Article Text

Statistics from Altmetric.com
Case description
The patient is a 68-year-old man with a history of prostate cancer metastatic to the testicles and obstructive lower urinary tract symptoms who failed medical management and multiple partial transurethral resections of the prostate (TURP). Prior to the operation, his plasma sodium was measured at 141 mmol/L. He underwent a repeat TURP with a plan for definitive radiotherapy to follow. The operation lasted approximately 90 minutes. Early in the case, several small blood vessels were transected and cauterized, resulting in minor bleeding with an estimated blood loss of 50 mL. During the procedure, the patient underwent continuous bladder irrigation with approximately 15 L of sorbitol. Immediately postoperatively, his plasma sodium was measured to be 95 mmol/L (normal 135–145 mmol/L). Measured serum osmolality was 268 mOsm/kg and calculated osmolality was 303 mOsm/kg (osmolal gap 68). His anion gap was 14 mmol/L. His arterial blood gases were acidotic with pH 7.2. His glucose was normal at 100 mg/dL.
What would you do?
Lasix drip.
Dialysis.
Rapid correction of sodium with hypertonic saline.
What we did and why
C. Rapid correction of sodium with hypertonic saline.
TURP syndrome is a type of severe iatrogenic hyponatremia (serum sodium <120 mmol/L) that can occur during endoscopic urologic or gynecologic procedures requiring continuous irrigation. Hypotonic solutions (1.5% glycine, 3% sorbitol, or 5% mannitol) are required for the use of unipolar cautery because they are non-conducting. However, in rare cases, they can be rapidly absorbed through exposed venous plexuses, causing hyponatremia and fluid overload. Risk factors for the development of TURP syndrome include increased operative time, type of anesthesia (general anesthesia vs. spinal), increased vascularity and bleeding, visceral perforation, and pressure of irrigating fluid.
Several strategies to reduce the risk of TURP syndrome have been proposed. The most effective is to perform the operation with bipolar cautery, thus allowing irrigation with isotonic saline. Studies have shown an almost negligible change in serum sodium using such solutions1. However, fluid overload and congestive heart failure can still occur if more than 2.5 L of fluid is absorbed systemically If unipolar cautery is required, operating room staff can estimate the fluid deficit in real time by measuring the volume of irrigation used and subtracting the volume removed by suction. A fluid deficit threshold of 1 to 1.5 L has been found to significantly increase the risk for developing neurologic symptoms due to TURP syndrome. However, this technique can be challenging as blood and urine mix with the irrigation, complicating accurate estimates. If spinal anesthesia is employed, the patient’s neurologic status can be monitored intraoperatively; if general anesthesia is performed, the patient may not manifest symptoms until arrival in recovery. Our patient was under general anesthesia and became progressively hypoxic during the second half of the operation, providing early warning that he absorbed a significant amount of fluid and was developing pulmonary edema. Indeed, in the post-anesthesia care unit, his respiratory rate was 31 and he required 10 L non-rebreather oxygen mask to achieve O2 sat >92%. His chest X-ray was notable for diffuse bilateral pulmonary edema.
Interestingly, the neurologic symptoms seen in acute hyponatremia are due more to hypo-osmolality rather than hyponatremia itself. Low serum osmolality leads to cerebral edema, and in severe cases can result in brain herniation. However, since the irrigating fluids are not pure water, the serum osmolality is usually not as low as might be expected given the degree of hyponatremia. In this case, the patient’s serum osmolality was 268 mOsm/kg; this could explain why he did not exhibit neurologic symptoms despite an extremely low serum sodium of 95 mmol/L. Of note, when glycine is used for irrigation, there may be independent neurotoxic effects related to its metabolites.
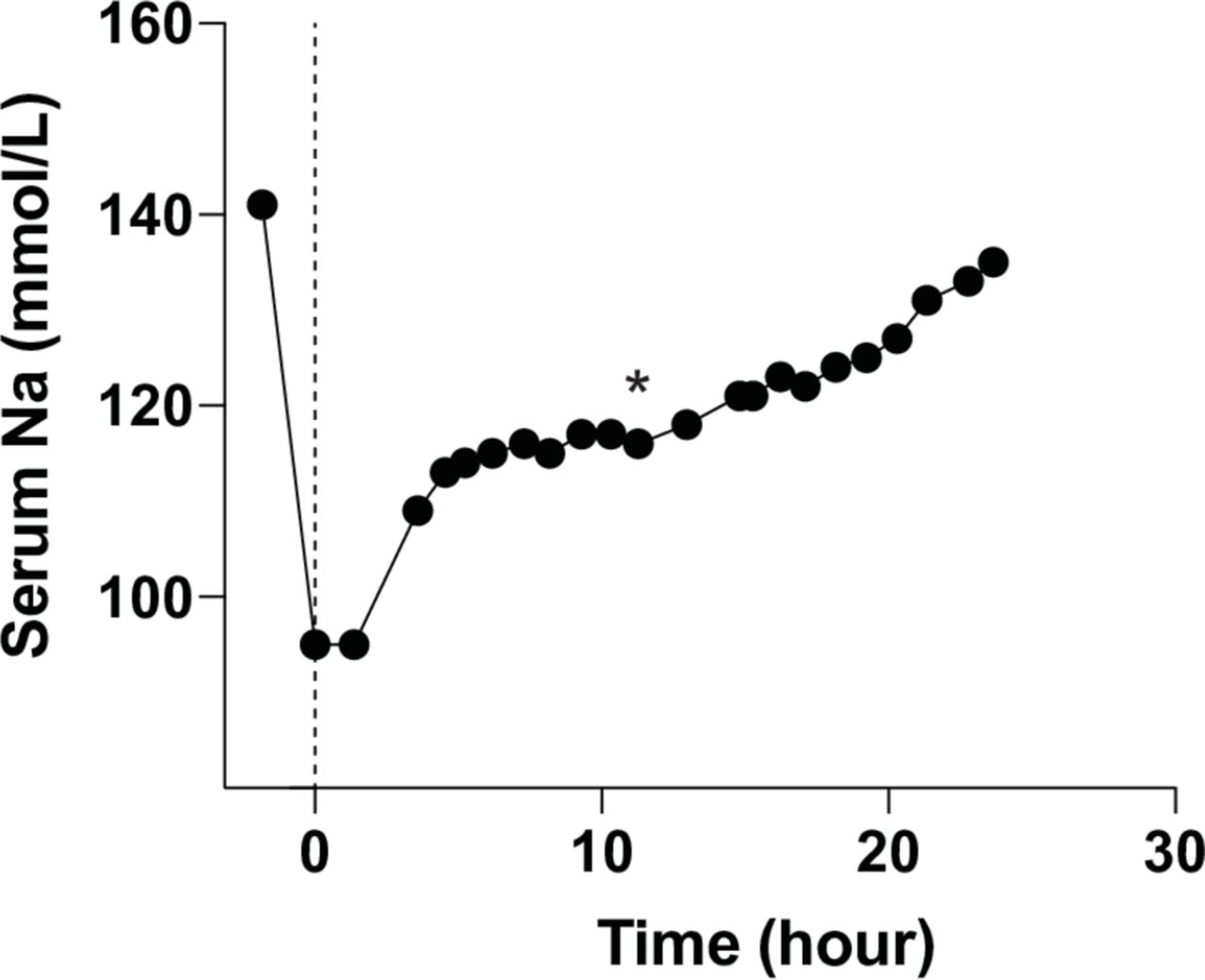
While the treatment of chronic hyponatremia requires a slow increase in serum sodium levels to avoid the feared risk of osmotic demyelination syndrome2, hyponatremia secondary to TURP syndrome is acute. Since the brain has not had time to equilibrate, rapid correction is safe and especially indicated if the patient is exhibiting neurologic symptoms. If the hyponatremia is mild and the patient is asymptomatic, no aggressive intervention other than monitoring may be required. For severe TURP syndrome, 3% hypertonic saline given as a bolus and/or infusion is useful to correct hyponatremia and to counteract the osmotic diuresis caused by glycine, sorbitol, or mannitol, which further draws sodium into the urine. Frequent monitoring in an intensive care unit setting is recommended to assess neurologic changes and ensure the rapid correction of sodium. Other treatment modalities include the administration of loop diuretics if there are any clinical signs of volume overload such as pulmonary edema3,4. Our patient was admitted to the intensive care unit with hourly neurologic monitoring and hourly whole blood sodium checks. He received 20 mg furosemide, with a repeat dose the following morning; he was able to wean from 10 L non-rebreather mask to room air overnight. In addition, he was given two 125 mL boluses of 3% hypertonic saline and was placed on a 3% hypertonic saline infusion overnight, at a rate that was titrated to achieve a slow and steady increase in sodium. Throughout the night, he had intermittent episodes of confusion that were attributed to mild cerebral edema, but never had a depressed mental status. The following morning, his intravenous line was found to have infiltrated, so the rise in sodium was slower than planned (figure 1). Twenty hours later, his sodium was 135 mmol/L (2 mmol/L/hour rise) and he was completely neurologically intact.

{kind=link}
Postoperative trend of the patient’s serum sodium after transurethral resection of the prostate. Time 0 represents time when the patient reached the recovery area. The labs were rechecked to confirm accuracy. The flat part of the curve below the asterisk denotes when the intravenous line infiltrated.
Footnotes
Contributors All three authors have been involved and made significant contributions to the writing of this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.