Article Text

Abstract
Introduction Women are under-represented in the surgical disciplines and gender bias is believed to play a factor. We aimed to understand the gender distribution of membership, leadership opportunities, and scientific contributions to annual trauma professional meetings as a case study of gender issues in trauma surgery.
Methods Retrospective collection of membership, leadership, presentation and publication data from 2016 to 2018 Trauma/Acute Care Surgery/Surgical Critical Care (TACSCC) Annual Meetings. Gender was assigned based on self-identification in demographic information, established relationships, or public sources.
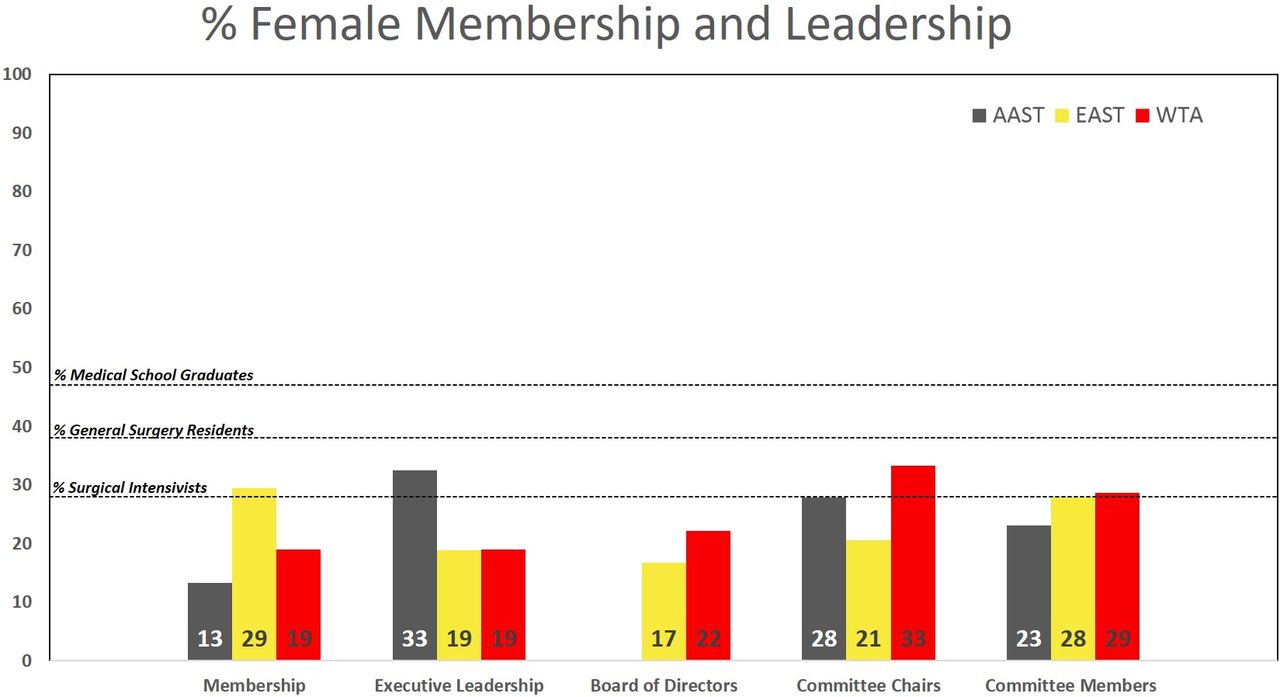
Results Women remain under-represented with only 28.1% of those ascertaining American Board of Surgery certification in critical care self-identifying as female. The proportion of female members in Eastern Association for the Surgery of Trauma (EAST) was comparable (29.4%), slightly lower for Western Trauma Association (WTA) (19.0%), and lowest for American Association for the Surgery of Trauma (AAST) (12.8%, p<0.05). In contrast, AAST had the highest proportion of female participants in executive leadership (AAST 32.5%, WTA 19.0%, EAST 18.8%) and WTA the highest for committee chairs (WTA 33.3%, AAST 27.8%, EAST 20.5%). AAST had the most significant increase in executive leadership during the last 3 years (AAST 28.6% to 41.6%). Invited lectureships, masters, panelists and senior author scientific contributions demonstrated the largest gap of academic representation of female TACSCC surgeons.
Conclusion Fewer women than men pursue careers in the trauma field. Continuing to provide mentorship, leadership, and scientific recognition will increase gender diversity in TACSCC. We must continue to promote, sponsor, recognize, invite, and elect ‘her’.
Level of evidence III, Epidemiology.
- gender
- trauma/ critical care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
According to the American Board of Surgery (ABS), women comprise only 28% of those certified in surgical critical care (SCC) and 22% of those certified in general surgery (GS) as of 2018. In contrast, half of all of those entering US medical schools during the last 10 years were women.1 2 While the etiology of persistent gender disparities in surgery is multifactorial, having female role models is a pivotal factor in ameliorating these disparities. The perception of how gender bias affects female advancement is a major influence in women choosing a career.3 Overt sexual harassment and explicit gender bias, which are viewed as unacceptable, have received considerable attention in recent years. Even more pervasive and subtle, however, is the contribution of implicit bias to continued gender disparity.
Implicit bias, or unconscious bias, has been shown to be common in surgical fields4 5 and occurs even when those involved are actively trying to avoid its perpetuation.4 6 Academic productivity is a key component of promotion and advancement. However, implicit bias has been shown to play a role in limiting female advancement. Women receive less extramural federal funding awards7 and less complimentary reviews compared with their male counterparts.8 The ‘glass ceiling’ is most difficult to break for surgical department chairs and full professors.6 Women are far less likely to be promoted to associate or full professor, and women make up a strikingly small percentage of medical school deans (16%) and department chairs (15%).7 Women are hired at lower salaries despite equal qualifications4 6 7 9 and leave academic medicine at a far higher rate than men.4
Increasing the visibility and quantity of female leaders is influential in driving more women to enter fields traditionally dominated by men.10 For the Trauma/Acute Care Surgery/Surgical Critical Care (TACSCC), women are increasing in numbers compared with all other surgical specialties. The highest annual increase per year over the last decade in female surgical trainees’ specialty choices was TACSCC as evidenced by 1.4% increase from 1994 to 2015.11 This success is tempered by the realization that despite this growth rate, women will not constitute an equal distribution of full professors in the larger field of surgery for at least 121 years11 and we lag behind internal medicine where this gender parity milestone will be achieved in 40 years.7 12
Knowledge of disparities is a first step toward combating explicit bias, revealing implicit bias, and achieving gender parity. Visibility within professional societies, recognition of scientific contributions, and leadership opportunities are important mechanisms to both increase gender representation and foster a network of female role models. There has been no in-depth contemporary analysis of the current state of women in TACSCC. The goal of this work was to conduct a current appraisal of female representation in our specialty and identify opportunities to facilitate additional steps toward gender equality in surgery.
Methods
The ABS was directly solicited for historical and up-to-date numbers of active diplomates in GS and SCC. Professional society membership demographic data were obtained from the the American Association for the Surgery of Trauma (AAST), the Eastern Association for the Surgery of Trauma (EAST), and the Western Trauma Association (WTA). These three organizations were chosen a priori as they represent voluntary professional societies most representative of the TACSCC community.
Assessment of current female representation in the field included available data from 2016, 2017, and 2018. Board certification (BC) data of self-reported gender were not recorded by the ABS until 2017. Member self-identified gender was used when available and classified as female, male, or not provided/unknown. When gender was not self-reported, membership rosters were used and cross-referenced against additional sources for verification.
Gender was determined by first cross-referencing the author or presenter name and affiliated institution if an academic profile was available. If an institutional profile was not available, internet searches were conducted for public sources that would indicate gender, including social media accounts and maintained professional profiles. Established interpersonal relationships among the authors were also used to determine gender. Open source materials for both medical student and in-training physicians were accessed including the Association of American Medical Colleges and the National Resident Matching Program. Each gender was independently determined by two separate reviewers.
Executive leadership was defined as an officer holding the title of president, president-elect, immediate past president, secretary, treasurer, or recorder of the society. Data on the board of directors were also collected with board positions defined by each society. Committee rosters were reviewed to quantify the number of female versus male committee chairs and members. Leadership data were provided in aggregate by gender for AAST and EAST from the executive office of each organization. Leadership data from WTA were compiled from publicly available committee and leadership rosters.
Representation at academic scientific forums was captured by reviewing the final scientific agenda for each organization’s national meeting over the study period. Two independent reviewers examined the program agendas and abstracts to manually extract the data on the gender of the first and senior author of each scientific presentation. Scientific podium full, quick shot, and poster presentations, as well as invited lectureships, speakers, discussants, moderators, and panelists were assessed.
Data were grouped by gender and professional society. Aggregate data were analyzed using analysis of variance to examine the difference between societies with significance determined at the p<0.05 level. Differences in the proportion of female members and women in leadership roles or presenter roles were tested using χ2 tests of association. Trends over time were also analyzed. Institutional review board waiver was granted for non-clinical/non-human research from Reading Hospital, Tower Health.
Results
In 2017, there were 29 001 certified diplomates of the ABS in GS. There was a 4.1% increase in the number from 2017 and 2018 (2018: 30 189). Although the absolute number also holding a BC in SCC rose in 2018 to 3453 from 3190 in 2017, the overall percentage of diplomates with dual BC fell to 8.75% in 2018 (from 9.0% in 2017; p=NS, not significant). By 2018, women constituted 22% of boarded GS and 28% in SCC (figure 1). Membership of women in the societies varied significantly. During the 3-year study period, women constituted 29.4% of EAST members, 19.0% of WTA members, and 12.8% of AAST members (table 1, p<0.0001).
Female membership and leadership of trauma and acute care surgery societies
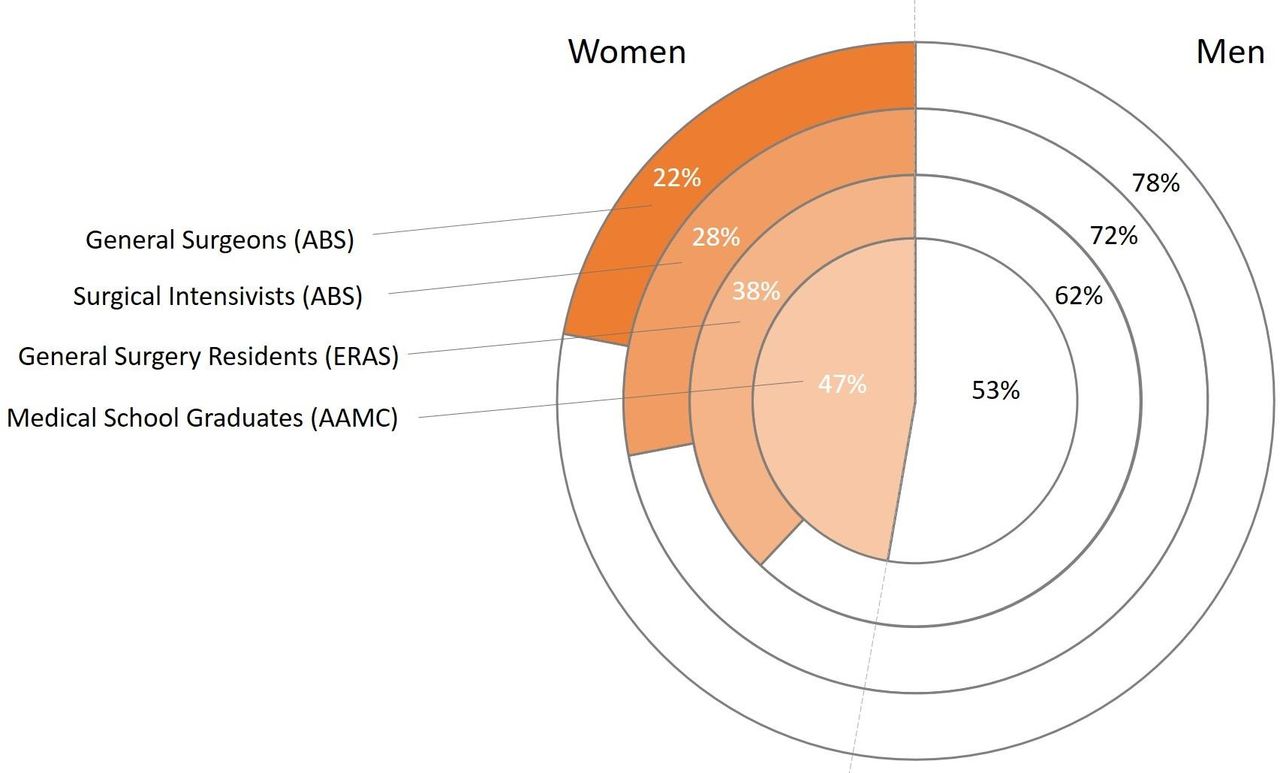
Gender trends in females entering trauma and acute care surgery. ABS, American Board of Surgery; ERAS, Electronic Residency Application Service; AAMC, Association of American Medical Colleges.
EAST reported a growth from 2016 to 2018 in the number of members reporting gender data from 1204 persons to 1434 with the rate of female representation of 27% in 2016, 28.8% in 2017, and 29.6% in 2018. By charter, the total number of members of the WTA is fixed and there was no appreciable change over the study period. However, the percentage of women increased very slightly from 18.9% to 19.2% (p=NS). AAST membership grew from 12.2% in 2016 to 13.3% in 2018 (p=NS).
Women holding leadership roles within the societies was variable. Compared with female membership numbers, women were under-represented in EAST board of directors and executive leadership roles. However, committee membership closely mirrored the percentage of female members (table 1). Women in WTA filled a higher percentage of committee chairs and committee members compared with membership distribution for females. Executive/board positions were similar to membership distribution. In contrast, although AAST had the lowest percentage of female members, in all leadership roles women were proportionately over-represented compared with membership numbers. Comparison within each category of leadership between societies was not statistically significant (table 1).
In addition to society leadership roles for women, we examined the visibility of women as invited experts. There was no difference across societies in the frequency of women filling these roles (table 2), and the number of women represented in these panels/lectureships mirrored the composition of the individual societies.
‘Expert’ roles for women at national meetings
Although women as invited discussants constituted a higher percentage than membership for both AAST and EAST (WTA has no discussants), EAST had a higher overall percentage, reflecting the difference in female membership distribution between the two societies.
An important component of promotion of women in academia includes presentation at the scientific forums of the national society annual meetings. Podium presentations by women were equally distributed across the societies (table 3).
Female representation at the scientific program of each society
Interestingly, within each society, the percentage of female podium presenters was significantly above the proportion of female members (figure 2). AAST demonstrated three times the membership percentage (40.2% vs. 13.3%, p<0.001), almost twice for WTA (34.4% vs. 19.0%, p<0.001), and 7.2% more for EAST (36.6% vs. 29.4%, p<0.05). Poster and quick shot presentations also exceeded membership distribution. However, a far smaller percentage of senior authors were women and it was lowest for WTA (p=0.022).
{kind=link}
{kind=link}
Distribution of females across trauma professional societies. AAST, American Association for the Surgery of Trauma; EAST, Eastern Association for the Surgery of Trauma; WTA, Western Trauma Association.
Discussion
The goal of this study was to use the current state of gender equality in TACSCC as a case study to highlight opportunities to improve gender diversity in surgery. Gender disparities in scientific fields are common. In 1998, Virginia Valian published Why So Slow, The Advancement of Women. This landmark book was trailblazing in its efforts to explain the role of gender schemas in gender imbalances in science. She noted these imbalances accumulate over time to the advantage of men.13 The book argued that simple recognition of stereotypes would lead to a change in progression of female leaders. However, decades have passed with literature still showing that gender disparity remains a prevalent issue.
Women will not seek environments or leadership opportunities where they perceive bias.3 In June 2019, the American College of Surgeons released its updated Statement on Harassment, Bullying, and Discrimination reiterating the mandate for a culture of respect and zero tolerance.14 Although explicit gender bias is recognized as unacceptable, implicit bias is much more pervasive and poorly recognized. Research has repeatedly shown that implicit bias is unconscious and happens even when one has the best intentions.4 Both men and women exhibit this implicit unconscious bias toward women.3 Thus, assessing the current state in our professional societies provides a foundation from which to identify successes and opportunities in promoting gender diversity.
Visibility of female leaders is an important factor in achieving gender equality. This has been shown to have a significant impact on decreasing overall gender bias,10 specifically by influencing the number of women choosing to enter the profession.3 Dr Molly Cooke noted in JAMA Internal Medicine in 2017 that if role models ‘do not mirror the sex and racial composition of the trainee pool, we are delivering the implicit but powerful message that these leadership roles and examples of excellence are for someone else.’3 Women make up nearly 50% of medical students yet the rate pursuing surgery has not appreciably changed. The reasons for this are certainly multifactorial, but one opportunity that professional societies likely impact is the visibility of female surgical leadership.
Societies play an incredibly influential role in establishing the reputation of those seeking promotion and providing a forum for highlighting academic or leadership accomplishment. Addressing implicit bias in these societies is a key factor in achieving gender equality. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) recently concluded that the proportion of female leaders within their organization was higher than the membership. However, women comprised only 21% of committee members, 18% of chairs, 16% of board members, and 14% of executives with only one female president.15 Our data demonstrate a similar trend to SAGES: women in leadership positions in TACSCC societies exceed the membership numbers during the last 3 years. TACSCC groups are also doing better in terms of committee membership (23.1% to 28.6%) and committee chairs (20.5% to 33.3%).
Although the leadership trends in our surgical societies are encouraging, women still only make up a small percentage of overall members. The net result is the pipeline of qualified women for leadership roles is constrained by the low number of women entering the field and joining the societies. In fact, for TACSCC this proportion is below the number of women seeking BC. Although some may choose career pathways in which society membership is not necessary, targeting tactics to increase diversity of membership will be key to progress toward equality. When one considers surgery as a whole, females with academic rank and in leadership roles are still increasing at a rate disproportionately slower than the increases in female medical students and surgery residents.16–18 Although the numbers are improving, surgical department chairs and full professors are still predominantly men.7 Women also only account for 18.4% of surgical program directors.16–19 Watching the future rate of women entering the profession and assessing how this parallels the recent exponential growth in the number of female department chairs during the last 5 years will provide important insight into the influence of female leadership roles in diversifying the future surgical workforce.
An area of particular success is our data demonstrating the female scientific speaker representation (30.1% to 40.2%) actually exceeds the proportion of female members. In comparison, a recent publication from Ruzycki et al reported a lower percentage of female speakers from 181 different medical/surgical conferences (24.6% to 34.1%). Further evaluation demonstrated surgical specialties had a 9.8% lower proportion of female speakers.10 For our trauma societies, scientific merit is judged in a blinded fashion without knowledge of author gender. The fact that the numbers exceed the rate of membership supports the notion that when one is unaware of gender, the science is judged more equitably.
Still, we found that senior authors were infrequently women, alluding to a potential leaky pipeline of female role models in research as one contributing factor. Women face unique challenges in pursing and maintaining scientific careers. These include receiving lower starting salaries,7 9 20 less institutional support for building research programs,7 9 20 fewer and less well-funded National Institutes of Health (NIH) grants,8 and have a slower rate of promotion even when controlling for factors that could impact academic productivity such as childbearing.7 The net effect is a smaller pool of female ‘experts’ at senior levels in whom to draw on for mentorship.
Female expert panelists in our TACSCC societies (17.9% to 23.7%) were lower than other medical/surgical groups as reported by Ruzycki et al.10 This is not unique to our TACSCC societies. At the American Burn Association (ABA) 50th Annual Meeting, Thompson et al reported that women bring new science to the ABA meeting in excess of membership proportion but remain under-represented or absent as moderators.21 An analysis of the Critical Care Conferences demonstrated only 5% to 26% of expert speakers were female physicians.22 Other surgical groups have reported higher rates of female moderators, including 28% at the recent American Society of Colon and Rectal Surgeons (ASCRS) meeting. Interestingly, at the ASCRS meetings, women tend to moderate more educational topics (48%) and be far less likely to be asked to lead technical sessions.23
Our TACSCC societies have made a commitment over the last several years to make technical sessions or expert panels more diverse. For example, in the AAST, in 2011, 50% of expert panels were male only and this was driven to 0% in 2016. The avoidance of the ‘manel’, a term popularized in a June 12, 2019 New York Times article ‘NIH Calls for end to all-male panels of scientists’,24 is an important step forward in promoting gender diversity. TACSCC organizations have done better in addressing ‘manels’ compared with other surgical societies. For example, in the past 5 years, at the American College of Surgeons Clinical Congress (CC) and the Academic Surgical Congress (ASC), there has been no appreciable statistically significant change in the number of ‘manels’ (38% to 23% CC, p=0.4; 23% to 17% ASC, p=0.5).25 The deliberate choice to avoid male-only panels in our national trauma forums is only one of several important initiatives the TACSCC groups are promoting.
Within the trauma community, both the EAST and the AAST have increased efforts to address diversity and equity issues in our profession. In his 2018 EAST presidential address, Dr Andrew Bernard focused on equity and put his executive mission into action with creation of the Equity, Quality, and Inclusion in Trauma Surgery Practice Ad Hoc Task Force, colloquially known as EAST4ALL.26 Dr David Spain, current president of the AAST, announced at the 2019 annual meeting the formation of the Ad Hoc Committee for Inclusion and Diversity. In loud calls to action, these leaders have challenged the community to reflect inward to establish a foundational assessment of our current state and identify strategic opportunities to address gender diversity issues. To achieve equality in our organizations for both men and women, we must consider our own collective and individual responsibilities for creating opportunities for all to excel.
Limitations to this work include the lack of available source material. All involved groups have not historically tracked gender information making it difficult to reflect the changes over a longer period than the 3 years in this study. Additionally, stratification by participant age was not possible due to a lack of source material provided by the societies or ABS. Thus, looking across three differing societies with complimentary but distinct membership criteria provides the best current mechanism available for understanding the role of age/experience with this issue.
Further, we were reliant on manual counts and personal relationships or public profiles to ascertain some demographic data which may lead to error. Also, printed annual meeting program materials as compared with online resources did show minor discrepancies, and in some cases only one or the other was able to be fully analyzed. This was most applicable in full committee and membership lists, and explains the limited years chosen for this review. As our methods explain, lack of ease of access to multifaceted demographic information and lack of transparency prevent complete evaluation. Collecting demographic information in aggregate to analyze and dissect for the benefit of all members, rather than as a marker for individual classification, merit or appointment is a clear need. Until aggregate demographic information encompassing not just gender but other important factors where implicit bias is prominent (ie, race, ethnicity) becomes readily accessible, it will be difficult to appropriately address under-representation of these groups.
Conclusion
Fewer women than men pursue careers in the trauma field, although the numbers are increasing. Despite under-representation in the studied societies, the contributions of women are disproportionately high where the science is graded and chosen in a blinded fashion based on merit alone. Continuing to provide mentorship, leadership, and scientific recognition opportunities is an important component of increasing gender diversity in our field. We must continue to promote, sponsor, recognize, invite, and elect ‘her’.
Acknowledgments
Christine Eme, executive director, EAST, and Sharon Gautschy, executive director, AAST, for access and support throughout the process; Alison Muller, research coordinator, Reading Trauma Center, for administrative support.
References
Footnotes
Presented at Presented in part at the 78th Annual Meeting of American Association for the Surgery of
Trauma and Clinical Congress of Acute Care Surgery in Dallas, Texas, on September 20, 2019.
Contributors SMF, JK, and RAC participated in the literature search. SMF, JK, CGV, SB, DAJ, HS, JJC, and RAC participated in the study design. SMF, JK, CGV, SB, DAJ, HS, and RAC participated in the data collection. SMF, JK, SB, and RAC participated in the data analysis. SMF, JK, SB, HS, and RAC participated in the data interpretation. SMF, JK, and RAC participated in the writing. SMF, JK, CGV, RAC, DAJ, and HS participated in critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available public, open access repositories. Data are available upon reasonable request. Data are all extracted from publicly available resources.