Article Text

Abstract
Background Airway obstruction remains a preventable cause of death on the battlefield. Surgical cricothyroidotomy is an essential skill for immediate airway management in trauma. Training for surgical cricothyroidotomy has been undertaken using simulators, cadavers or animal models. The ideal approach to training for this low volume and high-risk procedure is unknown. We hypothesized that current simulation technology provides an equal or better education for surgical cricothyroidotomy when compared with animal tissue training.
Methods We performed a prospective randomized controlled study comparing training for surgical cricothyroidotomy using hands-on training on swine versus inanimate manikin. We enrolled medical students who had never performed or had formal instruction on surgical cricothyroidotomy. We randomized their instruction to use either a swine model or the inanimate version of the Operative Experience Inc. advanced surgical manikin. Participants’ skills were then evaluated on human cadavers and on an advanced robotic manikin. Tests were scored using checklists modified from Objective Structured Assessment of Technical Skills and Tactical Combat Casualty Care. We compared scores between the groups using Wilcoxon rank sum tests and generalized linear models.
Results Forty-eight participants were enrolled and trained; 30 participants completed the first testing session; 25 completed the second testing session. The mean time to establish an airway from the incision until the cuff was blown up was 95±52 s. There were no significant differences in any of the outcome measures between the two training groups.
Discussion Measured performance was not different between subjects trained to perform surgical cricothyroidotomy on an animal model or a high fidelity manikin. The use of an advanced simulator has the potential to replace live tissue for this procedure mitigating concerns over animal rights.
Levels of evidence I
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
First responder care rendered to a casualty in prehospital settings is important to ultimate survival. Most combat-related deaths occur in the prehospital setting before the casualty reaches a military medical facility.1–5 Airway obstruction ranks third as a preventable cause of death on the battlefield following severe hemorrhage and tension pneumothorax.1 Review of modern military conflicts suggest that airway compromise accounts for 1%–2% of total combat fatalities.3 6 7 In a study by Adams et al,8 from Operation Iraqi Freedom, 5.8% of 293 casualties needing advanced airways received a cricothyroidotomy. Other data from Mabry indicate that 18 of 982 battlefield casualties had airway compromise as the most likely primary cause of death. Of these 18 casualties, all had traumatic injuries to the face and neck and nine had multiple injuries to major vascular structures with significant hemorrhage.9 Airway management is a top priority in initial resuscitation of these casualties, and it is literally the difference between life and death.10 11 Airway control is one of the few procedures in prehospital emergency care that significantly affects outcome.12
Combat first responders are currently trained to provide trauma care in the tactical environment using the principles of Tactical Combat Casualty Care (TCCC), and these principles and guidelines serve as the basis for predeployment training for operational medical and combat personnel. TCCC guidelines recommend the aggressive use of surgical airways when maxillofacial trauma makes the use of non-invasive airway techniques inadequate to open the airway,13 and surgical cricothyroidotomy is one of the essential skills taught to combat first responders. Unfortunately, not all surgical cricothyroidotomies are successful. One of the key factors associated with success rate is the effectiveness of training. Challenges associated with training include use of anesthetized animal whose anatomy is not similar to human anatomy.
We believe that currently available simulation technology has the potential to vastly improve the training of both military and civilian medics to perform surgical cricothyroidotomy when compared with currently used ‘gold standard’ of animal or cadaveric tissue training. Bowyer et al 14 found that a haptic enabled virtual reality cricothyroidotomy trainer significantly improved the confidence level of deployed medics and improved their understanding of the anatomy involved. This model allows individuals to ‘train as they fight’ a moving bleeding model with human anatomy.
The purpose of this study was to compare the outcomes of training for cricothyroidotomy using a live animal versus an advanced simulation model. We hypothesized that the advanced simulation model provides an equal or better education for surgical cricothyroidotomy when compared with animal model training.
Methods
Design
A prospective randomized controlled study with crossover design was used. Participants were allocated to each intervention group at a 1:1 ratio. All randomizations were computerized. IRB approval was obtained from the Johns Hopkins School of Medicine (IRB00046347).
Subjects
Medical students from the Johns Hopkins School of Medicine who had never performed or had instruction on how to perform a surgical cricothyroidotomy were eligible to participate in the study. The goal was to train true novices with limited surgical and procedural skills. Participants were excluded from the study if they had received formal training to perform cricothyroidotomy or if they had observed, assisted or performed one or more cricothyroidotomies during their training. The study was conducted in the minimally invasive surgical training and innovation center at the study institution where anesthetized pigs (swine model) and human cadavers were used for the routine training of surgical residents. Once the resident training was completed, the pigs were euthanized just prior to the beginning of our study. No additional pigs or human cadavers were used for this study.
Interventions
After a written consent was obtained from the eligible participants, the study was conducted in two phases: training and testing.
Phase 1 (training phase)
All participants where trained on how to perform a cricothyroidotomy using the standardized TCCC Curriculum for surgical cricothyroidotomy that composed of didactic and hands-on skills training. A 15 min long voice-over PowerPoint created by one author (MB) was used to provide the standardized didactic content. The participants were provided an opportunity to ask questions after the didactic presentation prior to hands-on skills training. Based on the randomization, participants received additional mentored ‘hands-on’ training to perform a surgical cricothyroidotomy on either the swine model (n=24) or on the inanimate version of the Operative Experience Inc. advanced surgical robotic manikin (n=24) where the manikin was neither bleeding nor moving.
Phase 2 (testing phase)
The second phase consisted of two sessions: testing 1 and testing 2. Trained participants were tested on a human cadaver or an animated version of the Operative Experience Inc. advanced surgical robotic manikin that had the capability to move and bleed for the first testing session and then the testing model was alternated during the second session (online supplementary figure S1). The animated version of the Operative Experience Inc advanced surgical robotic manikin comprised hyper-realistic materials with surgically correct human anatomy developed by the Operative Experience Inc (North East, Maryland; http://operativeexperience.com). It is commercially available and has a combat realistic transfacial gunshot wound with severe injury to the oral cavity, massive bleeding from the nose and mouth, air moving from the lungs through the airway and remotely controlled head movements (online supplementary figure S1). The model had a low cost modular neckpiece that can be replaced after each cricothyroidotomy attempt. The model is rugged but highly portable allowing for practice and testing in more combat realistic environments and conditions than an animal lab.
Supplemental material
During both testing sessions, the participants were given a brief introduction to the techniques involved with the performance of a surgical cricothyroidotomy. After which, a case scenario was provided to indicate the need for a criothryoidotomy, and the participants performed the procedure. The testing sessions were videotaped using a fixed camera on a bedside table as well as a head-mounted high-definition video camera (Looxcie) that the participant was asked to wear. All surgical cricothyroidotomy procedures were performed using the standardized Tactical CricKit favored by military medics (http://www.narescue.com).
Outcomes
Phase 1 (training phase)
The outcome for the training phase was the self-assessed confidence level measured using a confidence level questionnaire (CLQ). The CLQ comprised five items that the participants used to self-assess their comfort level with identifying and managing an airway obstruction, and their ability to secure an airway using non-surgical and surgical techniques. Each item was rated on a scale of 1–5, with 1 being ‘will not attempt skill’ and 5 being ‘will attempt while teaching it to another colleague’. The CLQ was administered before and after the training to assess for any increment in the self-assessed confidence level.
Phase 2 (testing phase)
An outcome for the testing phase was the participants’ technical skills level in performing a cricothyroidotomy measured using the Objective Structured Assessment of Technical Skills (OSATS) cricothyroidotomy and the TCCC skills instruments. The validated OSATS has 10 questions. Nine of them rate each step of the procedure as unsatisfactory or satisfactory. One question provides a global assessment of the participants’ performance by rating the overall performance on a scale of 0–5 with 0 representing failure and 5 representing outstanding. The validated TCCC instrument had 13 items that evaluated each step of the cricothyroidotomy procedure and was rated as unsatisfactory or satisfactory.
Outcomes measured during the testing phase were: (1) placement and securement, (2) procedural duration and (3) success of the procedure. The placement and securement data pertained to how the participant would determine whether the cricothyroidotomy tube was in place and how the tube would be secured. The procedural duration referred the time taken to complete the procedure served as the primary outcome for this study. The time taken to establish the airway from the time the instructor completes the case scenario until the cricothyroidotomy tube’s cuff was inflated and the time taken from the time an incision was made to the time the cricothyroidotomy tube’s cuff was inflated were measured in minutes. The success of the procedure was an assessment of the overall success of the procedure using three critical evaluation criteria: (1) ability to identify the location of the cricothyroid membrane, (2) ability to obtain a patent airway and (3) performance of the procedure is safe manner.
Sample size
A sample size of 48 participants was predicted based on the hypothesis that individuals who train on an inanimate manikin with human like anatomy would perform the skill faster than those who train on a live swine model. We predicted that the mean for the swine model trained group would be 65 s, and the mean for the inanimate manikin trained group would be 55 s with a sigma of 11 s. A sample size of ~20 for each group was calculated using a desired power of 0.80 and an alpha of 0.05 for this expected normal distribution comparison of two independent samples based on pilot tests. We increased the number of participants to 48 to account for potential participant attrition.
Randomization
The research identification numbers were randomized into either the inanimate manikin or the swine model training groups using an Excel-generated random numbers. The original random allocation sequences were stored in a password-protected folder on the institution’s server that only one study member VP was able to access. The participants were enrolled by a research assistant K.P. When a participant was enrolled in the study and had completed the didactic training, the study member VP informed KP regarding the allocation to intervention group based on the study identification number.
Blinding
Since the participants were able to see which model was used for training and testing, we were unable to blind them from the types of intervention. The recorded video sessions of the testing sessions were scored by two expert surgeons CJ and WRL who were not involved in the data collection. The two video reviewers were blinded to the type of training the participants received and the order of testing. They only knew whether the testing was done on a human cadaver or a robotic manikin. The two reviewers’ inter-rater reliability was 0.92 for the initial two scorings, and the overall inter-rater reliability of all scorings was 0.95.
Statistical methods
Descriptive statistics were used to analyze all variables. χ2 tests were used to compare categorical variables between two groups. Student’s t-test or Wilcoxon matched-pairs signed-rank tests were used to compare interval data between two groups depending on whether they were parametric or not. Generalized linear model testing using a log link was conducted to analyze for any significant differences in testing scores (OSATS and TCCC) by the type of training, type of testing and order of testing. Any interactions between type of training and type of testing were also explored. Akaike Information Criterion scores were also calculated to identify the most parsimonious model.
Results
Participant flow
Forty-eight participants were enrolled in the study from May 2016 to April 2017 and all 48 received the intended training in phase 1. In phase 2, 30 participants completed the first testing session, while only 25 participants completed the second testing session, and data were analyzed accounting for the those who were lost to follow-up (figure 1). Reasons why participants were lost to follow-up is listed in figure 2. The primary reason was scheduling conflict since these students were undergoing medical training and were not always available when the models were available for testing.
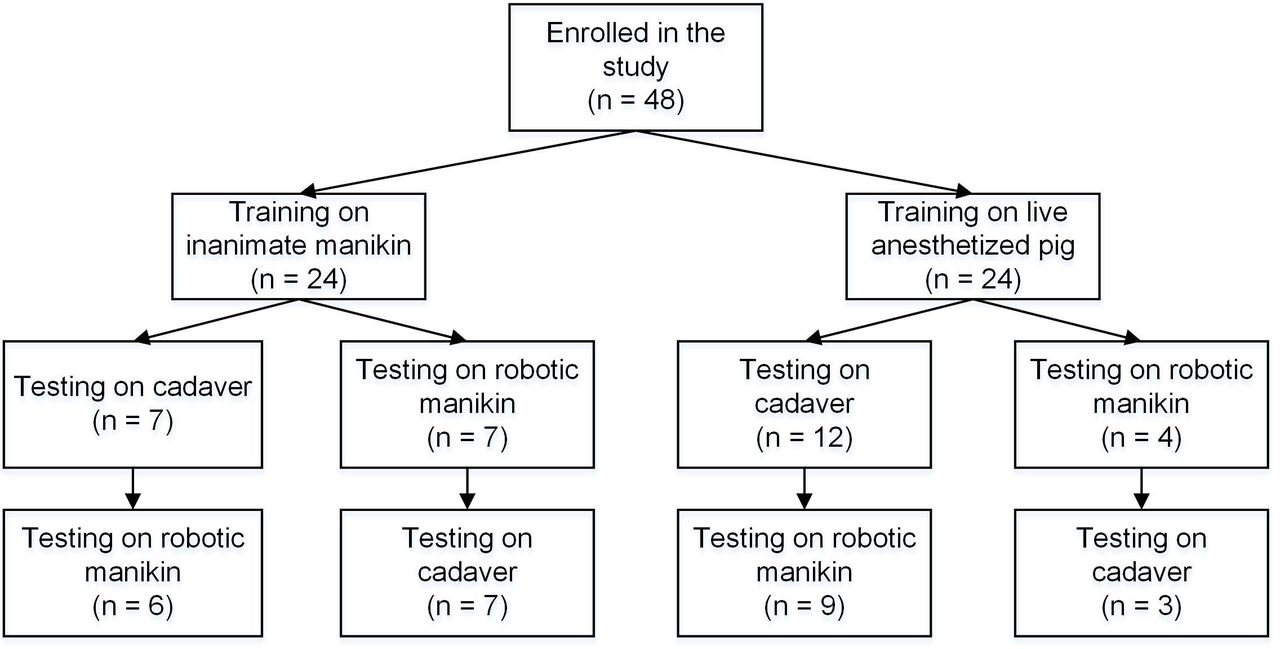
Training and testing of participants.
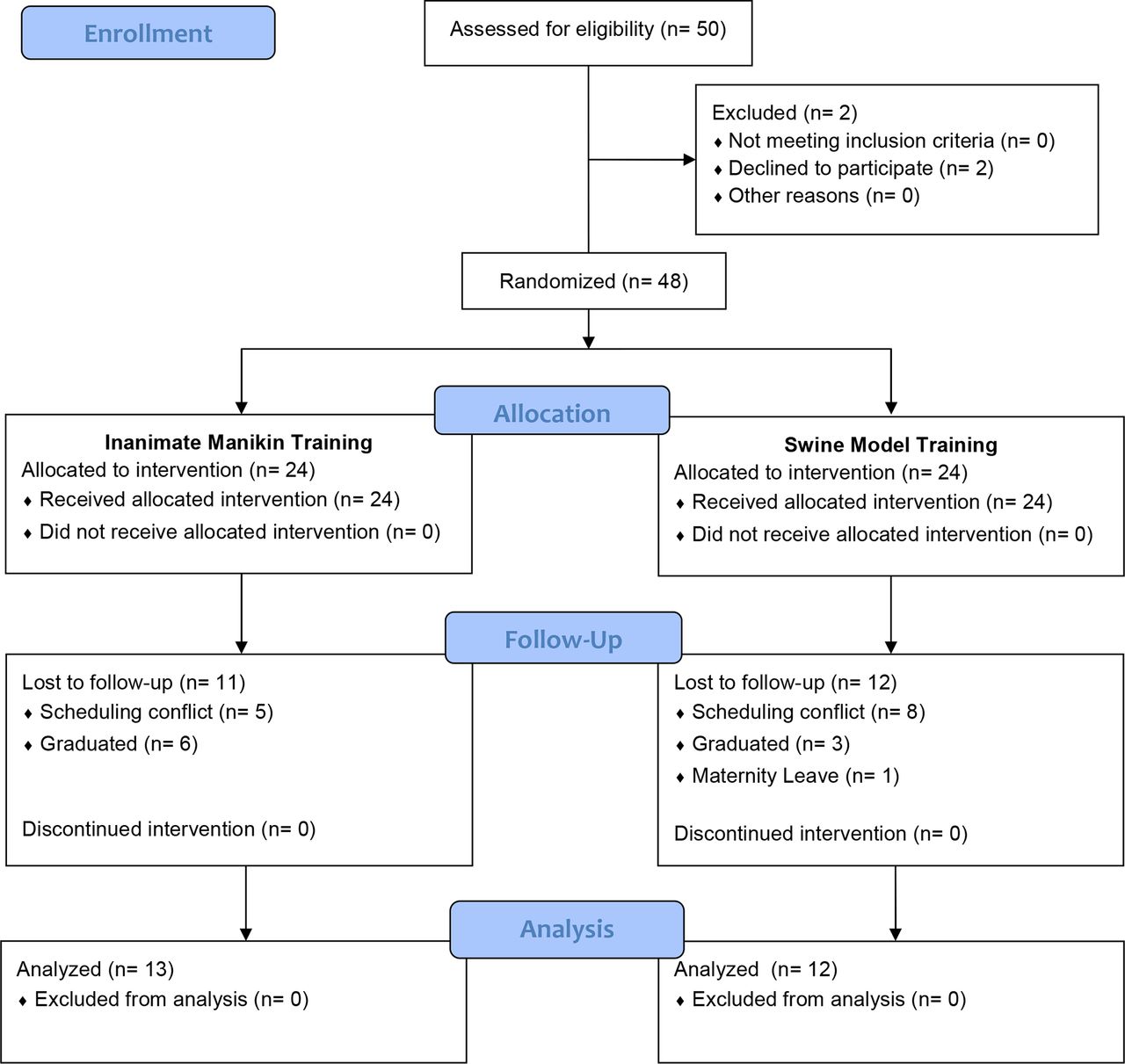
CONSORT study flow diagram.
Baseline participant characteristics
The mean age of the 48 participants was 26±3 years and 52% of them were women. Most of the participants anticipated pursuing general surgery (31%) or medicine (23%), while the remaining were interested in specialty surgery such as plastic surgery (15%) or otolaryngology head and neck surgery (8%), or emergency medicine (8%). About 15% of the participants had not decided on which specialty to pursue at the time of this study. There were no significant differences in participant characteristics between those who were trained on the live anesthetized pigs and those on the inanimate manikin (table 1).
Participant characteristics
Self-assessed confidence level
The mean baseline self-assessed confidence scores ranged between 1.3 and 2.3. For every item on the self-assessed confidence instrument, the scores improved from the baseline indicating an increase in confidence in performing a surgical cricothyroidotomy after the training. Percent increase in self-assessed confidence scores for each item and the type of training is provided in table 2. There was no significant difference in the change in self-assessed confidence scores from before to after training using swine model and inanimate manikin.
Change in self-assessed confidence scores before and after training
Technical skills level
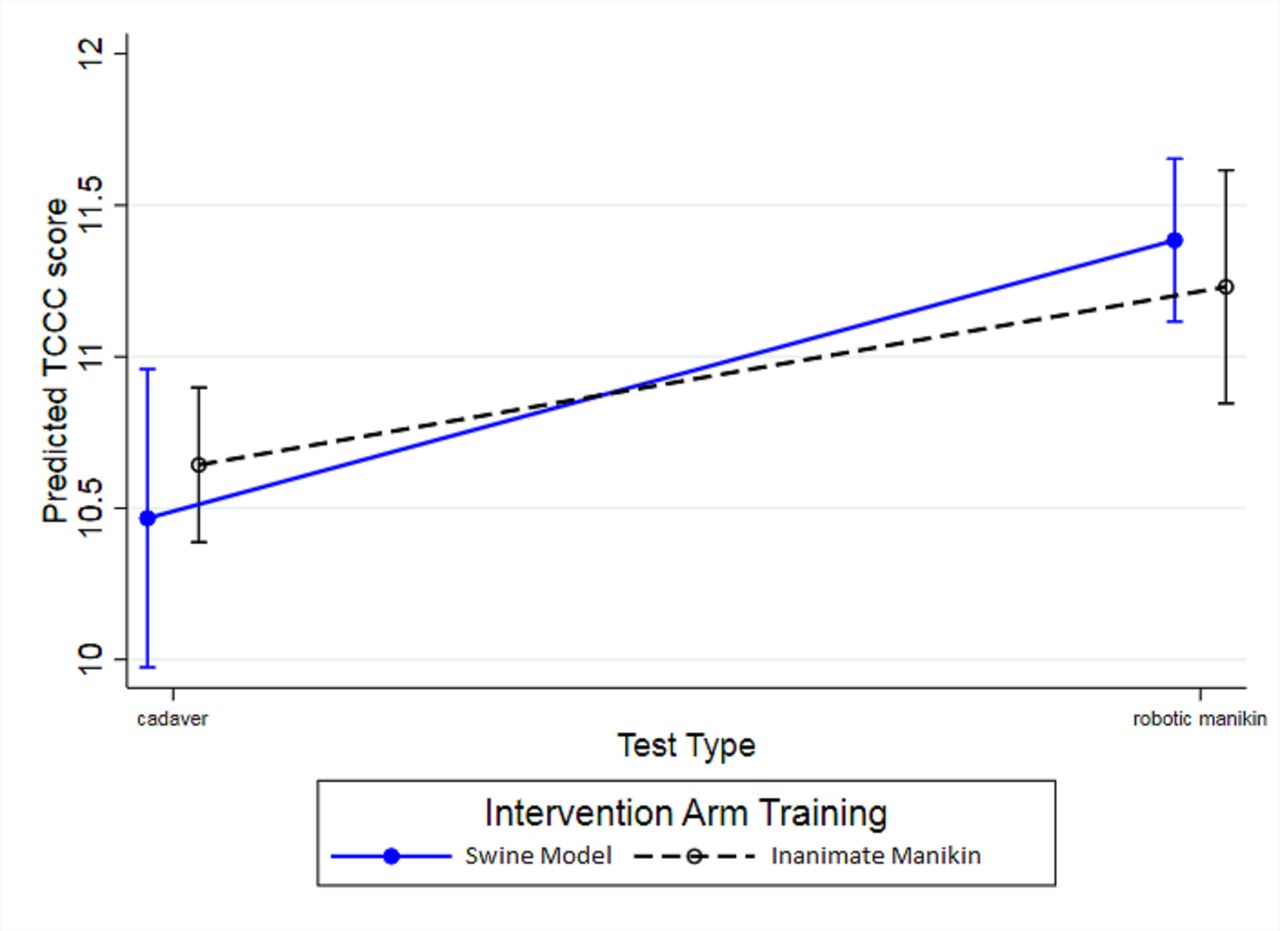
Generalized linear models with a log link analysis revealed that the OSATS scores were not significantly different by training (swine model vs manikin), type of testing (manikin vs human cadaver) or the order of testing (online supplementary table S3). Generalized linear models with a log link analysis of TCCC scores revealed that the test scores of participants who tested using the robotic manikin was significantly higher on an average by 7 points compared with the test scores using human cadaver (figure 3). However, the TCCC scores did not significantly vary by training or the order of testing (online supplementary table S4).
Supplemental material
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Graphic display of predicted TCCC scores comparing between those trained on swine model versus inanimate manikin. TCCC, Tactical Combat Casualty Care.
Placement and securement
The majority of the participants stated that they would primarily assess for chest rising (83%) or auscultate (70%) for breath sounds to confirm that the tube was correctly placed in the airway. Only 23% of participants stated that they would feel for air movement with their hand placed in front of the cricothyroidotomy tube and 17% stated that they would assess the oxygen saturation to confirm that the tube was correctly placed in the airway. While the validity of the didactic teaching module may not be perfect, the findings were similar in both groups. Most of the participants (97%) were able to describe how they would secure the cricothyroidotomy tube. There was no significant difference in the responses regarding the confirmation of tube placement or securement of airway between those who were trained using swine versus inanimate manikin models (table 3).
Comparison of cricothyroidotomy competency scores between swine model trained and inanimate manikin trained during first testing
Procedural duration
The average time taken for the participants to establish an airway from the time the instructor said ‘time starts now’ until cuff was blown up was 155±82 s (median=124.5 s), and the average time taken from the time the incision was made until the cuff was blown up was 95±52 s (median=75.5 s). The mean difference of 60 s is attributed to the time it took for the participants to collect and set up the supplies for the cricothyroidotomy. There was no significant difference in the time taken between those who were trained using the swine model versus the inanimate manikin (table 3).
Success of the procedure
All participants who were trained using the inanimate manikin were able to successfully obtain a patent airway after performing a surgical cricothyroidotomy. There were two participants in the swine model group who placed the cricothyroidotomy tube above the thyroid cartilage and one participant in the same group who placed the cricothyroidotomy tube in a false track anterior to the trachea.
Discussion
We evaluated novice medical students who were trained on swine and inanimate manikin models and found no major differences in their performance of cricothyroidotomy. Mean duration of cricothyroidotomy procedure was almost identical between two groups, and the rate of successful cricothyroidotomy was not statistically different. Blinded raters applied two different validated tools, the OSATS and TCCC rubric, to assess the performance of the cricothyroidotomy and could detect no significant difference between those trained on the swine model and those trained on the inanimate manikin. Given the consistency of these findings, the authors feel that it is unlikely that either training method is substantially superior to the other.
The only consistent change over the course of the study was the participants’ self-reported comfort with cricothyroidotomy and airway management. All participants, irrespective of which training method they were allocated to, what order they were tested in or what specialty they were interested in, were unanimous in stating their increased subjective feeling of comfort with emergency surgical airway management. One interesting finding was that the assessment scores using the TCCC rubric for all participants, again irrespective of training method, were universally higher when performing on the animated manikin than when performed on the human cadaver. TCCC is a course and a rubric designed to train and teach real combat scenarios and, perhaps, sterile and inanimate cadaveric specimens are less well suited to assess the kind of real world oriented, hands-on training and assessment offered through TCCC.
Unsuccessful surgical cricothyroidotomy in both the civilian and combat environment can be attributed to a number of factors including lack of familiarity with the procedure, inadequate teaching of the underlying anatomy, limited hands-on training with human anatomical landmarks, inadequate human training simulation models and a low refresher training frequency.15 Elliott et al 16 state that one of the main reasons for cricothyroidotomy failure is the lack of clinical experience, and therefore regular refresher training is required for skill maintenance. Walls17 relates two major problems when performing an emergent cricothyroidotomy that affect success rates: (1) the stress of the operator owing to the life-threatening nature of the situation; and (2) anatomical distortions caused by injury. The combat first responder may also find that correct identification of the landmarks needed to perform a successful cricothyroidotomy can be exceedingly difficult in austere environments owing to limitations of sensory perception, poor lighting, lack of equipment and added environmental stressors.11 As such, a solid knowledge of anatomy is imperative to lessen complications and is a key component in reducing anxiety among providers.15 18
Many if not all of the challenges stated above could be ameliorated by higher quality, more frequent cricothyroidotomy training with validated teaching methodology. The results of this study point future surgical airway educators in an important and perhaps different direction than has been taken in the past. The past and current ‘gold standard’ of training on an animal or cadaveric model is problematic. First, the animal used as the ‘gold standard’ is not, in fact, standardized as both goats and pigs are used. While live animals and cadavers have the benefit of having realistic tissue and dissection planes, an anesthetized, non-wounded, non-moving animal, with non-human anatomy, in a well-lighted vivarium, does not truly allow first responders to ‘train as they fight.’ Conversely, some medics are currently trained using non ‘gold standard’ models due to scarcity of animal or cadaveric models. These commercially available, synthetic models have the benefit of being anatomically correct but lack the tissue fidelity of the emotional realism of human cadavers or anesthetized animals.10 In the present study, the use of a dynamic, moving, bleeding, anatomically accurate human simulator overcomes the limitations of both previous training methods. Our study reveals that the TCCC scores among all participants were better when tested on a high-fidelity robotic manikin, as opposed to a cadaver, irrespective of the participants’ training method. The consistently observed higher scores on the high-fidelity manikin suggest it is a useful and feasible tool for both training and assessment.
Finally, given the concerns over animal rights of using animal models, the use of an advanced simulator has the potential to replace tissue models for surgical cricothyroidotomy training.19–21 While the initial capital investment for a high-quality human patient simulator is substantial, the long-term durability, portability and reusability likely make it a financially attractive option when compared with all the attendant care and ancillary services needed for animal training models.
Limitations
The key limitations of this study was the attrition rate, which was high due to scheduling challenges and availability of cadavers. It is important to note that while all medical students in this study were sensitive to scheduling challenges and away rotations, there was no systematic bias in terms of which students were available during periods when cadavers came available for testing. Essentially, it was random chance that permitted some students to complete the assessment while other did not, and in the authors’ view, this reduces the risk of any systematic bias unique to those who were lost to follow-up. The findings from this study are generalizable to most novice learners such as medical students but could also be extrapolated to other first responders such as paramedics, advanced practice providers and military personnel. First and second year medical students are truly undifferentiated with some anatomic and physiologic knowledge but little to no hands on experience with medical procedures and, as such, are a highly externally valid group to serve as procedural novices. Finally, data were not collected on the long-term skill retention to assess the sustenance and durability of the knowledge.
Conclusion
This is the first study to conduct a randomized controlled trial comparing the effectiveness of swine models to advanced simulation manikins in the training of first responders in cricothyroidotomy procedure. The similarities in the outcome measures between the two training approaches suggests that preferential use of high fidelity manikins for emergency surgical airway training may reduce both costs and ethical harm to animals. It may be time to establish a new ‘gold standard’ teaching methodology for emergency surgical airway procedures.
References
Footnotes
VP and WRL are joint first authors.
Contributors VP, WL, MB and ERH provided substantial contributions to the conception or design of the work; VP, KP and WL were involved or the acquisition of the data; VP, WL, CJ and GY were involved in the analysis and interpretation of data for the work; VP drafted the work; and WL, CJ, KP, GY, MB and ERH revised it critically for important intellectual content. All authors provided final approval of the version to be published and are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This work was funded by the Henry M. Jackson Foundation, Uniformed Services University of the Health Sciences (HU0001-14-0038, Subward 2884).
Competing interests VP has received two research grants from National Institutes of Health. The first grant is through the Nursing Institute of Nursing Research to assess symptoms and screen for laryngeal injury postextubation in intensive care unit settings (R01NR017433-01A1). The second grant is funded through the National Institute of Aging to evaluate the effectiveness of a novel arm restraint for intubated patients with cognitive impairment to reduce agitation, sedation and immobility (R42AG059451). ERH is/was primary investigator of contracts from PCORI entitled 'Preventing Venous Thromboembolism: Empowering Patients and Enabling Patient-Centered Care via Health Information Technology' (CE-12-11-4489) and 'Preventing Venous Thromboembolism (VTE): Engaging Patients to Reduce Preventable Harm from Missed/Refused Doses of VTE Prophylaxis' (DI-1603-34596). ERH is primary investigator of a grant from the Agency for Healthcare Research and Quality (1R01HS024547) entitled 'Individualized Performance Feedback on Venous Thromboembolism Prevention Practice' and is a coinvestigator on a grant from the National Institute of Health/National Heart, Lung, and Blood Institute (R21HL129028) entitled 'Analysis of the Impact of Missed Doses of Venous Thromboembolism Prophylaxis'. ERH is supported by a contract from The Patient-Centered Outcomes Research Institute (PCORI), 'A Randomized Pragmatic Trial Comparing the Complications and Safety of Blood Clot Prevention Medicines Used in Orthopedic Trauma Patients' (PCS-1511-32745). ERH receives royalties from Lippincott, Williams, Wilkins for a book 'Avoiding Common ICU Errors'. ERH was the paid author of a paper commissioned by the National Academies of Medicine titled 'Military Trauma Care’s Learning Health System: The Importance of Data Driven Decision Making', which was used to support the report titled 'A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury'.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.