Article Text

Abstract
Background The primary goal of the present study is to describe the psychosocial support services provided at our institution and the evolution of such programming through time. This study will also report the demographics and injury patterns of patients using available resources.
Methods Trauma Recovery Services (TRS) is a social and psychological support program that provides services and resources to patients and families admitted to our hospital. It includes a number of different services such as emotional coaching from licensed counselors, educational materials, peer mentorship from trauma survivors, monthly support groups, post-traumatic stress disorder (PTSD) screening and programming for victims of crime. Patients using services were prospectively recorded by hired staff, volunteers and students who engaged in distributing programming. Demographics and injury characteristics were retrospectively gathered from patient’s medical records.
Results From May of 2013 through December 2018, a total of 4977 discrete patients used TRS at an urban level 1 trauma center. During the study period, 31.4% of the 15 640 admitted adult trauma patients were exposed to TRS and this increased from 7.2% in 2013 to 60.1% in 2018. During the period of 5.5 years, 3317 patients had ‘direct contact’ (coaching and/or educational materials) and 1827 patients had at least one peer visit. The average number of peer visits was 2.7 per patient (range: 2–15). Of the 114 patients who attended support groups over 4 years, 55 (48%) attended more than one session, with an average of 3.9 visits (range: 2–10) per patient. After the establishment of PTSD screening and Victims of Crime Advocacy and Recovery Program (VOCARP) services in 2017, a total of 482 patients were screened for PTSD and 974 patients used VOCARP resources during the period of 2 years, with substantial growth from 2017 to 2018.
Conclusions Hospital-provided resources aimed at educating patients, expanding support networks and bolstering resiliency were popular at our institution, with nearly 5000 discrete patients accessing services during a period of 5.5 years. Moving forward, greater investigation of program usage, development, and efficacy is necessary.
Level of evidence Level II therapeutic.
- trauma recovery services
- trauma survivor network
- psychosocial
- peer mentorship
- support group
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Social, economic and psychological parameters are becoming increasingly accepted as having substantial bearing on recovery after traumatic injury. Preinjury mental illness is pervasive among trauma patient populations with reported rates as high as 45%.1–8 Substance use is also ubiquitous among trauma patients.9 10 After injury, mental illness and substance use disorders are associated with higher rates of complications, worse functional outcomes, poor treatment adherence, and an increased risk for later recidivism.2 4 7 8 11–17 Mental illness has also been shown to negatively impact patient satisfaction.18 19 However, patients with high activation levels, those partaking more in their care experience, tend to experience greater satisfaction.19
There has been limited study of interventions among trauma patient populations to address these issues. Promisingly, a few single-center studies have shown favorable results in limiting opioid use, instituting peer mentorship programs, and bolstering mental health resources.20–24 The Major Extremity Trauma Research Consortium (METRC) has also sought to address psychosocial issues through a multicenter prospective trial. The resulting Trauma Collaborative Care Study (TCCS) provided Trauma Survivors Network (TSN) programming at study institutions, with reported benefit to patients and providers alike.23–26 Despite encouraging results, more research is warranted to promote establishment and expansion of similar interventions.
Our institution’s psychosocial support program, Trauma Recovery Services (TRS), began through TCCS and has since evolved to offer new services and resources not originally encompassed by TSN or TCCS. The goal of the present study is twofold: (1) to describe services at our institution and the evolution of programming through time, and (2) to report the demographics and injury patterns of patients using available resources, to target services to populations who may use and benefit from them.
Methods
Overview of study and variables of interest
During the course of a period of 5.5 years (May 2013 through December 2018), 4977 discrete patients used TRS at an urban level 1 trauma center. The majority of patients targeted for services were those admitted to the hospital, with the exception of post-traumatic stress disorder (PTSD) screening and victims of crime services. Chart review was conducted for patients who used services beyond direct contact (educational materials and/or coaching) and Victims of Crime Advocacy and Recovery Program (VOCARP) services alone, which was applicable for 2324 patients. Demographics and background information such as age, sex, marital status, race, ethnicity, primary emergency contact, employment status, and insurance were retrospectively collected from the electronic medical record. Injury characteristics including mechanism, region of injury (head/neck, face, chest, spine, abdomen, pelvis, upper extremity or lower extremity) and hospital length of stay were similarly recorded.
Founding TRS
The development of psychological and social resources for trauma patients and families, referred to as TRS at this trauma center, began through TCCS via METRC. This was a multicenter study designed to study its effects on clinical and functional outcomes after high-energy orthopedic trauma, through introducing patients at six intervention sites to similar services. Since its initiation, TRS at our hospital subsequently evolved by modifying or discontinuing services patients did not find useful and through implementation of new programs tailored to our unique patient population and the needs of the surrounding community. See table 1 for greater detail.
Overview of services offered through Trauma Recovery Services
Direct contact
‘Direct contact’ refers to offering patients educational materials and/or personalized coaching. Both services were offered from TRS program onset in 2013. Specifically, patients received the TSN Handbook for Trauma Patients and Their Families. This text includes explanations of common injuries and typical treatments for these injuries. The handbook also provides lay information about hospitals, services and policies. Patients who receive the TSN Handbook are also informed about the TSN website, which can serve as another resource for information and guidance after injury. In May 2017, after the development of the TRS App (http://bit.ly/traumaapp), patients could also access similar, and more detailed information from this application on their mobile device. Individualized coaching visits sometimes accompanied receiving educational materials. A trauma recovery coach, a trained member of the TRS program that helps provide emotional coaching, support and education to patients and families, initiated these sessions. Coaches likewise would advise patients and families about resources available to them or initiate higher level referrals, as necessary. In our program, coaches have Master of Education degrees in counseling or Master of Public Health degrees, and are licensed professional counselors. At the onset of programming in 2013, there was one full-time coach available for all patients admitted after trauma activations. This single coach represented a limited resource, who was unable to reach every patient. There are now two full-time counselors who provide coaching and related services, but there are still patients with unmet needs or patients who decline to use services. TRS providers attempt to identify new trauma patients who may benefit from services and to make resources available to as many of them as possible. Trauma physicians and other providers in the system could also initiate consult requests for TRS coach, at their discretion.
Support groups and family classes
In May 2013, support groups, family classes, and NextSteps classes were offered. Support groups are offered monthly and are confidential meetings that allow patients and family members to speak about their experiences and to support one another. In the month of May, a National Trauma Survivors Day celebration is offered in lieu of a regular meeting. This is an opportunity for patients and families to come together along with healthcare providers to celebrate recovery and engage in fellowship. In December, a holiday potluck dinner is held, instead of a regular support group meeting. Initially, support groups were tailored for general trauma populations, but have expanded to be more inclusive to amputees, patients who have sustained a traumatic brain injury (TBI) and their families. Family classes were initially designed to help prepare family members to take on caregiving roles and offered family members the opportunity to connect with others in similar circumstances. Family classes were discontinued in 2015, due to low utilization levels. All support groups, family classes and NextSteps classes are run by TRS coaches.
Peer mentorship
Peer mentorship also began in May 2013. Each peer visitor is a trauma survivor, with his or her own story of a traumatic experience or injury. Peer visitors offer patients and families the opportunity to connect with someone who understands their position and to ask questions. Peer visitors offer wisdom, encouragement, and hope, so that each patient and family member may recognize peer support and understanding during their recovery. At program onset in 2013, ten peer volunteers were trained by TRS coaches. By 2018, there were 24 peers, with over 500 hours of services offered to patients.
‘We’ve got you covered’ comfort bags
In December 2014, peer mentors suggested the addition of this program and have since participated in donating and preparing comfort bags for patients. These comfort bags are presented shortly after admission and contain personal items for hygiene and other basic needs, many of which may have been lost during the injury. Some of the materials included are socks, tissues, notebooks, lip balm, hand sanitizer, combs/brushes, dental hygiene products, reading glasses, puzzles and blankets.
Victims of crime
In March 2017, TRS expanded to offer the VOCARP. VOCARP identifies victims of crime within the hospital system and recommends resources and education to patients and their families. These include, but are not limited to, compensation, information about the criminal justice system, referral to internal or external resources, relocation assistance, and individualized counseling. These victim advocacy services are provided by five social workers who are available at any time to meet with patients in the emergency department (ED), during their hospitalization, or at outpatient clinic visits. Additionally, social workers may contact patients via phone if providers request a referral.
PTSD screening
PTSD screening began in June 2017. For this screening, the PTSD checklist for Diagnostic and Statistical Manual for Mental Illness, Fifth Edition (PCL-5) is administered during a patient’s first postdischarge outpatient clinic visit. Patients at general trauma or orthopedic trauma clinic visits are identified for survey. Surveys are distributed by nursing staff and were scored by coaches. However, not all identified patients receive the PCL-5 due to personnel, time, or patient-related constraints. All patients screened positive for PTSD (score ≥33) are contacted by TRS coaches and offered ancillary services for intervention such as support groups, counseling and outpatient psychotherapy.
Results
Overview and patient capture
From 2013 until 2018, there were a total of 32 637 trauma activations at our institution. Although the mean age of all trauma patients was slightly younger compared with those using TRS (43 years vs. 45.4 years, p<0.001), neither population was different in terms of sex (both 64% male). Among all trauma activations the most common mechanisms of injury were falls (33.5%), motor vehicle collisions (MVC; 28.7%) and penetrating trauma (gunshot wounds or stabbings: 12.2%). Of the 32 637 trauma activations, 16 997 patients (52.1%) were discharged home from the ED. 31.4% of admitted patients used TRS during the study period. This increased from 7.2% of admitted patients using services in 2013 to 60.1% of admitted patients in 2018.
Demographics of the study population
Between 2013 and 2018, a total of 4977 patients used TRS, with 2324 patients (46.7%) receiving more than direct contact or VOCARP services, only. Of these 2324 patients, the mean age was 45.4 years (SD=18.5) and 64% were male (table 2). The majority were Caucasian (69%), single (48.8%) and had Medicaid as their primary insurance coverage (39.1%). Equivalent numbers of patients were employed (40.6%) or unemployed (40.2%) at time of presentation.
Patient demographics for all who had resource utilization beyond educational materials, coaching, or VOCARP (n=2324 of 4977). Frequency (%) is based on the number of patients with available data
Injury characteristics of the study population
The mean hospital length of stay was 10 days (SD=11.2). Mechanisms of injury were variable, with MVCs (31.8%), falls (25.3%), penetrating trauma (13.9%), and motorcycle collisions (MCC, 12%) representing the primary etiologies. See table 2. Of these 2324 patients, 1519 (67.7%) had at least one orthopedic injury, including those to the spine, pelvis, or extremities. The most common injuries were to the lower extremities (39.7%), chest (24.7%), upper extremities (20.4%) and head/neck (19.1%).
Use of TRS
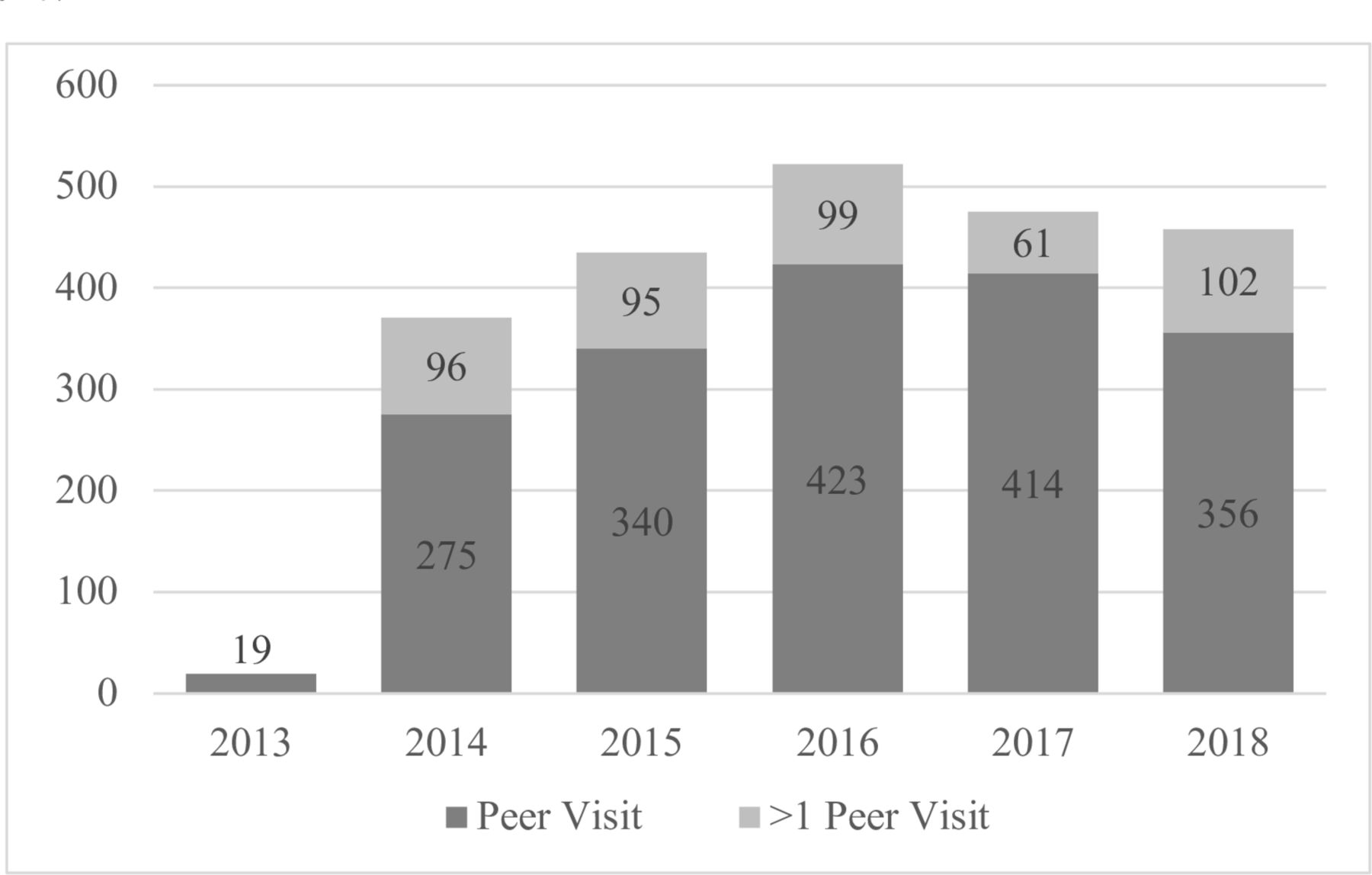
The total number of discrete patients using TRS rose from 209 in 2013 to 1388 in 2018. Although the number of direct contacts reached a plateau between 550 and 700 each year, the total number of patients informed about resources spiked to 1443 in 2017 and remained steady in 2018. Peer visits also became more frequent with program expansion and, accordingly, there was a steady growth in peer visits from 2013 to 2016 (figure 1, supplemental digital contact).
From 2014 to 2018, between 50 and 100 patients received more than one peer visit. The average number of peer visits in this population was 2.7 and the median was 2.0 (range: 2–15).
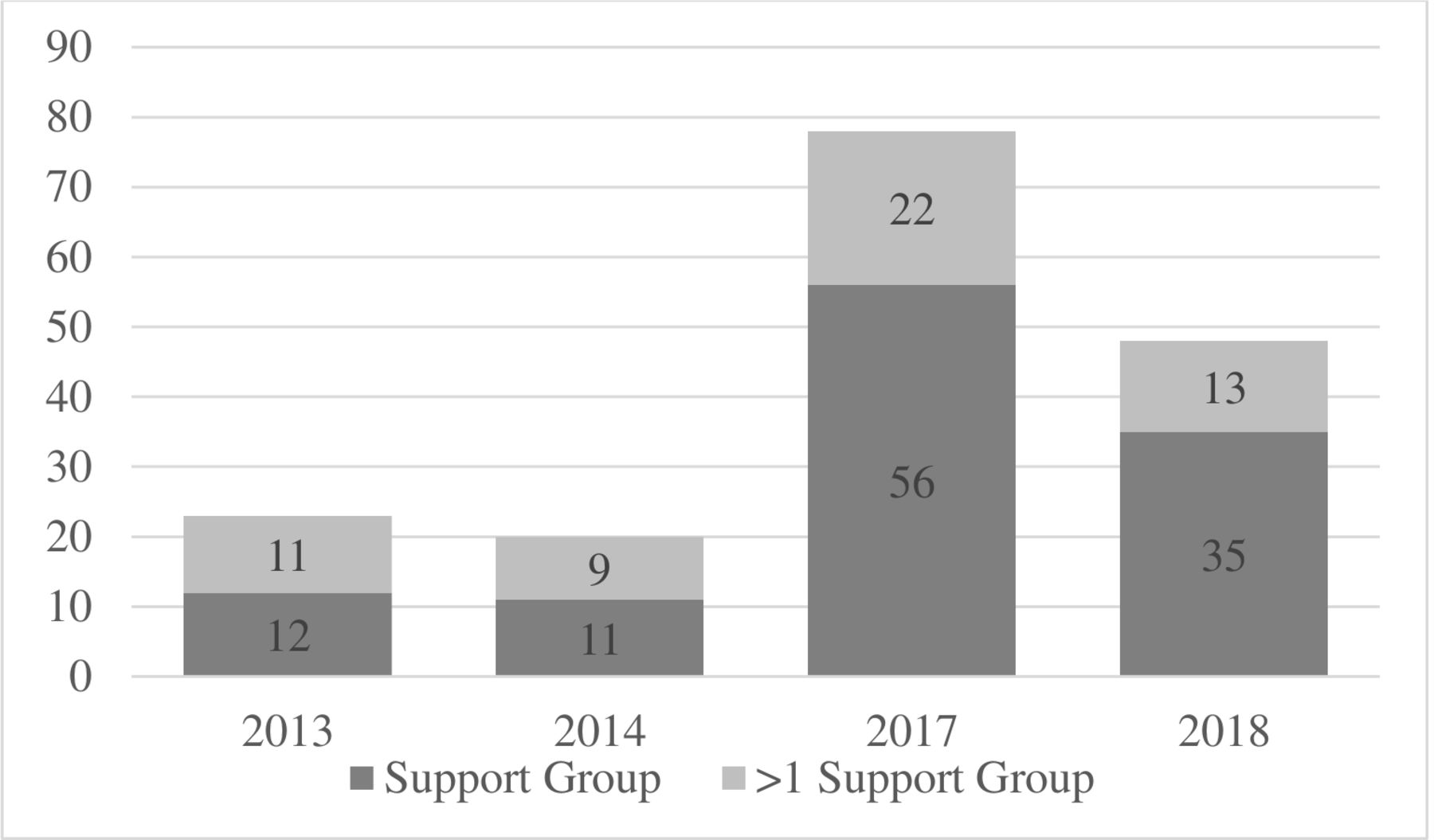
Support groups also became more widely used over time, with the highest attendance seen in 2017 (Figure 2). Of the 114 patients who attended support groups over 4 years, 55 (48%) attended more than one session, with an average of 3.9 visits and median of 3.0 visits (range: 2–10) per patient. The onset of PTSD screening and VOCARP services in 2017 led to 482 patients being screened for PTSD within a period of 2 years and 974 patients using VOCARP resources as well, with substantial growth from 2017 to 2018 (table 3).
Summary of services used from 2013 to 2018
Demographics and injury characteristics per resource utilization
Patients who used different services (>1 peer visit, support groups, VOCARP, and PTSD screening) had varying demographics (table 4). In particular, patients using VOCARP resources were younger (33 years vs. 44 years), were more often male (78% vs. 60% to 65%), single (76%), and were less often Caucasian (30% vs. 60% to 73%), all p<0.02.
Breakdown of patient demographics and injury patterns for different services used. Frequency (%) is based on the number of patients with available data
The majority of patients who attended support groups were married or had a significant other (56% vs. 20% to 40%) and were often employed (52% vs. 26% to 45%), both p<0.001. Patients with >1 peer visit had longer average hospital stays: 16.7 days (SD=14.9). MVCs and MCCs were more common mechanisms for patients with >1 peer visit and support group attendees, whereas VOCARP users had substantially more penetrating trauma (78%, p<0.0001).
The majority of patients receiving a peer visit (n=1827) only had one visit (73%). Eighteen percent of these patients had two peer visits, and 9% had three or more, with one patient receiving 15. Patients with more peer visits were younger but were no different in terms of sex or marital status (table 5). Patients with more peer visits were less often retired (9% vs. 16% to 17%, p=0.02), but were no different in terms of rates of employment. Patients with three or more peer visits were less likely to be injured by falls (8.4% vs. 20% to 25%) and were more likely to present after MCCs (24% vs. 12% to 16%), both p<0.001, potentially related to hospital stay. As the number of peer visits increased, patients had longer associated hospital stays (1 visit: 9 days; 2 visits: 14 days; 3+ visits: 23 days), p<0.001.
Breakdown of patient demographics and injury patterns by number of peer visits. Frequency (%) is based on the number of patients in a given column with available data
Discussion
Since program initiation in May 2013 through December 2018 nearly 5000 unique patients were reached by TRS at our institution. Patients represented a wide variety of social and economic backgrounds, being inclusive to both employed and unemployed individuals, those with both low and high levels of social support, and to the young and elderly alike. Close to half of all patients (2324 of 4977, 47%) had resource use beyond direct contact or VOCARP services alone. This group represents patients who demonstrated greater engagement with the programming, thus were studied in more detail.
Psychosocial resources for trauma patients including educational materials, counseling, peer mentorship, and support groups are not widespread among trauma systems; therefore, prior investigation of their use is limited. Peer mentorship programs are most notable among patients with spinal cord injuries,27 28 TBI29 or for military veterans.21 Several positives include heightened self-efficacy, better coping mechanisms and bolstered use of mental health resources.21 27–29
Aside from peer mentorship, there has been more limited study of resources similar to those provided at our institution. In a preliminary study of the TSN, Castillo et al found use of such programs to be limited, even when available to patients. Of the 94 participants with follow-up data (out of 126) in their study, 3% reported attending NextSteps classes, 6% attended support groups, 10% met with a peer visitor, 17% visited the TSN website and 27% received the TSN Handbook.22 In some respects, these results are similar to our findings. At our institution, support groups and family/NextSteps classes were not well attended, with a participation rate of 2.3%. However, patients who did participate appeared to benefit, as 48% attended more than one session, with a median of three visits per patient. Other resources were more popular: 40.6% of our patients received a peer visit and 73.7% received direct contact, which includes educational materials and/or personalized coaching. Therefore, our TRS program as a whole was much more used than like interventions in prior reports.
VOCARP was a recent addition to TRS at our hospital, beginning in March 2017, due to a grant from the State of Ohio to support this type of programming. Programming includes financial resources, education about criminal justice and victim rights, general and personal advocacy, emergency resources, individual and group counseling, and referrals for both internal and external services. Major goals of such programming are to increase patient education and engagement, to promote recovery and well-being in the community, and to limit recidivism in this high-risk group. Although new to our institution, other hospitals around the country have investigated the impact of similar violence intervention programs.30–34 These programs have noted a number of benefits including reduced recidivism, cost savings, and transformed attitudes about violence and shame.32–34 In future studies, we hope to explore VOCARP in greater detail, focusing on possible associations with mental illness, recidivism and outcomes.
Many interventions in healthcare never reach widespread implementation. This is poignantly true for psychosocial resource programs similar to our own. One reason behind this trend is that many high-risk groups, including those with cancer, HIV, and autoimmune diseases, are reluctant to use such services.35–39 For example, a foremost barrier to attending support groups among these populations is a lack of perceived need.38 39 In many respects, this is true for trauma patients as well. These patients may be encumbered by psychiatric illness, social habits, and inadequate support systems that create challenges for managing clinical adherence, let alone promoting use of elective services.8 18 Environmental resources may also impede patients from accessing available programming. Many patients live far away or rely on family and friends to provide transportation after injury. Therefore, patients with lower social support might have more difficulty securing resources, even if they are in greatest need. Some critically injured patients are also not discharged directly home after injury. Patients recovering for extended periods in skilled nursing facilities or rehabilitation centers will not have access to resources provided within the hospital. Provider and institutional barriers may hinder establishing programming as well. Specifically, Bradford et al investigated barriers to fully introducing TSN resources.40 In a survey of providers trained to launch these services at 30 centers, the foremost obstacles to implementation included lack of time, insufficient funding, institutional barriers and poor collaboration among departments.40 We realized more provider knowledge of programming and more collaboration among providers within the first years of TRS implementation. We also aggressively sought internal and external funding resources to support program continuation and growth once the TCCS grant funding was expended.
Shortly after program inception in 2013, internal and external funders were solicited, recognizing that program sustainability would not necessarily occur if reliant completely on our hospital system operating budget, regardless of demonstrating program efficacy. By 2015, we were able to support a portion of theTRS budget with funds outside of our hospital system. Since the TCCS grant support ended, the TRS program has been supported by our hospital operating budget and by external resources. Additional funding from the State of Ohio, which was acquired in 2017, has afforded robust resources including personnel to address those trauma patients who are victims of crime.
This study does have several limitations. Despite prospective accumulation of patients using TRS resources, data collection may have been incomplete. As multiple team members including counselors, interns, and volunteers are all involved in distribution of programming, data management was inconsistent. This led to under-reporting, most notably of those who attended support groups in 2015 and 2016 and those who received comfort bags in 2016. Given the small sample sizes of these particular programs, we do not think that this skewed the general population demographics, though it may have impacted subgroup analyses. Given program design, it was not feasible nor ethical to offer programming to individual patients while preventing a control group from having any exposure to available services. These thoughts were similarly reflected by Castillo et al and are a reason behind the institution-wide provision of TSN resources during the TCCS study.22 23 Finally, this study does not measure satisfaction; therefore, we cannot objectively speak to patient valuation of available resources. However, prior work at our institution identified more patient satisfaction among trauma patients who felt more confident about likelihood to recover.41 Going forward, the authors would like to more critically investigate satisfaction, as well as the intersection of TRS and opioid consumption, new or untreated mental illness, and clinical outcomes related to injury.
Hospital-provided resources aimed at educating patients, expanding support networks and bolstering resiliency were popular at our institution, with close to 5000 discrete patients accessing services during a period of 5.5 years. With growth of available resources over time, more patients were able to be ‘touched’ by TRS. Program evolution during this time also allowed for adaptation to specific trauma populations pervasive in our community. It is clear that there is patient demand for such programming and that it will not go unused if made available.
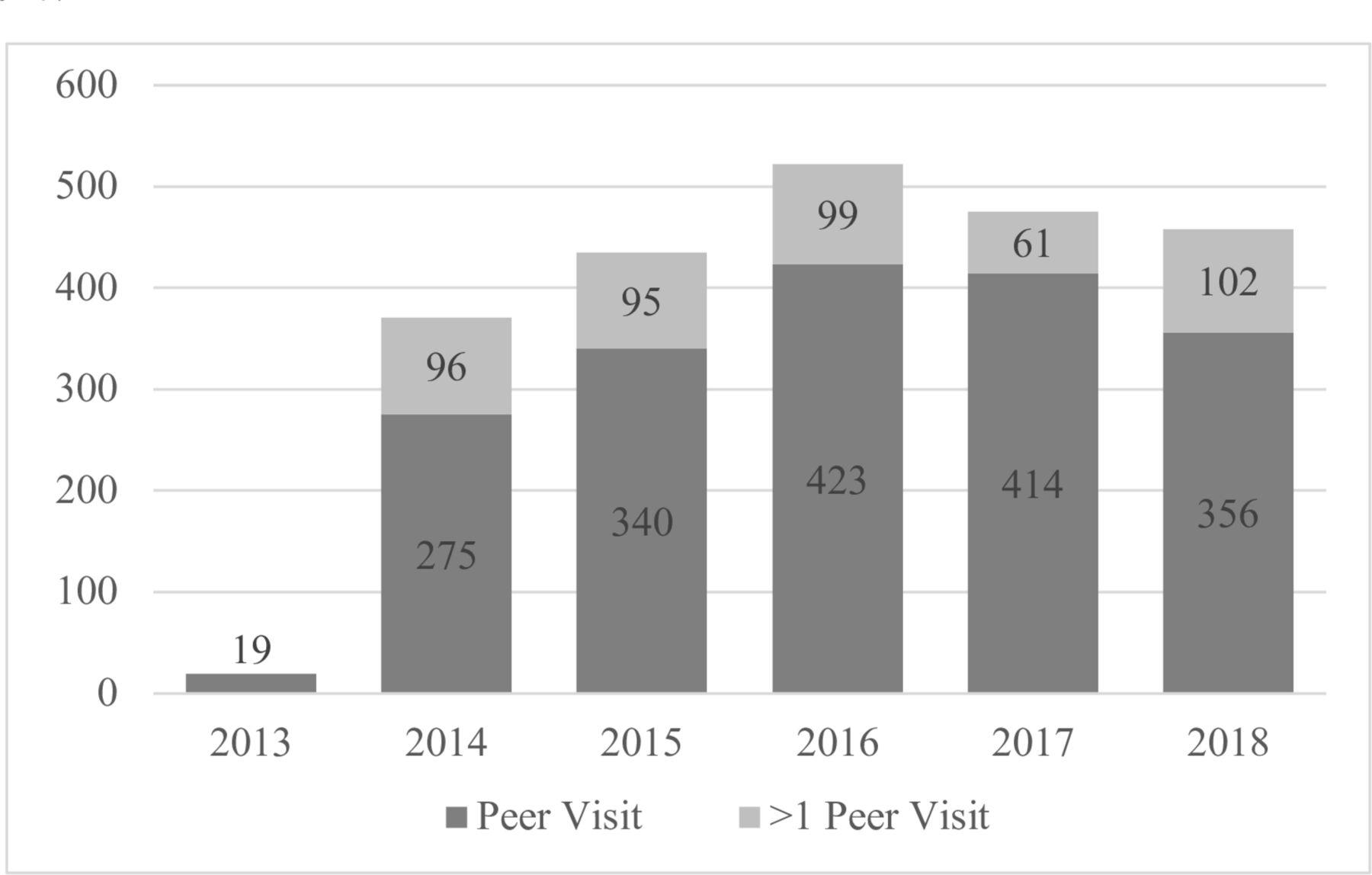
Total number of discrete peer visits and number of peers with more than one visit from 2013 to 2018.
{kind=link}
{kind=link}
Total number of patients attending support groups from 2013 to 2018, along with the number of patients attending >1 support group. *Support group data were unavailable for 2015 and 2016.
Acknowledgments
We gratefully acknowledge the providers of trauma care in the MetroHealth System for their attention to continuous improvement in the management of injured people.
References
Footnotes
Contributors NMS participated in literature search, data collection, data analysis, data interpretation, writing and critical revision. TR participated in data collection, data interpretation, and critical revision. MAB participated in study administration and design, data collection, data interpretation and critical revision. SBH participated in program leadership and critical revision. MK participated in critical revision. MS participated in programming and critical revision. VPH participated in data interpretation and critical revision. HAV participated in study design, data collection, data interpretation, writing and critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. For access to data please contact HAV: hvallier@metrohealth.org.