Article Text

Abstract
Background Thoracoabdominal trauma presents a diagnostic challenge for the emergency physician. The introduction of bedside ultrasonography (USG) provides a screening tool to detect hemoperitoneum, hemothorax, pneumothorax and pericardial effusion in torso injuries.
Aim To evaluate the accuracy of extended focused assessment with sonography for trauma (EFAST) for chest and abdominal injuries performed by first responders in a tertiary care hospital of Nepal.
Methods This was a prospective study including all trauma patients who obtained either an Injury Severity Score ≥15 or direct trauma to the trunk in 1 year period in the emergency department (ED) of Dhulikhel Hospital-Kathmandu University Hospital. The results of the EFAST were then compared with contrast-enhanced CT (CECT), radiology ultrasound (USG)/chest X-ray, or intraoperative findings when the EFAST was positive. The negative EFAST cases were observed for a minimum of 4 hours in the ED. Descriptive statistics and sensitivity, specificity, positive predictive value, negative predictive value and accuracy were calculated.
Results Out of 267 cases, 261 patients underwent an EFAST examination. The sensitivity and specificity were 94.8% and 99.5%, respectively. The negative predictive value was 98.53% whereas the positive predictive value was 98.21%. The overall accuracy was 99.4%.
Conclusion The results of this study suggest that EFAST examination performed by first-line healthcare providers is a useful method for assessment of thoracic and abdominal injuries. EFAST was found to have a high specificity (99.5%) and positive predictive value (98.21%) which indicates that it is an effective technique for detecting intra-abdominal or thoracic injuries. However, the effectiveness of EFAST is limited by its being operator dependent, and thereby human error. For negative EFAST cases, we recommend a monitoring period of at least 4 hours, serial fast scan, or further investigation through other methods such as a CECT.
Level of evidence Level I
- hemopneumothorax
- pneumothorax
- abdominal injuries
- lung injury
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Trauma is the leading cause of death globally,1 and the rates of trauma-related mortality and morbidity are higher in low and middle-income countries.2–4 Among traumatic injuries, abdominothoracic injuries are the most prevalent and can be fatal without rapid intervention. If intra-abdominal or intrathoracic bleeding is present, the probability of death increases by about 1% every 3 minutes that pass without intervention.5 Hence, delays in the treatment of trauma patients can be detrimental for patient outcomes. Thus, the initiation of treatment within the ‘golden hour’ after trauma is critical.6 However, the initial management of a person who is critically injured from multiple traumas is a challenging task for the emergency department (ED), and every minute can make a difference between life and death.7 Diagnostic peritoneal lavage (DPL) was historically used to detect free fluid (blood) in the peritoneal cavity.8 However, DPL is an invasive procedure and has more complications than the extended focused assessment with sonography for trauma (EFAST) examination. Similarly, a chest X-ray is used to diagnose free air/fluid in the pleural cavity. In the emergency setting, however, an erect chest X-ray is difficult to perform, and X-ray can easily miss minimal hemothorax and pneumothorax.9 Contrast-enhanced CT (CECT) remains the gold standard for diagnosing intra-abdominal and intrathoracic injuries, but CECT is an expensive and time-consuming test.10 Additionally, the patient needs to be transported out of ED for the CECT, which is unethical for hemodynamically unstable patients.
The optimal test, which is rapid, accurate, simple, non-invasive, and portable, is bedside ultrasonography (USG). It has been widely used in the ED for the assessment of trauma patients11 because it assists emergency doctors in making timely decisions and triaging the patients.12 It has also been incorporated into an advanced trauma life support course and added as an adjunct to primary survey.13
The EFAST facilitates the detection of hemothorax, hemoperitoneum, pneumothorax and hemopericardium in real time.14 Research conducted in different countries has shown EFAST to have excellent sensitivity and specificity for ruling out free blood in the pericardial, pleural and peritoneal cavities as well as in the diagnosis of pneumothorax in trauma victims.15–17 Therefore, the purpose of this study is to evaluate the sensitivity, specificity, negative predictive value, positive predictive value and overall accuracy of the EFAST technique for trauma victims in the ED. The main objective of the EFAST examination is to identify free blood in the abdomen/chest cavity or free air in the pleural cavity secondary to injuries by using portable USG.
METHODS
This was a prospective and observational study performed in the ED at Dhulikhel Hospital, Kathmandu University Teaching Hospital, which has an annual audit record of 20 000 patient visits in the ED. About one-third of patients are trauma patients. Trauma patients, who scored either an Injury Severity Score (ISS) ≥15 or who sustained direct trauma to the torso (table 1), were selected for the study.18
Criteria for direct trauma to torso*
Consecutive samples were taken from May 18, 2018 to May 19, 2019 after receiving ethical approval. With informed consent, participants were enrolled in the study. Non-trauma cases, patients under the age of 18 years, patients with isolated extremity injuries, pregnant women, patients whose intraoperative findings or whose chest X-ray/CECT abdomen or chest could not be assessed appropriately, EFAST scans performed by healthcare professionals who failed to correctly identify 10 subsequent cases after 2 hours of USG training, patients who were referred to another center without surgery or appropriate investigations (chest X-ray/USG/CECT abdomen/chest) in the ED and those patients who did not give consent were excluded from the study. Included patients were examined by emergency personnel who were trained in basic and advanced ultrasound. Emergency medical officers who had not received ultrasound training were given a 1 hour lecture and 1 hour hands-on training on EFAST by the principal investigator. A 2- hour session has been shown effective among residents of emergency medicine according to the residency-based ultrasound education of American College of Emergency Medicine.19 Hence, we structured a comparable training session for amateur medical officers with the evidence-based expectation that this training would be sufficient for basic competency in EFAST.19–21 Prior to enrollment, clinicians had the opportunity to perform and interpret 10 EFAST scans on trauma patients. Then, a registered radiologist ensured that each clinician acquired adequate interpretation skills for chest and abdominal ultrasounds. After the 2-hour ultrasound training, the trainees were evaluated based on how accurately they interpreted findings from 10 consecutive chest and abdomen trauma cases. Adequacy was defined on the basis of correct interpretation of all 10 consecutive cases of abdomen and chest trauma. The findings of those failing to correctly identify all 10 cases were excluded from the study. One of the medical officers was excluded from the study on this ground.
All patients who arrived in different triage zones of the ED were first assessed by a triage officer regarding all external injuries. At the end of the primary survey, the attending physician performed EFAST with Mindray ultrasound machine using a curvilinear probe (2–5 MHz) in a supine position. The ISS was then calculated after taking into account all of the internal injuries collected from reports from different departments such as radio imaging and surgery.
Care was immediately initiated when the patient presented to the ED, irrespective of whether or not the patient or his/her legal guardians consented to the procedures that were lifesaving. Neither incentives were provided nor was care delayed to obtain consent from the patients. For patients who were unconscious or not in the right frame of mind to give consent, consent was taken retrospectively from his or her legal guardian.
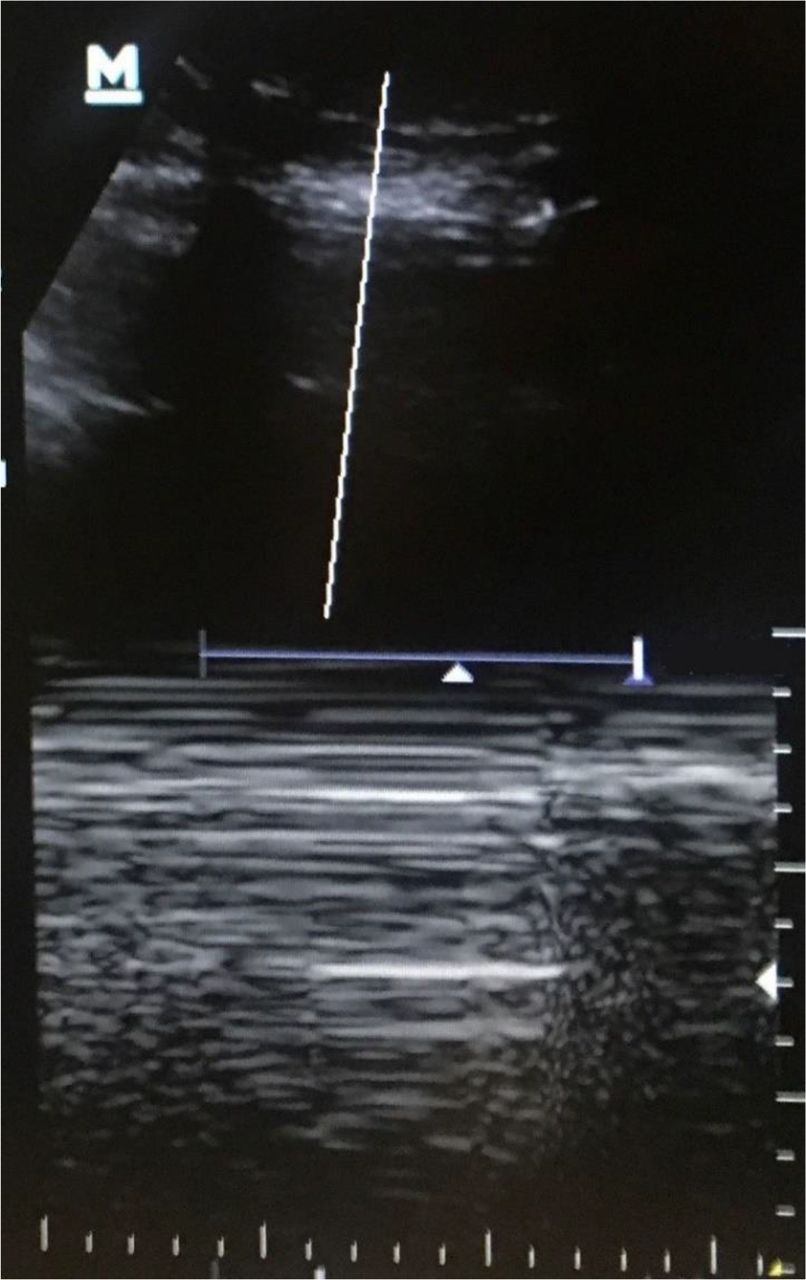
The following standard views were performed in each case: (A) right upper quadrant (RUQ) view (figure 1) to include Morison’s pouch and right pleural cavity, (B) subxiphoid view to see pericardial effusion, (C) left upper quadrant view to include splenorenal recess and left pleural cavity, (D) transverse and longitudinal pelvis view to visualize rectouterine pouch in female or rectovesicular pouch in male, (E) right anterior chest view (third and fourth intercostal spaces at a mid-clavicular line) to visualize right pneumothorax, and (F) left anterior chest view (third and fourth intercostal spaces at the midclavicular line) to see left pneumothorax. The ultrasound machine is available 24 hours a day, and the same ultrasound machine was used throughout the study period. The investigators ensured that the ultrasound investigation did not interfere or delay with resuscitation. The examination was classified as positive if the free fluid was seen in at least one view or if there was an absence of lung sliding in motion mode (M-mode) and visualization of bar code sign in ultrasound (figure 2).

Ultrasonography (USG) showing blood collection on right upper quadrant view.

Ultrasonography (USG) showing bar code sign in motion mode (M-mode) in anterior chest view for pneumothorax.
The presence or absence of lung sliding was saved in M-mode in ultrasound and printed out for data collection. All of the positive EFAST cases were managed in the operating theater, in the intensive or surgical intensive care unit or further investigated with a chest X-ray or chest/abdomen CECT as appropriate. The EFAST negative cases were kept for observation in the green triage zone for a minimum of 4 hours and then discharged if no clinical signs and symptoms of hemothorax, pneumothorax, hemopericardium and hemoperitoneum were present. The reassessment was performed if inclusion criteria were met and if clinical signs and symptoms were persistent or appeared later during observation. Patients underwent CECT and repeat EFAST examination as a part of additional workup. If injuries other than the chest and abdominal were present, patients were shifted to respective departments for appropriate care.
The EFAST examination was performed in real time. The EFAST results were subsequently compared with the attending surgeon/radiologist’s investigation method of choice—CECT, chest X-ray, USG, or laparotomy. The collected data obtained were analyzed on SPSS V.16.0. The sensitivity, specificity, and positive and negative predictive values of EFAST were calculated.
RESULTS
A total of 261 (72.4% male; 27.6% female) trauma patients underwent EFAST examination between May 2018 and May 2019 (table 2).
Demography of participants
The median age of presentation was 39 years (range 18–95 years). The leading cause (n=116, 44%) of trauma cases was due to road traffic crash (RTC) followed by fall injuries (n=112, 43%). Approximately 23% of patients arrived at the ED within 1 hour of the trauma occurring, whereas 77% presented after 1 hour.
The median ISS was 9 (IQR=13). Eighty-eight patients were enrolled for ISS ≥15, 169 for direct torso trauma and four for both ISS ≥15 and torso trauma. The time taken to perform EFAST ranged from less than 2 minutes (12%), 2–5 minutes (71%), and more than 5 minutes (17%) among the attending physicians. There were a total of 32 abdominal injuries, 22 thoracic injuries and 5 thoracoabdominal injuries. Among the five thoracoabdominal injuries, one was hemopneumothorax with hemoperitoneum and the other four were pneumothorax with hemoperitoneum. The former one underwent chest tube insertion and emergency exploratory laparotomy and the latter one underwent chest tube insertion and conservative management for hemoperitoneum. There were a total of 34 hemoperitoneum, 16 pneumothorax, 7 hemothorax and 1 hemopneumothorax cases. All patients with pneumothorax and hemothorax excluding one hemothorax case underwent intercostal drainage tube insertion. All patients were then shifted to the surgical unit for further management and observation. Patients (n=117) were observed for longer than 4 hours, and (n=144) less than 4 hours.
In our study, the first-line attending physician performed EFAST which resulted in a sensitivity of 94.8%, a specificity of 99.5 %, negative predictive value of 98.53%, and positive predictive value of 98.21%. The accuracy of the EFAST test was found to be 98.4% (table 3).
Comparison of EFAST with confirmative test
Among the ED primary care physicians, five were ED consultants who had received basic and advanced ultrasound training, and 12 were less experienced medical officer physicians who participated in a 2-hour ultrasound training on EFAST prior to enrollment in the study. When comparing the specificity and sensitivity among the two groups, the emergency consultants had a sensitivity of 100% and specificity of 98.6%, whereas the medical officers showed a sensitivity of 89.3% and specificity of 100%.
Among total trauma victims, five patients were hemodynamically unstable and underwent emergency exploratory laparotomy: one for unstable splenic injury, two for unstable liver laceration and two for small bowel injury. The remaining cases were hemodynamically stable so they were conservatively managed.
The results of EFAST were true positives for 55 patients as confirmed by one of the following: CECT of the abdomen only (n=26), CECT abdomen and laparotomy (n=3), CECT thorax only (n=5), CECT abdomen-thorax and laparotomy (n=1), CECT abdomen-thorax only (n=3), chest X-ray (n=16), CECT abdomen-thorax and chest X-ray (n=1) (figure 3). There was only one false-positive case in which the attending ED doctor suspected a renal cyst in the hepatorenal space for free fluid, but after negative confirmation by CECT, the patient was discharged. Of the 55 total EFAST true positive cases, the most common site for the fluid collection was hepatorenal space (n=26) followed by splenorenal space (n=21). Two hundred and twenty-seven cases were found to have no free fluid in the abdominal examination. The most common solid organ injuries in the abdomen were the liver (12 cases), spleen (12 cases) and kidney (2 cases) (table 4).

{kind=link}
{kind=link}
{kind=link}
Flowchart showing number of patients visited in emergency department (ED), EFAST test and number of confirmatory tests (CECT, laparotomy, ultrasonography performed by radiologist, chest X-ray) with EFAST. Patients aged <18, had isolated limb, neck and head injuries, ISS <15, were pregnant, difficult to do confirmatory test, referred, had denial of consent, scans of failing personnel, were dead during resuscitation, referred to another center for ICU and CECT, and had penetrating injury were excluded from the study. X-ray refers to chest X-ray. CECT, contrast-enhanced CT; EFAST, extended focused assessment with sonography for trauma; ICU, intensive care unit; ISS, Injury Severity Score; USG, ultrasonography.
Intra-abdominal organ injury
Among the 12 liver laceration injuries, 7 patients had grade III, 3 had grade I and 2 had grade II liver injury. Similarly, among 12 splenic injuries, 7 had grade I, 2 had grade III, 2 had grade IV, and 1 had grade II injury. There were only three cases of multiple organ injury within the abdomen. Grading of involved organ injury in multidetector CT is based on the American Association for the Surgery of Trauma.22
Of 205 EFAST negative cases, 1 underwent laparotomy, 7 CECT, 58 USG, 35 chest X-ray, and 104 USG and chest X-ray to confirm a negative result. In this study, there were three false-negative cases: two splenic injuries and one ileal injury with pneumoperitoneum.
DISCUSSION
This is the first study conducted in Nepal which assesses the diagnostic accuracy of EFAST test for blunt torso injury. The findings of the study suggest that EFAST is a useful tool to detect hemoperitoneum, hemothorax and pneumothorax in the initial management of trauma patients given its high sensitivity, specificity and positive predictive value. In this study, we found the sensitivity, specificity and positive predictive value of EFAST to be 94.8%, 99.5% and 98.21%, respectively. The sensitivity and specificity of EFAST, when conducted by emergency room consultants, were 100% and 98.6%, respectively. On the other hand, the sensitivity and specificity of EFAST, when conducted by medical officers who correctly identified 10 films of EFAST after 2-hour training on ultrasound, were found to be 89.3% and 100%, respectively. In a study conducted by Bode et al, the sensitivity, specificity and positive predictive value of EFAST were found to be 92%, 100%, and 100%, respectively.23 A similar study conducted by Hsu et al suggested the sensitivity, specificity and positive predictive value of EFAST were to be 80%, 100% and 100%, respectively.24 This provides evidence that EFAST can be regarded as one of the most reliable screening modalities to correctly identify free air in the pleural cavity or free fluid in the peritoneal, pleural or pericardial cavity.
Of the patients requiring EFAST in this study, the majority were male (72.4%), which is consistent with a similar study that showed 74% of the patients were male. This gender difference is further illuminated by the higher rate of disability-adjusted life-years from transport injuries in males versus females.25 A study conducted by Singh et al also demonstrated a male preponderance in RTC.26 This could be due to the greater participation of males in outdoor and high-risk activities such as driving, construction work, heavy lifting, and so on, as compared with females.
RTC (44.4%) and fall injuries (43.3%) were observed to be the most common mechanisms of injury. Similar studies performed by Shrestha et al and Payal et al suggested fall injury and RTC to be the most common modes of injury, respectively.7 27 This could be due to the proximity of Dhulikhel Hospital to the Araniko Highway, a major highway in Nepal. Additionally, our country’s hilly and mountainous terrain and difficult roads lead to RTC.28
Early diagnosis and timely intervention in trauma patients with chest and abdominal injuries can save lives.29 In this study, the majority of the EFAST examinations were performed within 2–5 minutes (n=185, 70.6%). In a study conducted by Tunuka et al, it was also found that most EFAST examinations were performed in under 5 minutes.16
Among chest and abdominal injuries, abdominal trauma is more common. Among intra-abdominal trauma, solid organs like liver/spleen are more commonly injured. In our study, the most commonly injured intra-abdominal organs in blunt trauma were found to be the liver and spleen, a result consistent with the study of Zwingmann et al.30 A study conducted by Arumugam et al demonstrated that liver is the most common organ involved followed by the spleen.31 Most of the traumas were managed conservatively and only a few patients were hemodynamically unstable and underwent emergency exploratory laparotomy, a result consistent with other research studies.32
Many of the trauma patients came more than 1 hour after sustaining the injury. This is due to overall infrastructural challenges within Nepal33 and the context that Dhulikhel Hospital primarily covers the remote areas of Sindhupalchok and Kavrepalanchok districts which have less accessibility to safe roads.34
Among the false-negative cases, the first case was a grade II splenic injury which was reported within 1 hour of the injury and yielded a positive EFAST result when the test was repeated a second time. The other false-negative case was an ileal perforation injury with pneumoperitoneum that underwent emergency exploratory laparotomy and loop ileostomy. EFAST has a limited ability to detect relatively small fluid collection during the early phase after trauma35 and it has low sensitivity to detect gut injuries, a result consistent with other study findings.36 37Also, EFAST is a subjective technique that requires a well-trained, competent, and experienced attending physician.17 Hence, repetition of EFAST after 4 hours of the initial examination and another modality of diagnosis such as CECT may be added along with repeated serial EFAST examination and closed clinical observation rules out any intra-abdominal injury.
There was only one false-positive case in our study in which fluid was seen in right Morison’s pouch but repeated EFAST scan was negative. The findings were then confirmed by CECT of the abdomen, and the patient was later discharged. EFAST was repeated whenever indicated as per the inclusion criteria and need for additional workup. Three repeat EFAST examinations along with CECT were performed for the sake of uncompromised patient care. Although repeat EFAST can be considered in a CECT resource-limited setting, the three cases of repeated EFAST documented in this study are not sufficient to form conclusions as to solely relying on the efficacy of repeat EFAST as a diagnostic modality. Further studies as to the efficacy of repeat EFAST in CECT resource-limited contexts are needed.
In the study by Akdemir et al, it was shown that ISS correlated with free fluid and hemodynamic status of the patient.38 In this study, patients who had either blunt trauma torso or an ISS ≥15 were included. It was found in the course of this study, however, that a proportion of trauma patients (61.3%) requiring EFAST examination had low ISS. This suggests that although ISS correlates with hemodynamic stability and presence of free fluid, ISS should not be the only parameter used in the assessment and introduction of EFAST examination in blunt trauma patients.
CONCLUSION
EFAST is a useful diagnostic tool for timely assessment of chest and abdominal trauma patients in the ED as it is a rapid, reliable and feasible method with high specificity and positive predictive value. It can effectively rule out hemoperitoneum, pneumothorax, hemothorax and hemopericardium. The EFAST examination tool is especially beneficial in the initial triage and assessment of trauma patients when evaluating the need for urgent surgery.
SIGNIFICANCE OF THIS STUDY
This EFAST diagnostic performance study in Nepal provides grounds to implicate its use as a diagnostic modality in torso injuries.
We recommend that EFAST should be adopted as the initial investigation tool to augment the clinical assessment of thoracoabdominal trauma in resource-limited countries where CECT is not readily available and not affordable for most patients.
LIMITATION
Despite measures taken to train the first-line responders in how to interpret EFAST scan, the interpretation ultimately depended on the individual knowledge and experience of the examiner as well as the external factor related to the patient.39 This study showed the risk of a false-negative result in gut injury patients and its inadequate ability to detect pneumoperitoneum.
Therefore, the use of advanced imaging modality such as CECT, serial EFAST examination or closed clinical monitoring should be sought to provide effective conservative or laparotomy treatment. In addition, emergency USG for trauma should be focused to perform EFAST and to see free fluid in front of the liver in RUQ view, paracolic gutters, or pelvic space along with closed clinical observation to rule out intra-abdominal injury. We also recommend that a negative EFAST should be repeated at least an interval of 4 hours, irrespective of the development of symptoms. Similarly, as the results differed between the groups who had extensive EFAST experience compared with those who only underwent a brief ultrasound training, there is a need for further EFAST training for the inexperienced group.
FUTURE DIRECTIONS
This study only focused on whether or not there was free air/fluid in the EFAST scan in the adult trauma victims. There was no attempt to examine visceral injury or quantify the amount of collected fluid or pediatric trauma population. Additionally, all pediatric patients were excluded from this study, and the efficacy of EFAST training on pediatric populations in Nepal should be explored in the future. One drawback of EFAST is its ineffectiveness to accurately detect hollow organ injury. Hence, contrast-enhanced USG may be useful to better visualize such injuries. In this context, the use of contrast-enhanced USG for detecting blunt trauma has yet to be explored.
Acknowledgments
The authors acknowledge the staff from the emergency, radiology, surgery and information technology departments of Dhulikhel Hospital for their contribution towards data collection for the study. Similarly, the authors express their sincere gratitude to Dr Wolfgang Blank from the German Society of Ultrasound, Dr Sushma Dahal from the National Health Research Center, Dr Rudolf Horn and Dr Susanne Morf from the Center da sanda Val Mustair, Switzerland, and Claire Jacobson for providing various support.
References
Footnotes
Contributors SB participated in study design, literature search, data analysis, data interpretation, writing and critical revision of the article. SKS participated in study design and critical revision of the article. RS, APS, and AP participated in study design and data analysis. LG, GS, and SB participated in literature search and data collection. All authors contributed equally in the critical revision of the article, and read and approved the final version of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study received ethical approval from the Institutional Review Committee of Kathmandu University School of Medical Sciences/Dhulikhel Hospital (approval number: 41/18).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.