Article Text

Abstract
Background As the number of patients surviving traumatic injuries has grown, understanding the factors that shape the recovery process has become increasingly important. However, the psychosocial factors affecting recovery from trauma have received limited attention. We conducted an exploratory qualitative study to better understand how patients view recovery after traumatic injury.
Methods This qualitative, descriptive study was conducted at a Level One university trauma center. Participants 1–3 years postinjury were purposefully sampled to include common blunt-force mechanisms of injuries and a range of ages, socioeconomic backgrounds and injury severities. Semi-structured interviews explored participants’ perceptions of self and the recovery process after traumatic injury. Interviews were transcribed verbatim; the data were inductively coded and thematically analyzed.
Results We conducted 15 interviews, 13 of which were with male participants (87%); average hospital length of stay was 8.9 days and mean injury severity score was 18.3. An essential aspect of the patient experience centered around the recovery of both the body and the ‘self’, a composite of one’s roles, values, identities and beliefs. The process of regaining a sound sense of self was essential to achieving favorable subjective outcomes. Participants expressed varying levels of engagement in their recovery process, with those on the high end of the engagement spectrum tending to speak more positively about their outcomes. Participants described their own subjective interpretations of their recovery as most important, which was primarily influenced by their engagement in the recovery process and ability to recover their sense of self.
Discussion Patients who are able to maintain or regain a cohesive sense of self after injury and who are highly engaged in the recovery process have more positive assessments of their outcomes. Our findings offer a novel framework for healthcare providers and researchers to use as they approach the issue of recovery after injury with patients.
Level of evidence III—descriptive, exploratory study.
- trauma
- injury
- recovery
- psychosocial factors
- qualitative study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Trauma is a common reason for hospitalization. It is estimated that over 12% of the US population will suffer a traumatic injury at some point in their life,1 and globally, an estimated 4.8 million deaths were due to injury in 2013. The number of people who survive trauma is estimated to be in the tens of millions per year.2
Most modern trauma systems are structured around five essential phases of care: injury prevention, prehospital emergency stabilization and transport, acute hospitalization, rehabilitation, and reintegration with society. Although the US trauma system has achieved great success in improving outcomes related to the first four phases of care, especially in reducing mortality in patients who sustain serious injuries,3 as the rates of preventable mortality have fallen, further improvements in preventable deaths are likely to be small.4 The final phases of rehabilitation and societal reintegration encompass the vital period of recovery that patients must navigate, often on their own and with little guidance from healthcare practitioners. While variability in patient outcomes after injury is shaped by well-studied factors like injury severity and resulting objective functional status, it is also greatly influenced by psychosocial factors.5 Surprisingly little research has been conducted on these final phases of recovery once contact with healthcare providers becomes less frequent, although this is changing.6 7
The goal of this qualitative, hypothesis-generating study was to explore what successful recovery from injury looks like through the eyes of the patient. It builds on prior work using qualitative methods to understand the psychological process and its impact on recovery from injury.5 8–11 Importantly, these works have lent support to the notion that illness and injury are not only physical phenomena but also forces of biographical disruption.12 13 In this view, illness and injury take on meaning not just through their direct consequences on physical function but also through their significance to patients’ life narratives. Here, we extend this work to our understanding of patient’s experience and perceptions of the recovery process following severe traumatic injury.
Data and methods
We conducted a qualitative study to explore the physical, psychological and social factors that motivate and shape how patients approach recovery after injury. We identified patients admitted to Level One university trauma center by retrospectively reviewing the center’s trauma registry. Maximum variation purposeful sampling was used to identify male and female patients 1–3 years postinjury and to include a range of ages, socioeconomic backgrounds, injury mechanisms and injury severities.14 Patients with common blunt-force mechanisms of injuries were recruited to ensure a representative sample across trauma experiences; these included motor vehicle/motorcycle crash, automobile versus pedestrian, bicycle crash, fall from height and ground-level fall. Additionally, we considered traumatic brain injury (TBI), spinal cord injury (SCI), rib fractures and polytrauma (defined as greater than one major bodily insult) to represent common injuries in the USA. We aimed to recruit a minimum of 15 participants as justified in qualitative methodology literature in order to reach thematic saturation—an expected point when no new ideas or themes emerge from analysis with inclusion of additional participants, identified either during the interview or analysis processes.8 15 Patients with burns or who sustained injuries through interpersonal violence were excluded, as the psychological context of such experiences was expected to be distinct from non-violence-related injuries.
Eligible participants were randomly contacted via telephone and asked to volunteer for a in-person or telephone audiorecorded interview until we had agreement from 15 patients. Patients with TBI were deemed to have sufficient cognitive function to consent if they had a Glasgow Coma Score of 15 at the time of consent.
A semi-structured interview guide was developed with input from experts with diverse professional backgrounds including trauma surgeons, emergency surgery advanced practice providers, critical care specialists, social and health psychologists and case managers. Open-ended questions were designed to lead participants through a brief discussion of their preinjury life before specifically discussing their experience with the recovery process (online supplementary appendix: Qualitative Interview Guide). Questions were designed to help guide the conversation toward key events and experiences in the time period after the injury in a neutral manner. Interviews were conducted by two of the authors, a surgical resident and a psychology doctoral student (GR, SZ), both of whom were trained in interview techniques and qualitative methods. All data were transcribed verbatim by a professional service and screened for accuracy. The transcriptions were imported into NVIVO V.11 (QRS International, Victoria, Australia) for storage, coding and analysis.
Supplemental material
Study personnel (GR, SZ, ES, NA) conducted a team-based analysis of all data and included a surgical resident, a psychology doctoral student, and two medical students familiar with the study aims. First, study personnel independently reviewed the transcripts for initial codes using a general inductive approach through a detailed reading of the data.16 Next, the team agreed on an interim coding scheme with clear definitions; codes and their definitions were iteratively refined through consensus-building using discussion and arbitration of discrepancies resulting in the final codebook. An inter-rater reliability test was conducted between the two coders (GR, SZ) to ensure consistent application of the final codes to the same units of text, with a minimum expectation of pooled Cohen’s kappa of 0.7.17 Once inter-rater reliability was ensured, all transcripts were then coded by the two coders (GR, SZ). After coding was complete, the full research team, including a qualitative expert (SBM) and content expert (TGW), consolidated emerging concepts into core themes over a series of discussions, which were then integrated into a conceptual model of patient recovery.
Participants were provided with study details verbally and in writing. Participants consented to participation in the study and audio-recording/transcription. We followed Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.
Results
Eighty-one potential participants meeting eligibility criteria were identified using the trauma registry. We sequentially enrolled patients until we reached our target sample of 15 patients representing the archetypal patient across the spectrum of age, socioeconomic and educational background. At the time of interview, individuals were on average 22 months (range=14–36 months) postdischarge from the hospital. Three participants (20%) were interviewed by phone and 12 participants were interviewed in person. Interviews lasted an average of 36 min (range=20–68 min).
The average age of participants was 47.7 (±SD, range 20–84) years and 13 (87%) were male. All were injured by blunt mechanism with seven (47%) requiring operative intervention during the index hospitalization for trauma. Thirteen participants (87%) spent at least one midnight in the intensive care unit and the average hospital length of stay was 8.9 days (range: 2–26 days). The mean injury severity score was 18.3 (range: 5–30). Participants had endured a range of injuries that matched common injury mechanisms and patterns (table 1). Three key insights emerged through qualitative analysis of the interviews.
Individual patient demographics and injury characteristics at time of interview
Comprehensive recovery of the body and the self
The first key insight was that participants generally considered recovery to involve two key components: recovery of the body and recovery of the self—a composite of one’s roles, values, identities and beliefs. Recovery of the body included the functional outcomes commonly targeted by physical therapy and rehabilitation: the recovery of form, function, and ability. However, participants noted that recovery of the body was not the sole contributor to healing. Recovery of the self was found to be an important component of rehabilitation. Therefore, a successful recovery of the self meant that participants had a coherent sense of these four components and could answer the questions: “Who am I? How do I fit in this world?”
Injury threatened one’s self-concept, and the consequences of an injury might be incongruent with an individual’s understanding of themselves or their assumptions of how the world should operate. For example, an individual’s form, function, and abilities could be a deeply integrated part of their identity and how they understood themselves (ie, through work, hobbies and social roles). Therefore, when an injury affected one’s ability to perform at work or carry out roles, it could pose a threat to one’s self-concept (table 2; quote 1).
Representative quotes about the comprehensive recovery of the body and the self, level of engagement in the recovery process and subjective assessments of recovery outcomes
For some participants, the injury itself and the subsequent recovery process were at odds with their understanding of the world (ie, bad things do not happen to good people). When the randomness of the experience or perceived injustice of the consequences were incongruent with their beliefs about how the world should operate, participants’ self-concept was called into question (table 2; quote 2).
Some participants expressed not feeling like themselves and spoke about how this unsettling experience presented challenges throughout the recovery process. Those who lacked a sound sense of self described struggling with achieving a positive subjective outcome assessment (table 2; quote 3).
Level of engagement
The second key insight was that while engagement in the recovery process appeared to be important, it was not universal, and fell on a spectrum. For this study, we operationalized ‘engagement’ in terms of its behavioral and psychological characteristics. Behavioral components included effort, participation and persistence, while psychological components included emotional regulation, problem-solving and approaching rather than avoiding challenges.
Discussions of engagement often emerged as participants reflected on key transitions in the recovery process, such as the transition from more structured care environments (ie, an inpatient facility) to less structured environments (ie, home or an outpatient program). No longer able to rely on institutional support systems to guide their recovery process, many patients found that the responsibility for recovery had passed to them and their own support systems. Our analyses suggested that individuals varied in the degree to which they assumed responsibility for their recovery and took an active and engaged role in this process.
Participants who were highly engaged repeatedly described instances in which they approached recovery in an active, purposeful way. These participants expressed an overall belief that persistent attention to goals and effortful pursuit of them—even in the face of challenges—were necessary components of the recovery process (table 2; quote 4). They often took ownership of their injury and recovery process and engaged in a motivated pursuit of specific recovery-relevant goals (table 2; quote 5).
Not all participants engaged in the recovery process to this degree. While less engaged participants were likely to have some brief, sporadic moments in which they were highly engaged, they did not often independently set out and pursue recovery-relevant goals in the same effortful manner. They demonstrated less ownership of their injury and recovery process, often describing an over-reliance on others’ directions. These individuals struggled to describe a clear approach or strategy to navigate the recovery process and appeared not to possess a mental model for how to comprehend their injury or how to approach recovery. Consequently, they often avoided taking critical actions necessary to facilitate successful recovery. When describing their injury, less engaged participants expressed how unjust or unfair it seemed, and often endorsed feeling like ‘victims of their injuries’. In focusing on these aspects of the injury and recovery, many languished without a clear path forward (table 2; quote 6).
Subjective assessment of recovery outcomes
The third key insight was that each participant had his or her own unique conceptualization of recovery, or ‘subjective outcome assessment’, as it was primarily based on their own personal assessment of their current state of health and well-being within the context of their broader lives. This assessment was influenced by both engagement and recovery of the self: participants who were highly engaged in the recovery process and described recovery of both the body and the self overwhelmingly reported more positive assessments of their outcomes. Highly engaged individuals tended to speak positively about their recovery, even if they faced ongoing challenges or permanent limitations. The act of engaging in the process of recovery appeared to contribute to a positive appraisal of their outcomes. In fact, some highly engaged participants had a very positive assessment of their outcomes despite persistent or permanent disabilities. The reason for a positive subjective outcome assessment despite incomplete recovery of the body appeared to relate to the recovery of the self.
Furthermore, recovery of a coherent sense of self was critical to a positive subjective outcome assessment. Participants frequently remarked positively about expectations for their recovery despite ongoing challenges, which contributed to one’s subjective outcome assessment (table 2; quotes 7 and 8). Participants were able to weave their current health status into their experience of the injury and their lives as a whole. Many expressed an overall appreciation for life, which greatly contributed to their subjective outcome assessment of their recovery (table 2; quote 9). Regardless of objective functional status, individuals whose sense of self was threatened by injury struggled to have a positive subjective outcome assessment of their recovery (table 2; quote 3).
Conceptual model for recovery
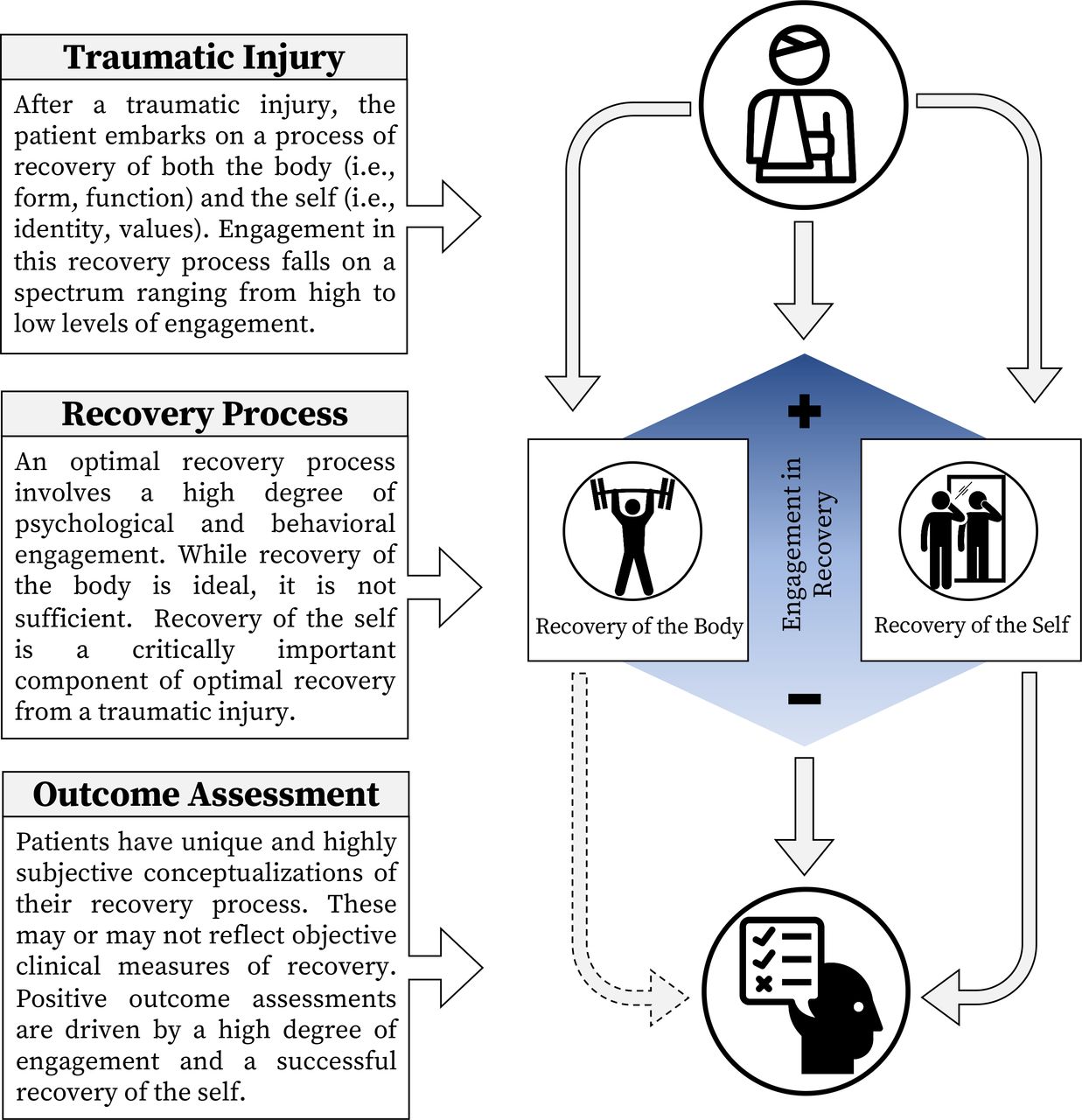
The impact injury and the subsequent recovery process have on the patient is highly variable and not entirely dependent on injury severity or resulting objective functional status. While some patients skillfully navigate the immediate injury and become highly engaged in the recovery process, others languish without a clear strategy for managing this critical time period. We observed that participants who were highly engaged in their recovery process tended to have a more positive assessment of their outcome regardless of their residual disability. Similarly, patients differed in both physical and psychological recovery from injury. While the physical recovery of the body’s form, functions, and abilities was important, we found that the recovery of a coherent sense of self was critically important for forming a positive assessment of one’s recovery and health outcomes.
This subjective assessment of one’s own status of recovery was critically important to nearly every participant interviewed in this study. It appeared to be influenced by the degree of engagement in the recovery process as well as the recovery of a coherent sense of self after injury. From these three key insights, we created a framework for a novel conceptual model of the post-injury recovery process (figure 1) that informed recovery.

Conceptual model of recovery after a traumatic injury.
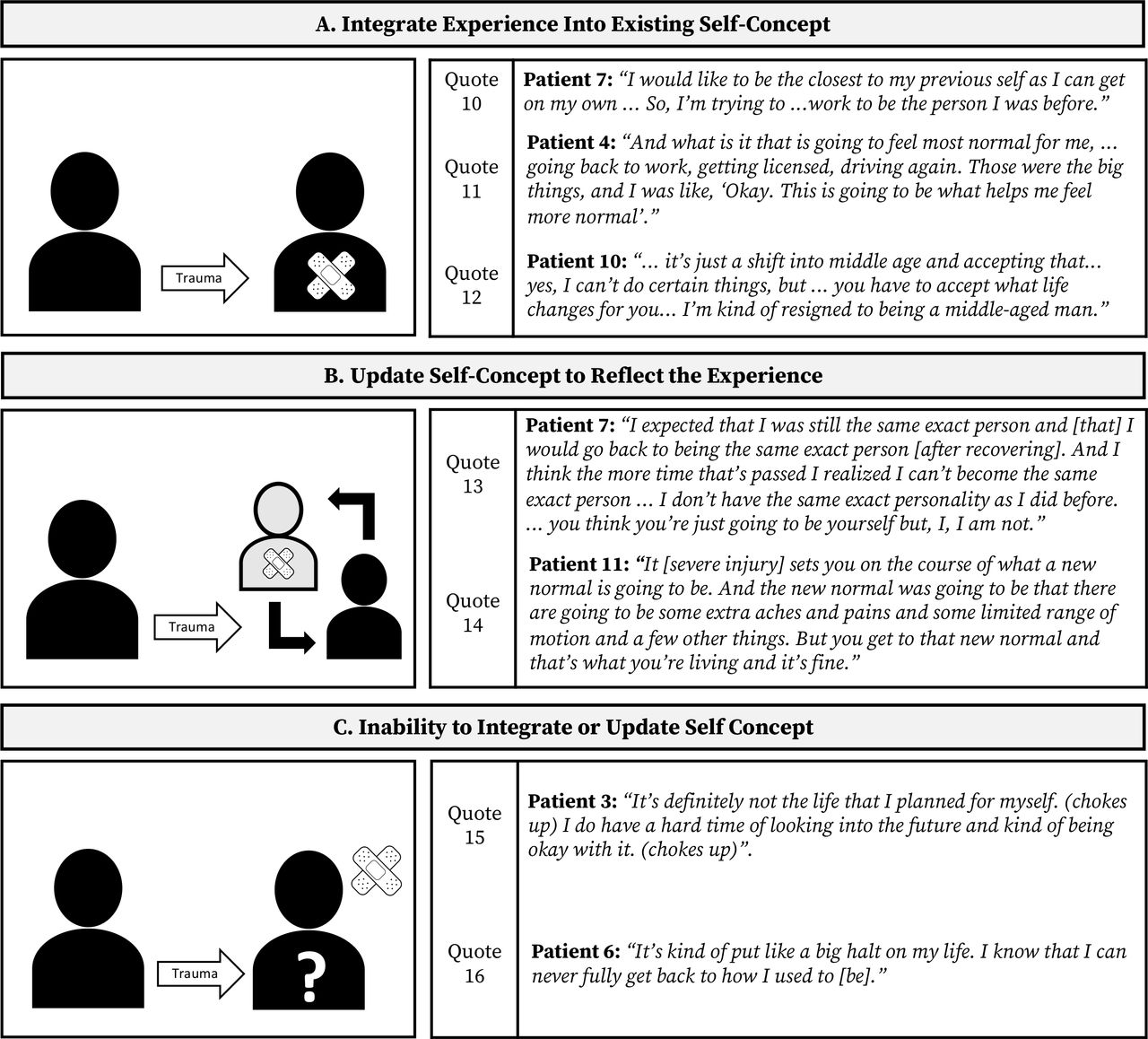
Overall, we found three potential pathways through which our participants attempted to understand themselves after injury: participants able to integrate their traumatic experience into their self-concept; participants creating a new sense of self to reflect their injury; and participants who were unable to update their sense of self (figure 2). In the first pathway, participants successfully integrated their experience into their self-concept. Although their injury shaped how they thought about themselves and their place in the world, they were able to integrate the experiences into their self-concept, generally retaining their sense of self-coherence and identity. Many participants expressed that actions and milestones helped in this process (figure 2; quotes 10 and 11). This pathway was common for many middle-aged participants, who expressed difficulties grappling with concerns surrounding aging and mortality, which may have previously gone overlooked. These participants were tasked with integrating a newfound awareness of age and disability into their postinjury self-concept (figure 2; quote 12).

{kind=link}
{kind=link}
Three pathways toward recovery of the self after a traumatic injury and representative quotes from participants. Panel A: maintain existing self-concept and integrate traumatic injury. Panel B: create a new self-concept that reflects the traumatic injury. Panel C: inability to integrate or update self-concept.
In the second pathway, participants crafted a new sense of self to reflect their injury. For these individuals, the consequences of their injuries affected their roles, values, identity and/or beliefs in ways that made it difficult or impossible to reclaim their previous sense of self, yet appeared successful in transcending their injuries in pursuit of finding a new and coherent sense of self. They acknowledged that recovery is a long-term, possibly lifelong process by taking ownership over their recovery and accepting ‘a new normal’ (figure 2; quotes 13 and 14).
In the third pathway, participants’ injury experience threatened their self-concepts in a more fundamental way, profoundly affecting their understanding of who they are and how they fit in the world. These individuals described a relentless search for a life congruent with their previous roles, values, identity, and beliefs. These individuals neither successfully updated their self-concept to reflect their injury and subsequent limitations, nor incorporated their injury into their previous self-concept. Many described a constant search for new things that resonate with their sense of self, but had been unable to change how they see themselves in their world (figure 2; quote 15). Others expressed a feeling of being stuck, that their life would be permanently different from how they previously saw it. These individuals did not describe searching for a new sense of themselves as a way to move on after their injury (figure 2; quote 16).
Participants in the first two pathways found ways to recover their sense of self by either integrating their experiences into their sense of self or creating a new sense of self. However, participants in the third pathway were unable to update their sense of self, which appeared to have important consequences for how they came to assess their recovery outcomes.
Discussion
Using rich narratives from interviews with archetypal trauma patients, an in-depth analysis of the period of recovery following injury revealed three important insights: that recovering from injury is multifaceted, involving both physical recovery of the body and psychological recovery of the self; that one’s level of engagement is central to recovery outcomes; and that the patient’s subjective assessment of their recovery outcomes is most important to them and is influenced by both level of engagement and achievement of a coherent sense of self. These elements were synthesized into a novel conceptual model for recovery after injury.
These findings highlight the importance of maintaining a coherent sense of self after injury. Self-coherence, or the need to be rooted and stable in one’s sense of self, has also been described as a core psychological need impacting motivational processes and goal pursuit.18 While this notion has been previously explored in the medical context,12 13 19 it has not been widely integrated into traumatic injury recovery and care.
Our analysis adds to the idea that injury can threaten one’s sense of self and provides further insight by observing that a coherent sense of self is integral to an individual’s positive subjective assessment of the recovery outcomes. We also noted the centrality of active engagement in the recovery process. The importance of engagement has been previously explored in other settings: patients who engage in the management of their healthcare show improvements across a number of objective behavioral and physiological health outcomes.20–22 Fostering engagement early on in the recovery process may have a similar impact on patients after injury and influence a patient’s subjective assessment of recovery, which is of particular importance to patients. As patients transition out of hospital, trauma teams should focus on promoting patient engagement. Rehabilitation specialists and primary care providers should continue to encourage high levels of engagement in the process of recovery as they council patients.
Our findings also illuminate the importance of an individual’s subjective outcome assessment and the fact that this appears to be largely influenced by engagement in recovery. We believe a subjective outcome assessment gives individuals space to have positive or negative opinions of their recovery in the face of continued disability or apparent full functional recovery. Critically, participants who were highly engaged in their recovery and who maintained a coherent sense of self expressed a positive appraisal of their recovery—often in spite of physical setbacks. This finding further illustrates the importance of both patient engagement and a comprehensive recovery of both the body and the self.
Future directions
This study was exploratory and hypothesis-generating. While we identified key insights into recovery after injury and integrated those insights into a conceptual model for recovery, focus must be directed at assessing the generalizability in a larger cohort. Further investigation is required to determine if addressing and promoting recovery of the self will improve overall self-reported outcomes. Because the aim of this study was to illustrate the experience of recovery from the perspective of the patient, we acknowledge there are many factors important to successful recovery that we did not explore, and that some of these factors can impair the ability of individual patients to take ownership of their recovery process. Future work should not neglect these factors, but rather incorporate our findings that sense of self contributes to subjective assessments within the constrains of any given situation when evaluating recovery from injury. Further investigations should also explore factors that predict differences in the recovery of the self factors that may nurture and maintain engagement in the recovery process. It should involve the use of mixed-methodology with quantitative patient-reported outcomes and objective functional measurement tools coupled with qualitative psychosocial assessments. Important work is already underway by other investigators using quantitative measures such as the Functional Outcomes and Recovery After Trauma Emergencies (FORTE) project6 23 and mixed methods approaches such as by Gabbe et al.7 11
Limitations
Participants volunteered for the interviews, indicating a certain level of engagement in the recovery process with selection bias toward potentially more engaged individuals. The viewpoints of those with lower levels of engagement in the process of recovery may not be fully represented in this sample, blunting our ability to observe the effect of engagement on outcome. Despite this, we were able to observe a spectrum of engagement among the participants in this study.
In addition, our study did not include victims of violent trauma; it is likely that recovery associated with violence is more complex than represented by our findings. Additionally, our sample included individuals 1–3 years following hospital discharge. As such, we are lacking long-term experiences with the process of recovery that could add additional insight to our conceptual model for recover. However, short-term to mid-term experiences are represented regarding essential elements for the recovery process.
Our sample of 13 males and 2 females is consistent with male predominance in the trauma population at large, we acknowledge that the smaller representation of females in our study represents a sampling bias. Even though we actively sought to recruit female participants, few volunteered, suggesting that a focused recruitment strategy to more fully incorporate the female recovery experience may be necessary.
Finally, the qualitative nature of the methodology for this study involved ascribing personal interpretations to the narratives obtained through the interviews. Although there are many objective patient-reported outcomes tools,24 we did not assess objective functional outcomes of participants. While care was taken to let the participants’ words speak for themselves, alternative findings and insights could be reached by individuals with different perspectives or expertise. We intentionally built collaboration with experts in traumatology and health psychology to add breadth of perspective to our analyses.
Conclusions
In this qualitative, exploratory study, we found the importance of both the body and self as necessary components of recovery following traumatic injury. Our analyses identified three key insights and led us to construct a novel conceptual model of recovery that includes recovery of the body and the self that we believe can inform clinical practice. In illuminating the patient’s understanding and approach to recovery after injury, our hope is to equip healthcare providers with a new framework that can help them guide patients through the recovery process. Based on these findings, we recommend that practitioners caring for patients with traumatic injuries acknowledge that recovery involves both recovery of the body and recovery of the self and help patients re-establish a coherent sense of self after trauma. Similarly, we encourage practitioners to highlight the importance of engagement in the recovery process. These two recommendations may help guide patients toward a more positive assessment of their own recovery.
References
Footnotes
Contributors Study design and conception: GR, SZ, AC, TGW. Data collection: GR, SZ, ES, NA. Data analysis and organization: GR, SR, ES, SBM, NA. Data interpretation: GR, SZ, SBM, DS, AC, TGW. Drafting of manuscript: GR, SZ, ES. All authors have reviewed the manuscript and approved the findings.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study was approved by the Stanford University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deidentified data will be made available on reasonable request.