Article Text

Abstract
Background Aims of the study were to determine the effects of humerus intraosseous (HIO) versus intravenous (IV) administration of epinephrine in a hypovolemic, pediatric pig model. We compared concentration maximum (Cmax), time to maximum concentration (Tmax), mean concentration (MC) over time and return of spontaneous circulation (ROSC).
Methods Pediatric pig were randomly assigned to each group (HIO (n=7); IV (n=7); cardiopulmonary resuscitation (CPR)+defibrillation (defib) (n=7) and CPR-only group (n=5)). The pig were anesthetized; 35% of the blood volume was exsanguinated. pigs were in arrest for 2 min, and then CPR was performed for 2 min. Epinephrine 0.01 mg/kg was administered 4 min postarrest by either route. Samples were collected over 5 min. After sample collection, epinephrine was administered every 4 min or until ROSC. The Cmax and MC were analyzed using high-performance liquid chromatography. Defibrillation began at 3 min postarrest and administered every 2 min or until ROSC or endpoint at 20 min after initiation of CPR.
Results Analysis indicated that the Cmax was significantly higher in the IV versus HIO group (p=0.001). Tmax was shorter in the IV group but was not significantly different (p=0.789). The MC was significantly greater in the IV versus HIO groups at 90 and 120 s (p<0.05). The IV versus HIO had a significantly higher MC (p=0.001). χ2 indicated the IV group (5 out of 7) had significantly higher rate of ROSC than the HIO group (1 out of 7) (p=0.031). One subject in the CPR+defib and no subjects in the CPR-only groups achieved ROSC.
Discussion Based on the results of our study, the IV route is more effective than the HIO route.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Globally, 1 million children die from blunt and penetrating trauma, accounting for more deaths among children than all other causes combined. An additional 9 million require emergency care following traumatic injury.1–3 In the USA, trauma and hemorrhage are the leading causes of death in children.4 In these scenarios, the leading cause of death is trauma and hemorrhage with subsequent cardiac arrest.
In cases of trauma, hemorrhage and cardiac arrest, establishing rapid vascular access is essential for return of spontaneous circulation (ROSC).5 6 Injuries that cause hemorrhage lead to volume depletion and vascular collapse. Additionally, endogenous catecholamine release results in vasoconstriction. These factors make intravenous (IV) access extremely difficult, time consuming or impossible even for the most skilled clinician. Other factors impeding rapid vascular access include limited personnel, limited expertise, unavailability of ultrasound, poor lighting, and mass casualties.
In patients with cardiac arrest (CA), early administration of epinephrine is associated with a higher probability of ROSC.7 8 In a mature pig model of CA, early intraosseous (IO) administration of epinephrine improved rate of ROSC, and 24 hours survival.9 We have previously shown that humerus IO (HIO) epinephrine administration is equivalent to IV administration in an adult normovolemic model.10 11
Because children have smaller veins and proportionately more fat tissue than adults, establishing vascular access in children is very difficult particularly in a young child and is exacerbated in the presence of hypovolemia and CA. Several studies have investigated the pharmacokinetics and effects of tibial IO administration of epinephrine relative to IV administration in animal models of pediatric CA.12–14 However, no studies have investigated the pharmacokinetics of epinephrine administered IO and rate of ROSC in a pediatric hypovolemic model. Hypovolemia in the child may also affect the serum concentration, volume of distribution (VD), mean concentration (MC), peak or maximum concentration (Cmax) and time to maximum concentration (Tmax) of epinephrine, adversely affecting rates of ROSC. In the Pediatric Advanced Life Support (PALS)-Emergency Cardiovascular Care Guidelines, the American Heart Association (AHA) recommends administration of epinephrine (0.01 mg/kg of 1:10 000) by IO or IV route. With limited empirical data, these recommendations, however, are based on expert opinion.15–17 To date, no studies have investigated the pharmacokinetics of epinephrine administered IO and rate of ROSC in a pediatric hypovolemic CA model.
To address this gap in knowledge, we examined the following research questions in a hypovolemic, pediatric CA porcine model:
Are there significant differences in MC over 5 min, Cmax and Tmax of epinephrine when administered via HIO versus IV routes?
Are there significant differences in frequency of ROSC in HIO, IV, cardiopulmonary resuscitation (CPR)+defibrillation (defib) and CPR-only groups?
Methods
The study was a prospective, randomized, within and between, blinded-experimental design using a hypovolemic pediatric pig model. The pig were cared for according to the Animal Welfare Act and the Guide for the Use of Laboratory Animals.18
Sample
Twenty-six male Yorkshire-cross pig weighing between 20 and 30 kg were used to represent human subjects aged 9 years.19 20 We selected male pigs to control for any potential hormonal effects. Young, castrated male pig were purchased from a single vendor to reduce any variability. This range of pig was chosen because the average blood volume, weight, cardiovascular system and bone structure is comparable to that of human children. We performed a power analysis using G*Power 3.1 for Windows (Heinrich Heine University, Dusseldorf, Germany) to determine sample sizes for each group. Using a α of 0.05, a large effect size of 0.6 based on previous similar research,21–23 and a power of 0.8, we calculated that we needed a sample size of 7 in the IV, HIO and the control group, CPR+defib. The local Institutional Animal Care and Use Committee (IACUC) required the restriction of the number of animals in the CPR-only group to five to prevent unnecessary sacrificing of pig. The pigs were randomized using a computerized random number generator into four groups: CPR+defib with epinephrine via humeral intraosseous catheter (HIO) (n=7); CPR+defib with epinephrine via IV (n=7); CPR+defib only (n=7) and CPR only (n=5). The humerus is an approved site for the administration of both fluids and medications.24
The pig were transported to the vivarium and allowed 3 days to acclimate. They received daily medical screenings to monitor overall health. During this period, the pigs were fed an approved diet and allowed water ad libitum. The pig were restricted from food for 12 hours preceding the study.
Procedure
On the day of the study, the animals were first administered intramuscular injection of tiletamine (4–8 mg/kg) and then transferred to the surgical suite. Anesthesia was induced through inhaled isoflurane 2%–5% via face cone. The pig were then intubated with either a 6.5 or 7.0 endotracheal tube (ETT). Mechanical ventilation with a tidal volume (Vt) of 6–8 mL/kg at a respiratory rate of 10–14 per minute using a GE Datex-Ohmeda Aestiva anesthesia machine (Datex-Ohmeda, Madison, Wisconsin, USA) was initiated after confirmation of placement and securing the ETT. The isoflurane concentration was then decreased to 0.5%–2% for maintenance of anesthesia but was discontinued when the pigs were in CA. An arterial catheter was placed in the left carotid artery, using a cut-down approach, for continuous hemodynamic monitoring for all animals and used as a replacement of manual pulse checks to determine effectiveness of compressions and ROSC during resuscitation. The same procedure was used to place an arterial catheter in the right femoral artery for blood sampling and induction of hemorrhage. Vital signs were monitored using a Carescape monitor (GE Healthcare; Little Chalfont, Buckinghamshire, UK); vital signs included oxygen saturation (SpO2), 5-lead ECG, arterial blood pressure, rectal temperature and end-tidal carbon dioxide and isoflurane. Cardiac output (CO) and stroke volume (SV) were monitored using a Vigileo hemodynamics monitor (Edwards Lifesciences, Irvine, California, USA). An 18-gauge peripheral IV was placed in the auricular vein of all pigs for fluid replacement and medication administration. IV patency was maintained by infusing normal saline (NS) at a keep-vein-open rate. For the HIO group, a 15-gauge EZ-IO catheter (Teleflex, Philadelphia, Pennsylvania, USA) was placed in the upper aspect of the humerus, after performing a cut down to expose the bone. Proper placement was verified through aspiration of bone marrow and ease of a 10 mL flush of NS.
All pig were allowed to stabilize for 15 min before beginning the experiment. Subjects had 35% of their blood volume exsanguinated at a rate of 100 mL/min, representing a American College of Surgeons class III hemorrhage.25 This equated to approximately 24.5 mL/kg of blood exsanguinated for each subject. To measure the exsanguination, we used a tabletop scale (NewClassic MF, Mettler Toledo, Columbus, Ohio, USA) to weigh the blood that was drained by gravity from the femoral arterial catheter. Shed blood was collected in heparinized collection bags for later reinfusion.
After exsanguination, CA was induced by direct electrical stimulation of the subject’s heart.26 CA was defined as a non-perfusing rhythm (ventricular fibrillation, pulseless ventricular tachycardia, pulseless electrical activity and asystole) and non-pulsatile arterial line waveform without palpable pulse. On confirmation of CA, inhaled anesthesia, ventilation and oxygen delivery were discontinued. The subjects remained in arrest for 2 min, representing the time used in other studies to begin resuscitation efforts in witnessed CA.27 IV midazolam 0.05 mg/kg and buprenorphine 4 μg/kg were administered immediately before beginning CPR. Chest compressions at a rate of 100 per minute with a depth of 2–3 inches were administered by using the Michigan Automated Thumper (Michigan Instruments, Grand Rapids, Michigan, USA). This device ensured that reliable and replicable compressions were delivered throughout the experiment. Subjects were manually ventilated at a rate of 10–14 times per minute at 6–8 mL/kg Vt. Resuscitation efforts and defibrillations were administered according to PALS Cardiac Arrest and Hypovolemic Shock 2015 guidelines.
Two minutes after the initiation of CPR, epinephrine 0.01 mg/kg was administered by either IV or HIO route followed by 10 mL NS flush.27 Blood samples were collected before hemorrhage, and at 0.5, 1, 1.5, 2, 2.5, 3, 4 and 5 min after epinephrine administration, in order to measure Cmax and Tmax via high-performance liquid chromatography (HPLC). Before each sample collection, 10 mL of blood was discarded to prevent specimen contamination. To ensure patency of the arterial catheter, 10 mL NS was flushed between blood samples. Arterial blood gases were collected before exsanguination and every 5 min after arrest to ensure suitable treatment and normal pH levels and guide ventilation parameters. Biphasic defibrillation started at 3 min and was repeated every 2 min using Lifepak 20 defibrillator (Redmond, Washington, USA). Isotonic crystalloid fluid resuscitation was initiated (3 mL of fluid for every 1 mL of blood loss) for hypovolemic shock and medications were maintained according to PALS guidelines/recommendations throughout the rest of the experiment.28 At 15 min postarrest, the exsanguinated blood was infused back to the subject via IV at a high rate using pressure bags at 300 mm Hg. ROSC was defined as a sustained systolic blood pressure ≥60 mm Hg and a palpable pulse. Following ROSC, subjects were placed back on mechanical ventilation at a Vt of 6–8 mL/kg, respiratory rate of 10–14 breaths per minute and isoflurane as tolerated. The same procedure was followed for the CPR+defib and CPR-only groups, excluding medication administration for the CPR+defib group and excluding both defibrillation and medication administration for the CPR-only group. If an animal attained ROSC, CPR was immediately discontinued, hemodynamic monitoring (CO, SV, mean arterial blood pressure and pulse) and continuous isoflurane administration were resumed. For animals that failed to achieve ROSC, end point or termination of resuscitation was 20 min after initiation of CPR, and animals were then euthanized per facility protocol. For subjects that successfully achieved ROSC, postresuscitative monitoring continued for an additional 30 min before ending the experiment and euthanizing the animals.
Blood specimens (10 mL) were collected in EDTA tubes and immediately placed on ice. Samples were then centrifuged at 4000 rotations per minute for 10 min, and 2 mL of separated plasma was transferred into microcentrifuge tubes and frozen at −40°C for shipment. These samples were placed on dry ice and then shipped to the University of Washington’s Pharmacokinetic Laboratory for epinephrine assays. Epinephrine concentrations in plasma were determined using HPLC with tandem mass spectrometry as previously described in the literature and is considered a routinely used method for epinephrine assays in plasma.29
Statistical analyses
We used IBM SPSS V.22 software (IBM, Armonk, New York, USA) to analyze the data. We used a multivariate analyses of variance (MANOVA) to determine if there were statistical differences in the pretest data including weight, CO, SV, systolic blood pressure, mean arterial blood pressure, temperature, heart rate between each group and the total volume of blood exsanguinated. We also used MANOVA to determine if there were significant differences between the groups relative to the Cmax and Tmax. We used a repeated analyses of variance (RANOVA) to determine if there were significant differences in the MC between the groups at 0.5, 1.0, 1.5, 2.0, 2.5, 3.0, 4.0 and 5 min following the initial dose of epinephrine. When statistical significance was achieved, we used a least significant difference post hoc test. A χ2 test was used to determine if there were differences in the rate of ROSC between the groups.
Results
Statistical analysis using MANOVA indicated no significant differences in the pretest data by group. All the groups were equivalent to weight, age, systolic and diastolic blood pressure, mean arterial pressure, heart rate, CO, SV, end-tidal carbon dioxide, oxygen saturation and temperature (p=0.323) (table 1).
Pretest demographic data by group
RANOVA of hemodynamic measurements (eg, heart rate, mean arterial pressure, CO and SV) collected before and after exsanguination and every 5 min during the 20 min of resuscitation determined that there were no significant differences between the groups (p>0.05). There were no significant differences in the number of defibrillations and description of number of pulseless shockable and non-shockable rhythms (p>0.05) between groups. Subjects in IV, HIO and CPR+defib groups were all observed to be in a pulseless non-shockable rhythm after the third defibrillation and two doses of epinephrine.
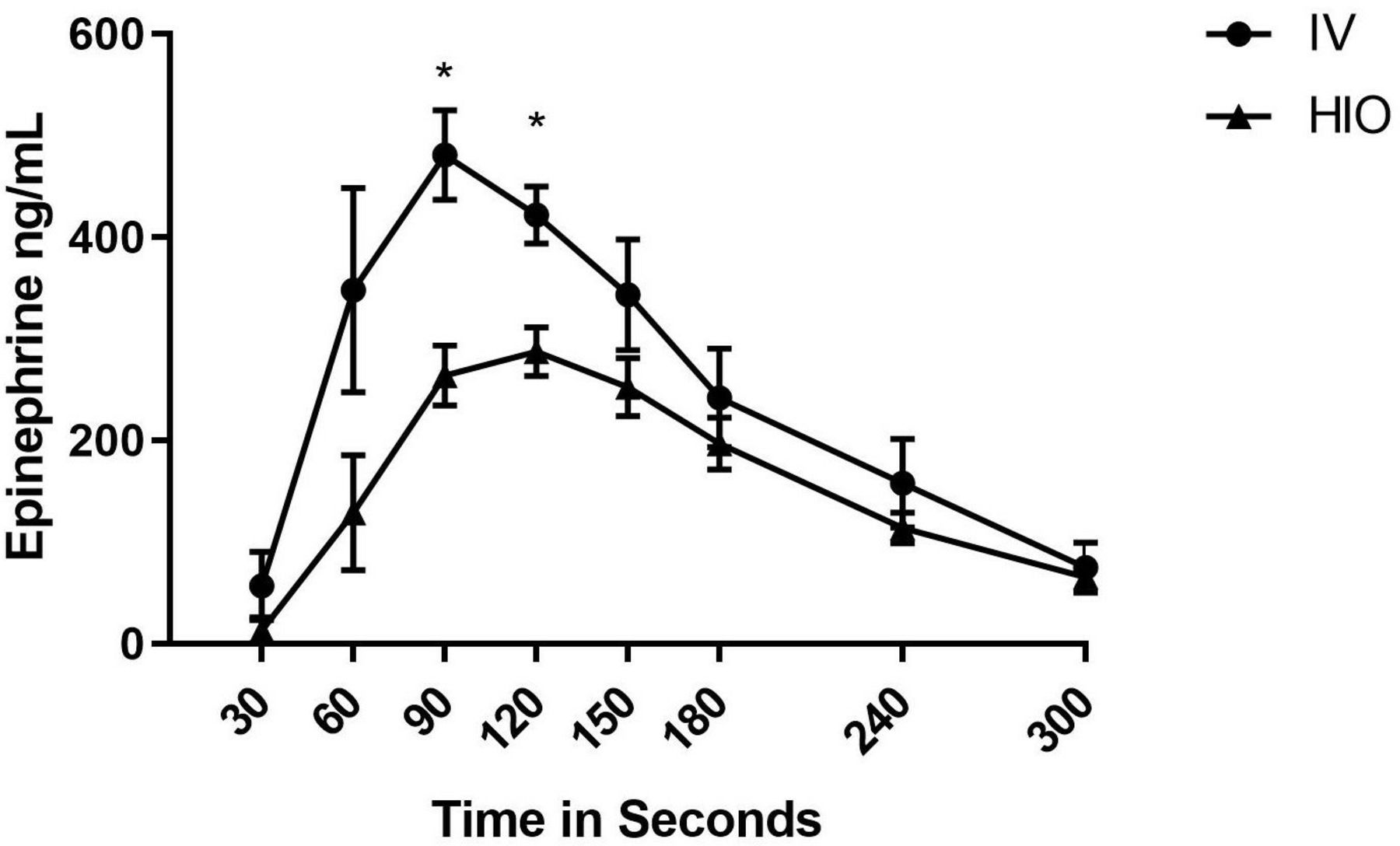
Following exsanguination and CA (pulseless ventricular fibrillation) of all groups, epinephrine (0.01 mg/kg) was administered by either IV or HIO route 2 min after the initiation of CPR with the exception of the CPR+defib and CPR-only group. Blood samples were collected at 0, 0.5, 1.0, 1.5, 2.0, 2.5, 3.0, 4.0 and 5 min between groups. Blood gases were also collected during this time period and throughout resuscitation. A RANOVA indicated that there were no significant differences in pH and base excess between IV and HIO groups (p=0.484). The IV group had a mean±SD pH and base excess of 7.32±0.15 and −9.6±3.43, respectively. The HIO group had a mean±SD pH and base excess of 7.27±0.10 and −6.4±3.54 correspondingly. We compared the MC at the repeated time measures. Significant differences were only observed at 90 s (p=0.001) and 120 s (p=0.003) between IV group and HIO group (figure 1).

Mean concentration±SE of the mean over time between IV (n=7) and HIO (n=7) groups. *Significantly different between IV and HIO groups observed at 90 s (p=0.001) and 120 s (p=0.003). HIO, humeral intraosseous; IV, intravenous.
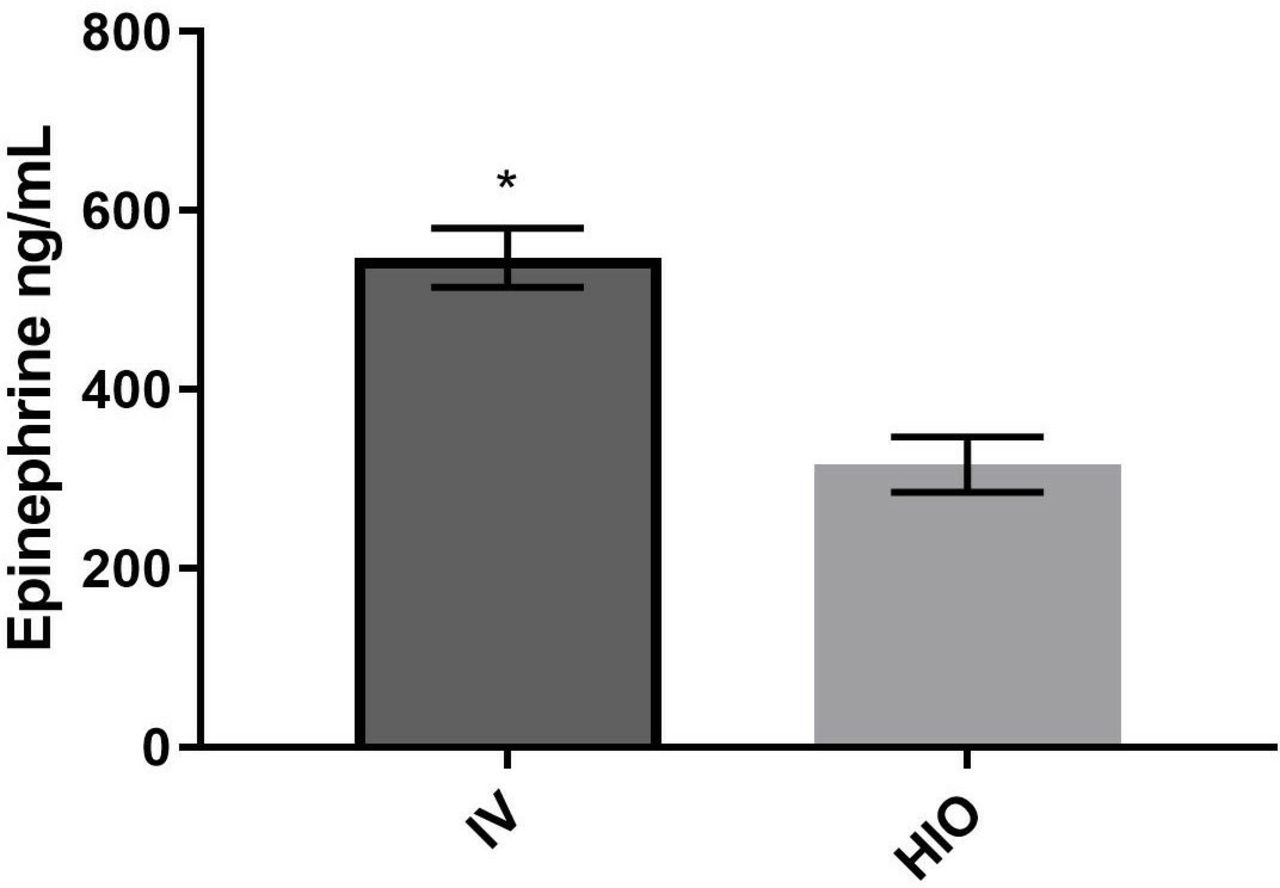
Cmax of epinephrine, measured in nanograms per milliliter (ng/mL)±SE of the mean, was compared for the HIO and IV groups. The IV group (n=7) had a mean concentration of 547 ng/mL; the HIO group had a mean concentration of 316 ng/mL. Statistical analysis demonstrated significant differences in Cmax by group (p=0.001) (figure 2).

Mean values for Cmax of epinephrine between IV group (n=7) and HIO group (n=7). Mean concentrations±SE of the mean expressed in ng/mL. *Significant difference between IV mean concentration (547 ng/mL) and HIO mean concentration (316 ng/mL) with a p value of 0.001. Cmax, maximum concentration; HIO, humeral intraosseous; IV, intravenous.
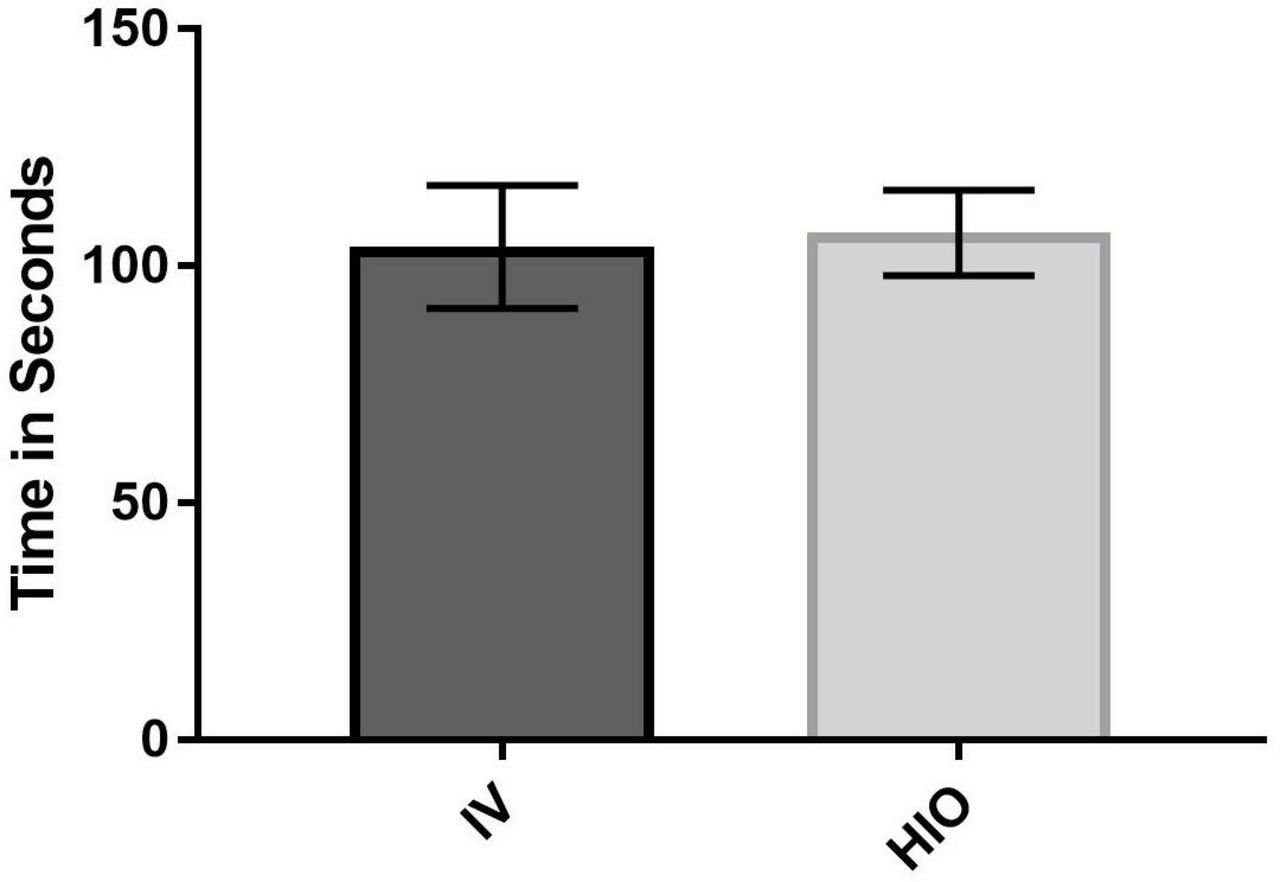
Tmax of epinephrine±SE of the mean in blood was compared for the HIO and IV groups. There was no significant difference in Tmax of epinephrine between groups. The IV group reached mean Tmax of 103 s compared with the HIO group at 107 s (figure 3).
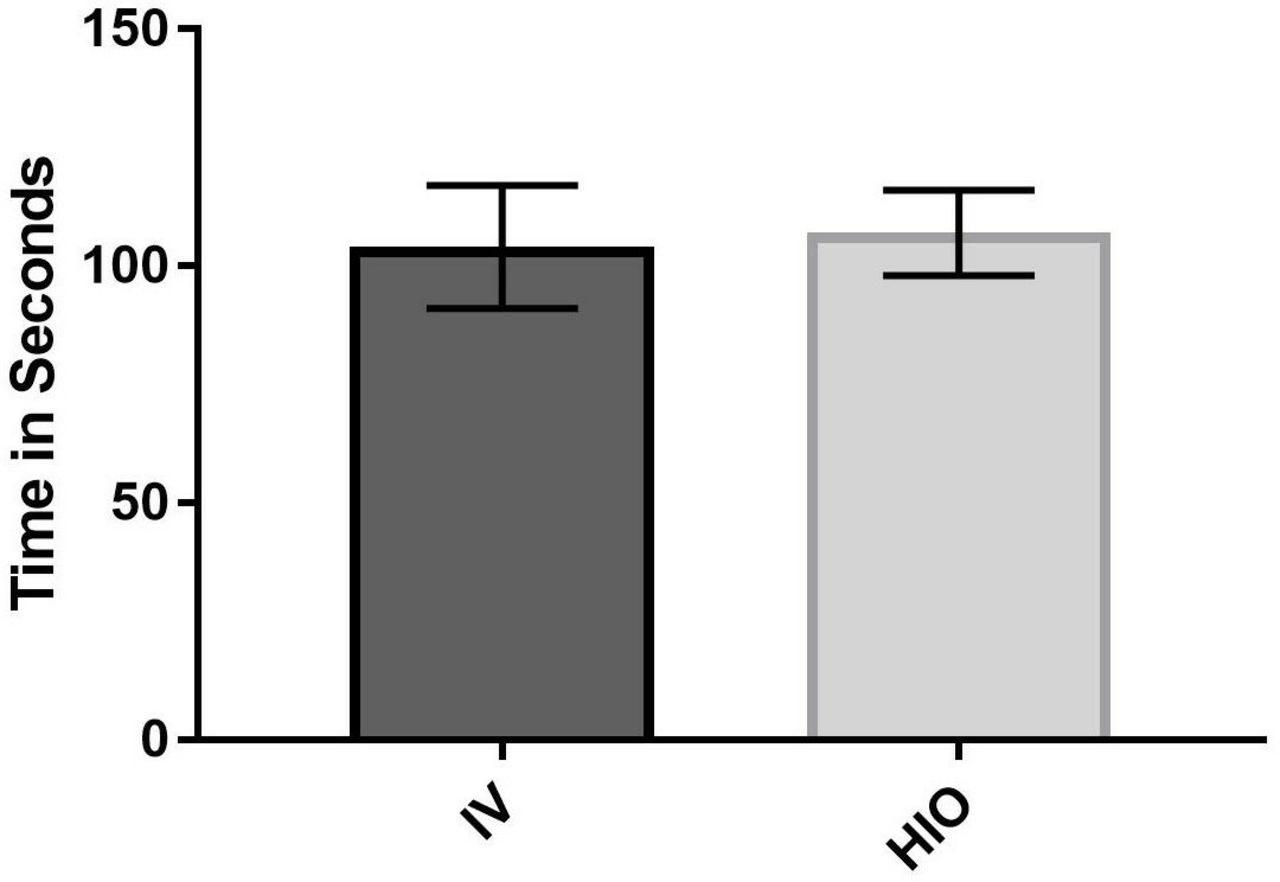
Mean values for time to reach maximum concentration (Tmax)±SE of the mean of epinephrine between IV group (n=7) and HIO group (n=7). Tmax expressed in seconds. Tmax IV (103 s) and HIO (107 s); p=0.789. HIO, humeral intraosseous; IV, intravenous.
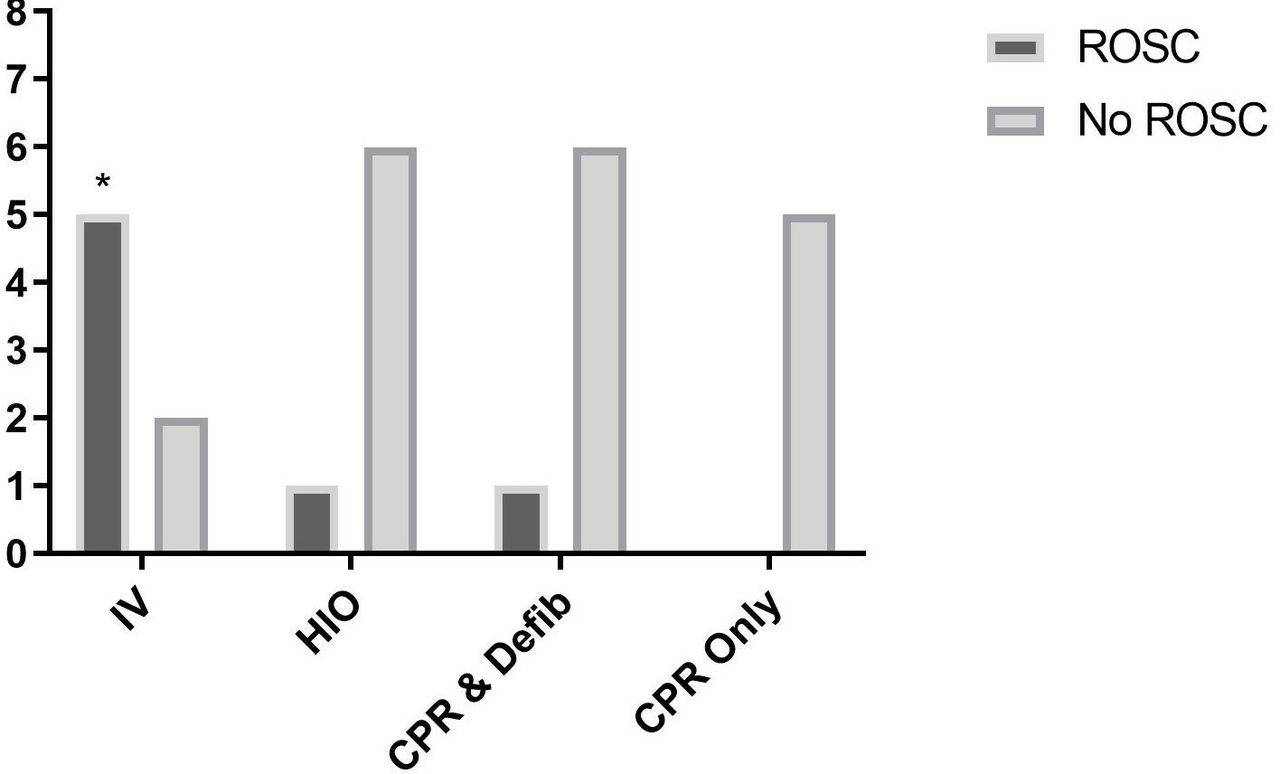
ROSC was achieved in five of seven subjects in the IV group. In the HIO group and in the CPR+defib group, only one of seven subjects achieved ROSC in each cohort. In the CPR-only group (n=7), none of the subject achieved ROSC. Using a χ2 test, significant differences were observed between the IV group and HIO group (p=0.031), IV group and CPR+defib group (p=0.031) and the IV and control CPR-only (n=7) group (p<0.001) (figure 4). No differences were found between the HIO and CPR+defib group (p>0.05), HIO and CPR-only group (p>0.05) and CPR+defib and CPR-only group (p>0.05). All subjects that failed to achieve ROSC, except in the CPR-only group, were administered similar number of defibrillations with similar energy levels during the resuscitation per recommended PALS guidelines.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of subjects (y-axis) experiencing ROSC for each experimental group (x-axis). Five subjects achieved ROSC in IV (n=7) group, one subject in the HIO group (n=7), one subject in the CPR+defib group (n=7) and NO subjects in the CPR-only group (n=5) achieved ROSC. Using a χ2 test, the IV group was significantly higher than the HIO group (p=0.031), CPR+defib group (p=0.031), the IV and control CPR-only groups (p<0.001). *Significantly different with a p<0.05 between IV and all other groups in the incidence of ROSC. There were no significant differences in ROSC between the HIO, CPR+defib group (p>0.05), CPR-only group (p>0.05). CPR+defib, CPR+defibrillation; HIO, humeral intraosseous; IV, intravenous; ROSC, return of spontaneous circulation.
Discussion
The aim of this study was to investigate and compare the effects of epinephrine administration by IV and HIO routes in a hypovolemic pediatric CA porcine model. We specifically examined the pharmacokinetic data (Cmax, Tmax and MC over 5 min) and rate of ROSC of epinephrine administration between HIO and IV access. We observed that the IV epinephrine administration in MC over 5 min (specifically at the 90 s and 120 s marks), and Cmax demonstrated significantly higher epinephrine concentrations than the HIO group. In terms of ROSC, our data demonstrated that there was a greater number of animals achieving ROSC for the IV groups (5 out of 7) than all the other groups (HIO and CPR+defib groups=1 out of 7 each and CPR-only group=0 out of 7). However, when we compared the HIO and CPR+defib groups, we observed no differences. We also observed that there was no difference in Tmax for either the IV or HIO groups.
The AHA PALS guidelines recommend epinephrine be administered by the IV route, but if not attainable, the IO route can be used.15 However, according to the AHA, the evidence for the recommendations of drugs used for CA in pediatrics are primarily based on expert opinion as well as there were no studies showing the effectiveness of epinephrine by any route of administration in CA.15–17
Interestingly, our results are different from findings from other studies comparing administration of epinephrine via IV and IO routes in adult normovolemic porcine models, which exhibited that there were no significant differences in pharmacokinetics of either routes of administration, IV or HIO.10 12 24 27 30 31
Multiple factors may have contributed to the decreased effectiveness of epinephrine administration through the HIO route in the hypovolemic pediatric CA porcine model. Low flow state in bone marrow is associated with CA and CPR (approximately 25% of normal), and hypovolemia has also been reported to decrease blood flow significantly thus impairing bone marrow blood flow.32 33 Bone marrow blood flow is responsive to physiological stresses as well as humeral and neurogenic stimuli. In the presence of hemorrhagic shock, bone marrow pressure drops approximately 90% and rise to 60% of baseline after fluid resuscitation.34 35 Cumming investigated the effects of epinephrine when administered in a single dose intravenously and demonstrated a reduction of bone marrow blood flow up to 75% with every dose injected.36 We speculated that HIO epinephrine administration and its direct vasoconstrictive effect may produce an additive or synergistic effect with CA’s and CPR’s reduction of blood flow to and from the bone marrow. Subsequently, this results in lower Cmax, Tmax and MC of serum epinephrine, which influences the ability to achieve ROSC. Another factor that may have influenced poorer outcomes of HIO epinephrine administration is the metabolism of epinephrine within the bone marrow cavity. Red bone marrow, which produces blood cells, predominates the bone marrow cavity in pediatric patients as compared with adults.37 Epinephrine is metabolized by catechol-O-methyltransferase (COMT) and monoamine oxidase (MAO), both found in red blood cells and platelets, respectively.38 It is possible after epinephrine is injected into the bone marrow and with the low flow state from hypovolemia and CA with CPR that epinephrine is sequestered in the bone marrow cavity and thus metabolized as epinephrine is exposed to various blood components within the bone marrow cavity. However, further study is warranted to discern the mechanism of this event.
According to current AHA guidelines, pediatric epinephrine IV dosing is 0.01 mg/kg of bodyweight for pediatric CA.39 A study investigating the survival rate at 24 hours after CA using either high-dose epinephrine (0.1 mg/kg) or standard dose epinephrine (0.01 mg/kg) in pediatric patients found that high-dose IV epinephrine did not provide any benefits and may lead to worse outcomes compared with standard dose therapy.40 However, this study only examined IV administration of epinephrine and not IO administration. Due to the alteration with bone marrow blood flow and the possible prolonged exposure to COMT and MAO, a higher dose of epinephrine may be necessary to improve resuscitative outcomes, when using IO epinephrine in the hypovolemic pediatric CA porcine model. Further research investigating this unique event will be necessary to determine the effectiveness of increased epinephrine doses and the risk-benefit ratio.
Long et al examined the effects of HIO epinephrine administration versus IV using an adult normovolemic and hypovolemic CA porcine model.11 Long et al investigated both normovolemic and hypovolemic states in CA porcine models. In their study, they found no statistical difference between HIO epinephrine administration and IV in the normovolemic model. However, when comparing HIO access between the normovolemic and hypovolemic groups, they found the time to ROSC was significantly less in the normovolemic group as well as the MC of epinephrine was significantly higher in the normovolemic group. It was also noted that the hypovolemic HIO group had fewer subjects (three out of seven subjects) achieve ROSC as compared with both normovolemic HIO groups (seven out of seven subjects) and normovolemic/hypovolemic IV groups (four out of seven subjects for each group), which is clinically relevant. Our study supports and expands their findings using a pediatric hypovolemic CA porcine model.
Limitations
The investigators acknowledge the pig model of hemorrhagic CA used in this study may have limitations that may affect generalization of the results to humans. However, pig have anatomically and physiologically similar cardiovascular systems compared with humans and are an accepted model for resuscitative research.41 The deletion of two pig from the CPR-only group created heterogeneous groups, but this likely did not affect results. The investigators, in consultation with the local IACUC, decreased the size of CPR-only group from seven to five consistent with the ethical principle of reduction. The electrical method used to induce CA in the pig following hemorrhage does not accurately replicate the normal mechanisms of hemorrhagic CA in children. However, we believed a controlled time point of CA would minimize variability between subjects and increase the internal validity of the experiment. The sternal IO (SIO) route was not included in this study, as currently approved SIO devices are not indicated for use in children <12 years of age. The rate and time of autotransfusion of blood to the pig was variable as transfusion was accomplished using a single 18-gauge auricular IV. Future investigators are advised to transfuse using an 18-gauge IV catheter in each ear to decrease variability and be more consistent with human resuscitative practices.
Most importantly, the pharmacokinetic differences between the IV and HIO infusion sites found in this experiment may not be generalizable to human resuscitative outcomes. Future investigators may consider using a longer period of CA without intervention. Another possibility is increasing the amount of hemorrhage to an ASC class IV (>40% Epstein-Barr virus) to determine if amount of hemorrhage affects the occurrence of ROSC and survival with acceptable neurological outcome when epinephrine is administered by the IO and IV routes with ongoing resuscitation.
Conclusion
Our findings suggest that HIO administration of epinephrine in a hypovolemic pediatric CA porcine model is no more effective in achieving ROSC than CPR+defib alone. Based on our results, we recommend administering epinephrine via the IV route over HIO during CA in pediatric patients in the presence of hypovolemic shock. These findings challenge the current PALS guidelines which state that HIO is a viable alternative to IV access.
Acknowledgments
The authors would like to thank COL Denise M. Beaumont, DNAP, CRNA, Program Director (US Army Graduate Program in Anesthesia Nursing) for her support and allowing staff and students to participate in this study.
References
Footnotes
Contributors MJN, JMB, JO’S and DJ conceived and implemented study. In addition, analyzed the data, interpreted the results and wrote the manuscript. DB, BT, KR, RR, PA, TH and JN carried out the experiments under the direct supervision of MJN, JO’S and DJ. DB, BT, KR, RR, PA, TH and JN contributed to the interpretation of the data and wrote sections of the manuscript.
Funding This study was funded by TriService Nursing Research Program (N17-B06).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Naval Medical Research Unit, San Antonio Institutional Animal Care and Use Committee (IACUC) approved the research protocol to be conducted in their laboratory setting.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.