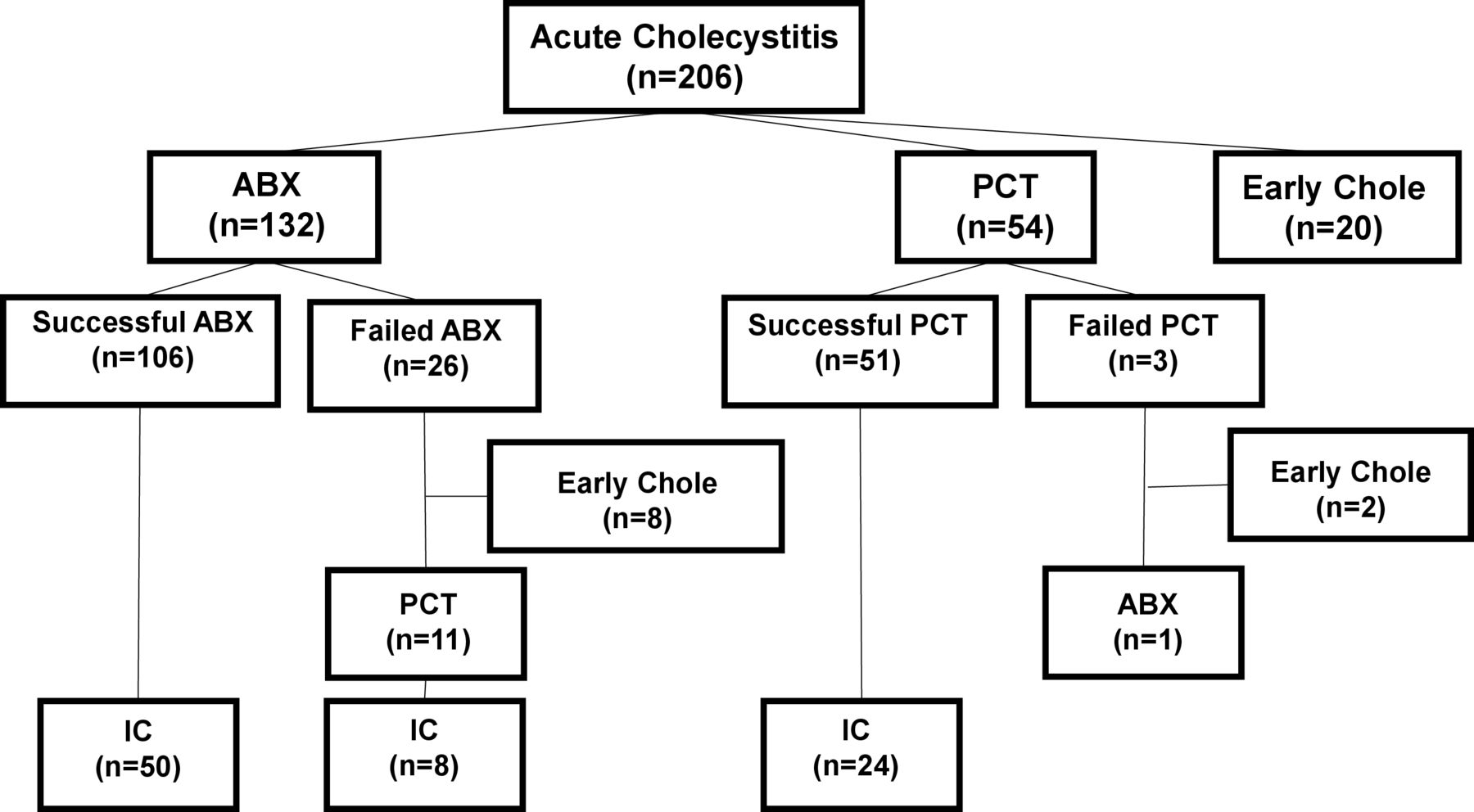
Chart review revealed that 132 patients were initially assigned to the ABX group, 54 to PCT, and 20 to EC (please refer to figure 2). The successful resolution of AC was 80% (106 of 132 patients) in the ABX group and 94% (51 of 54 patients) in the PCT group, and these proportions were statistically significant (p=0.02). There were 11 patients who proceeded to PCT after failing ABX alone (11 of 26 patients, 42%). On univariate analysis, higher median ANC was associated with resolution of AC by PCT (ANC=6.0×103 cells/μL, 95% CI 1.6 to 6.2, p=0.004) (see table 1). There was no difference in age, sex, the presence of abdominal radiation, or the proportion of patients with immunocompromised states between the two groups. LOS was statistically higher in the PCT group (8 days, IQR 6–12 days, p=0.02). ASA class was statistically different between the ABX and PCT groups, with the ABX group having a higher proportion of ASA III patients (p=0.04).
Univariate analysis of factors associated with resolution of acute cholecystitis with ABX versus PCTs

Non-randomized assignment of patients to surgical and non-surgical treatments for acute cholecystitis. legend: ABX, antibiotics; Chole, cholecystectomy; IC, interval cholecystectomy; PCT, percutaneous cholecystostomy tube.
On multivariate modeling, age and sex were included a priori in logistic regression due to prior evidence of their association with difficult cholecystectomy and presumed likelihood of pursuing initial non-operative treatment for cholecystitis. Abdominal malignancy and abdominal radiation were included in multivariate modeling by mathematics alone (p<0.20) as they represent potential confounding variables. All immunocompromised states were included in multivariate modeling because healing is tied to neutrophil counts that may be affected by any of the measured covariates comprising the immunocompromised states. In the context of a model including all specified predictors, abdominal malignancy is independently associated with increased odds of resolving AC (OR=6.66, 95% CI 1.36 to 32.6, p=0.02), and abdominal radiation is associated with decreased odds of resolving AC (OR=0.09, 95% CI 0.02 to 0.53, p=0.01). When compared with ABX and adjusted for potential confounders, PCT is independently associated with increased odds of resolving AC (OR=4.89, 95% CI 1.18 to 20.2, p=0.03). There were no independent associations between the presence of immunocompromised states, LOS, ASA class and resolution of AC (table 2).
Multivariate analysis of factors associated with resolution versus non-resolution of acute cholecystitis
Survival analysis revealed that 50% of patients in the EC group survived to 1490 days, 876 days in the ABX group, and 476 days in the PCT group. Figure 3 shows that ABX patients have a longer survival time than PCT patients (log rank test for survivor equality, p=0.02). Cox proportional hazard modeling revealed that PCT patients were more likely to die than ABX patients (HR=1.72, 95% CI 1.08 to 2.75, p=0.02).

{kind=link}
{kind=link}
{kind=link}
Survival time after initial diagnosis of acute cholecystitis. Log rank p=0.02. ABX, antibiotics; PCT, percutaneous cholecystostomy tube.
The total number of patients returning for IC was 67, and the total number of patients potentially eligible for IC was 157 (n=106 ABX, n=51 PCT). Thus, the total proportion of patients undergoing an IC was 43% (67 of 157 patients). The median time to IC after initial treatment is 45 days (IQR 27 to 118 days) for patients treated with ABX and 67 days (IQR 53 to 86 days) for patients treated with PCT, but this difference was not statistically significant, p=0.68.
Univariate analysis comparing patients who pursued IC versus those who did not revealed that patients presenting with higher platelet counts were more likely to undergo IC (p=0.02) (table 3). Although not statistically significant, patients undergoing IC appeared to have proportionately more patients that presented with nausea and vomiting (p=0.06) and fewer patients that presented with recent chemotherapy (p=0.10). Given these smaller p values (p<0.20), these possible associations were tested in multivariate analysis.
Univariate analysis of factors associated IC versus no IC
Multivariate modeling adjusting for associations between patients who underwent IC and those who did not included a priori inclusion of age and sex as these factors predispose patients to more difficult operation. The immunocompromised states were once again included in the analysis due to possible confounding effects on ANC and healing. Patients who initially present with immunocompromised states sometimes recover their ANC, and initial presentation with hematologic malignancy, stem cell transplant, and steroid use may have prompted selection for initial non-operative management followed by an elective IC. Factors eliminated from the multivariate model included the presence of abdominal malignancy, abdominal radiation, LOS, and ASA class because their p values (p>0.20) did not suggest they may be confounding variables. When adjusted for all covariates, initial presentation with nausea and vomiting was independently associated with undergoing IC (OR=2.30, 95% CI 1.09 to 4.86, p=0.03) (table 4). Additionally, ANC modifies the association of recent chemotherapy on IC. In the absence of rising ANC, recent chemotherapy is not associated with undergoing IC, whereas the presence of rising ANC increases the odds of IC after recent chemotherapy (OR=1.14, 95% CI 1.00 to 1.30, p=0.05). Rising platelet count was also independently associated with undergoing IC (OR=1.01, 95% CI 1.00 to 1.01, p=0.01).
Multivariate analysis of factors associated with IC versus no IC
Discussion
In a free-standing, tertiary cancer center, PCTs are associated with greater resolution of AC when compared with treatment with ABX alone. Our hypothesis that immunocompromised states are associated with decreased resolution of AC was not confirmed. When comparing the odds of resolving AC with ABX alone, PCTs have over four times the odds of resolving AC. An increased length of hospital stay was independently associated with patients treated with cholecystostomy tubes, and these patients had shorter survival.
Although no causal relationships can be analyzed from this study, possible causes for relative efficacy of PCTs versus ABX alone may be the mechanical decompression the gallbladder directly addressing the cause of AC, gallbladder distension and resulting gallbladder wall ischemia. The associations of abdominal radiation and abdominal malignancy with resolution of AC should be interpreted with caution. Very few patients had abdominal radiation, and the pronounced effect size on decreased resolution of AC may be spurious. Regarding abdominal malignancy, the association is not precise and has a wide CI. The odds of resolving AC are quite large, and the presence of abdominal malignancy may be a proxy variable for the better health of patients with abdominal malignancy in comparison with the high prevalence of patients with hematologic malignancy in our study population. Our population is skewed towards patients with hematologic malignancy who are often poor surgical candidates due to decreased functional status. Patients with abdominal malignancy may have higher likelihood of healing relative to leukemic patients, thus accentuating the association between resolving AC and abdominal malignancy.
There were some surprising associations on univariate analysis that were not independently associated with PCT on multivariate analysis. Undergoing chemotherapy less than 6 weeks to presentation with AC was thought to be a clinically significant factor for undergoing a PCT because it may render a patient immunocompromised and decrease surgical candidacy. Surprisingly, recent chemotherapy was not associated with undergoing PCT. Higher ANC was associated with PCT on univariate analysis, but was not independently associated on multivariate analysis. If PCT is used as a bridge to IC, it seems paradoxical that recent chemotherapy and lower ANC were not associated with undergoing PCT. The confounding variable may be recent improvements in chemotherapy, such as targeted or immunotherapy, that do not leave patients profoundly neutropenic. Some patients with PCT who underwent newer-generation chemotherapies may not have been profoundly immunocompromised.
We presume that increased LOS and decreased survival were associated with PCT patients because they were sicker. PCT patients have proportionally more ASA class IV patients, resulting in longer LOS. The decreased survival of PCT patients is consistent with patients being more ill. Although the higher proportion of ASA class IV patients in the PCT group may explain a lower survival rate, it is counterintuitive that these patients received a more invasive intervention and would be bridged to an IC in the future. Our original hypothesis that PCT may be a bridge to IC may not be correct. PCT may have been seen as a final intervention instead.
Our findings highlight that patients undergoing recent chemotherapy have decreased odds of undergoing an IC unless there is an increasing ANC. Clinically, this makes sense, as surgeons would be unwilling to risk operating in a patient who does not have potential to heal. This is consistent with previously reported associations between neutropenia, emergency operation, and increased postsurgical mortality. More notably, IC was performed in less than 50% of the patients eligible for the procedure, and initial non-operative management of cholecystitis resulted in a median delay to IC of 45–67 days. Medical oncologists often hold cancer treatments until IC is performed for fear of recurrent AC during periods of immune compromise or because strict treatment protocols require that patients do not have abdominal drains. If less than half of the patients received the perceived benefit of IC, further studies need to be performed to elucidate if delay in cancer treatment justifies pursuing IC.
There are several limitations of our retrospective study, including selection bias, unclear clinical decision making, small sample size, follow-up, time frame, and generalizability. There is selection bias as sicker patients were most likely assigned to non-operative treatments. Although surgical recommendations were often clearly documented, detailed rationale for clinical decision making was oftentimes terse, and surgeon preferences for non-operative management of AC could not be adjusted for. Attending surgeons taking call represented 14 surgical oncologists with primary specialties outside of the abdomen (melanoma, breast, and endocrine), and 21 surgical oncologists with specialties within the abdomen (liver/pancreas, gastric/HIPEC, colorectal, and sarcoma). Despite these classifications, however, surgeon preferences for management of AC may not necessarily relate to their named specialties. All patients who underwent PCT received broad-spectrum ABX; however, the rationale for antibiotic choice, duration, and whether or not cultures were tailored to bile cultures was not clear from chart review. The number of ABX patients not candidates for PCT was not collected, and decision making by interventional radiologists is not well documented. The small number of events given the 17-year time frame of the study may also represent a secular change. The acquisition of an electronic medical record during the latter period of the study captured more patients and accounts for imprecisions in measurement. Very little data exist regarding operative times, as a proxy variable for difficult operation, in the early parts of the study, making it challenging to compare operative times of EC versus IC to see if an increased operative time was a factor in choosing early versus interval operation. As a tertiary cancer center, we care for patients from geographically distant locations, and it is possible patients treated non-operatively may have had IC at other centers closer to them, and this may underestimate our IC rate. The long time frame of the study also does not account for advancements in treatment of AC and improvements in cancer-related mortality. Improvements in the skill of interventional radiologists may have also improved with time and, subsequently, the resolution of AC using PCT. Moreover, cancer care has improved and so has mortality; thus, it is difficult to account for how this may have increased IC rate. Whether a patient had active cancer versus a history of cancer was not a recorded variable given the limitation of a retrospective study; however, as the majority of patients had leukemia in our population, it is likely these patients had active malignancy undergoing chemotherapeutic trials. Lastly, our population is representative of a tertiary cancer center where the prevalence of patients with hematologic malignancy, stem cell transplant, and novel chemotherapeutic drugs is quite high. Although these findings may not generalize to a non-cancer center, they may serve as a substrate for study in cancer centers aiming to develop an acute care surgical program specific to their cancer population.
A strength of our study is that it demonstrates that surgeon-directed assignment of patients with cancer with AC to non-operative management can be effective in resolving AC. Although a statistical difference between PCT and ABX therapy exists, this may be less important clinically as the proportions of patients resolved by both treatments were well above 75%. The purpose of this exploratory study was largely hypothesis generating to develop future treatment pathways under a newly formed acute care general surgical service composed specifically of general surgeons in a center focused on cancer care. Given the clinical effectiveness of both ABX and PCT, it is reasonable to test pathways to decrease PCT placement by starting with administration of ABX prior to pursuing an invasive procedure. Placement of cholecystostomy tubes, although a valuable adjunct, was not associated with any particular patient factors except decreased survival. The use of PCT, aside from a terminal procedure, will need exploration. Our study also suggests that IC has low use and may even cause delay in cancer therapy; thus, the need to perform IC will be examined in future studies. Future study in the form of a quality initiative or randomized controlled trial is warranted to evaluate the clinical effectiveness of ABX versus percutaneous cholecystomy tubes in the treatment of acute cholecysitis, patient reported outcomes, and effects on delays in cancer care.
Conclusion
Historically, treatment of AC in a cancer center can be accomplished effectively with non-operative methods; however, PCTs were more effective in our center. The indication for PCTs as a bridge to IC is not convincing in our cancer population. Moving forward under a general operation acute care service, this exploratory study highlights the need to re-evaluate the appropriate use of PCTs and IC in the present era.
References
Footnotes
Contributors DS provided conception and design, data collection, statistical analysis, interpretation, and reporting. CRL and BB provided data collection and interpretation. AL and HG provided data collection.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the UT MD Anderson Cancer Center institutional review board, protocol number PA15-0098. Consent was waived as this is a retrospective review.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Deidentified patient data from chart review. All statistical analysis has been completed.