Article Text

Abstract
Introduction Extracorporeal membrane oxygenation (ECMO) was once thought to be contraindicated in trauma patients, however ECMO is now used in adult patients with post-traumatic acute respiratory distress syndrome (ARDS) and multisystem trauma. Despite acceptance as a therapy for the severely injured adult, there is a paucity of evidence supporting ECMO use in pediatric trauma patients.
Methods An electronic literature search of PubMed, MEDLINE, and the Cochrane Database of Collected Reviews from 1972 to 2018 was performed. Included studies reported on ECMO use after trauma in patients ≤18 years of age and reported outcome data. The Institute of Health Economics quality appraisal tool for case series was used to assess study quality.
Results From 745 studies, four met inclusion criteria, reporting on 58 pediatric trauma patients. The age range was <1–18 years. Overall study quality was poor with only a single article of adequate quality. Twenty-nine percent of patients were cannulated at adult centers, the remaining at pediatric centers. Ninety-one percent were cannulated for ARDS and the remaining for cardiovascular collapse. Overall 60% of patients survived and the survival rate ranged from 50% to 100%. Seventy-seven percent underwent venoarterial cannulation and the remaining underwent veno-venous cannulation.
Conclusion ECMO may be a therapeutic option in critically ill pediatric trauma patients. Consideration should be made for the expansion of ECMO utilization in pediatric trauma patients including its application for pediatric patients at adult trauma centers with ECMO capabilities.
- Extracorporeal
- trauma
- pediatric
- ECMO
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Pediatric trauma has been a relative contraindication to extracorporeal membrane oxygenation (ECMO) due to the high risk for persistent or new bleeding. Despite this, traumatic injuries such as intracranial bleeding, solid organ lacerations, and long bone fractures are no longer considered absolute contraindications to ECMO.1 Several large retrospective studies have supported the efficacy and safety of ECMO in adult trauma patients and it is now accepted as a therapy for the severely injured in certified centers.2 3
Although the use of ECMO in adult trauma has increased, the use of ECMO in pediatric trauma patients is rare. One of the first reports of ECMO use in pediatric trauma patients was a small case series published in 1991.4 Since that time there have been limited retrospective studies in pediatric patients and the largest studies are from administrative databases with little patient-level data.2 5
We performed a systematic review of the literature to describe the collectively reported use of ECMO in the pediatric population and its associated outcomes.
Methods
Data sources and search
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed for our review.6 An electronic literature search of PubMed, MEDLINE, and the Cochrane Database of Collected Reviews from 1972 to 2018 was performed by a trained medical librarian using a combination of keywords and MeSH terms. Our search protocol included identifying articles based on search terms to include: ‘Trauma’, ‘Injury’, ‘Extracorporeal’, ‘Pediatric’, ‘ECMO’ and ‘Cardiopulmonary support’.
Study selection
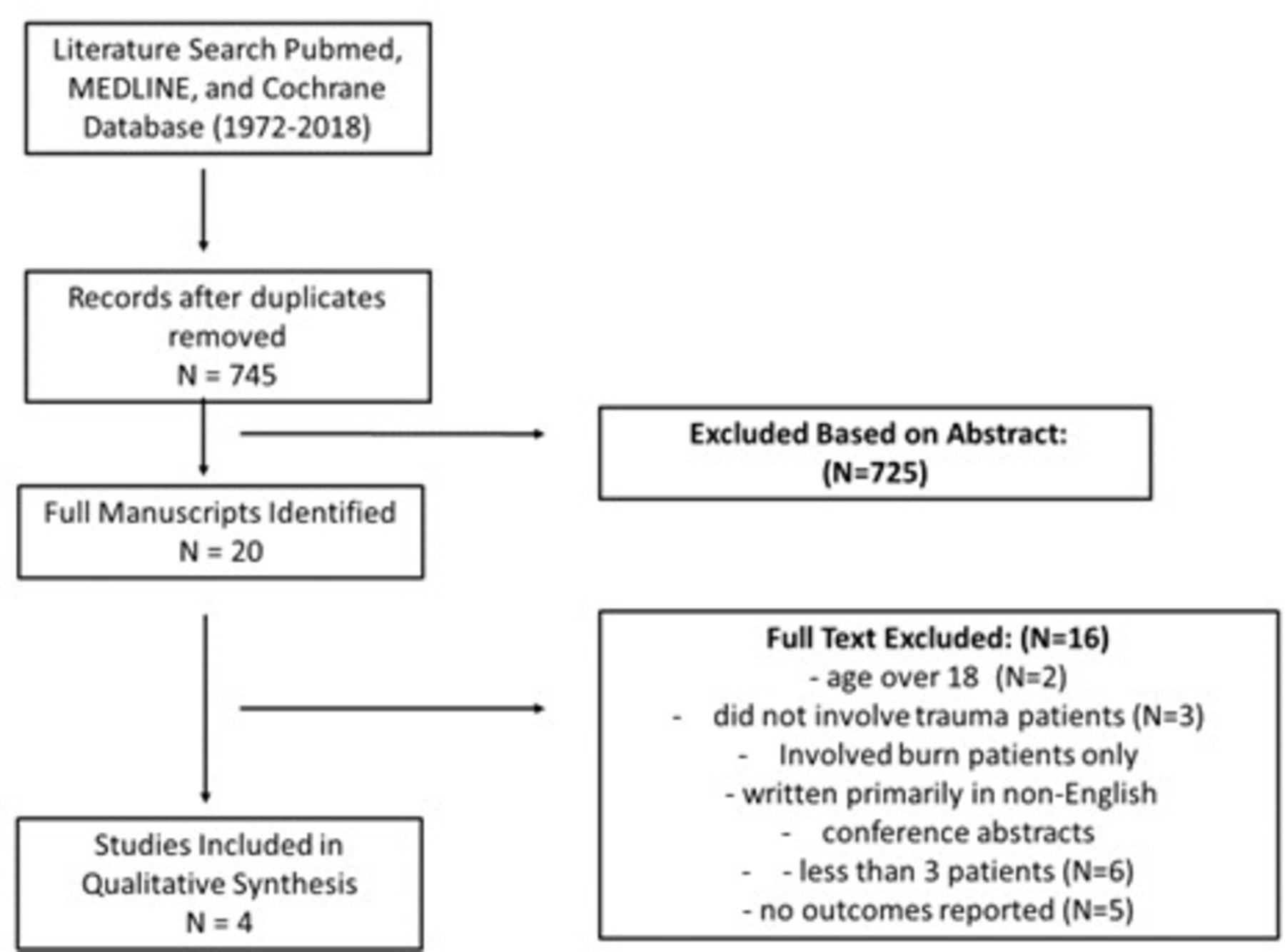
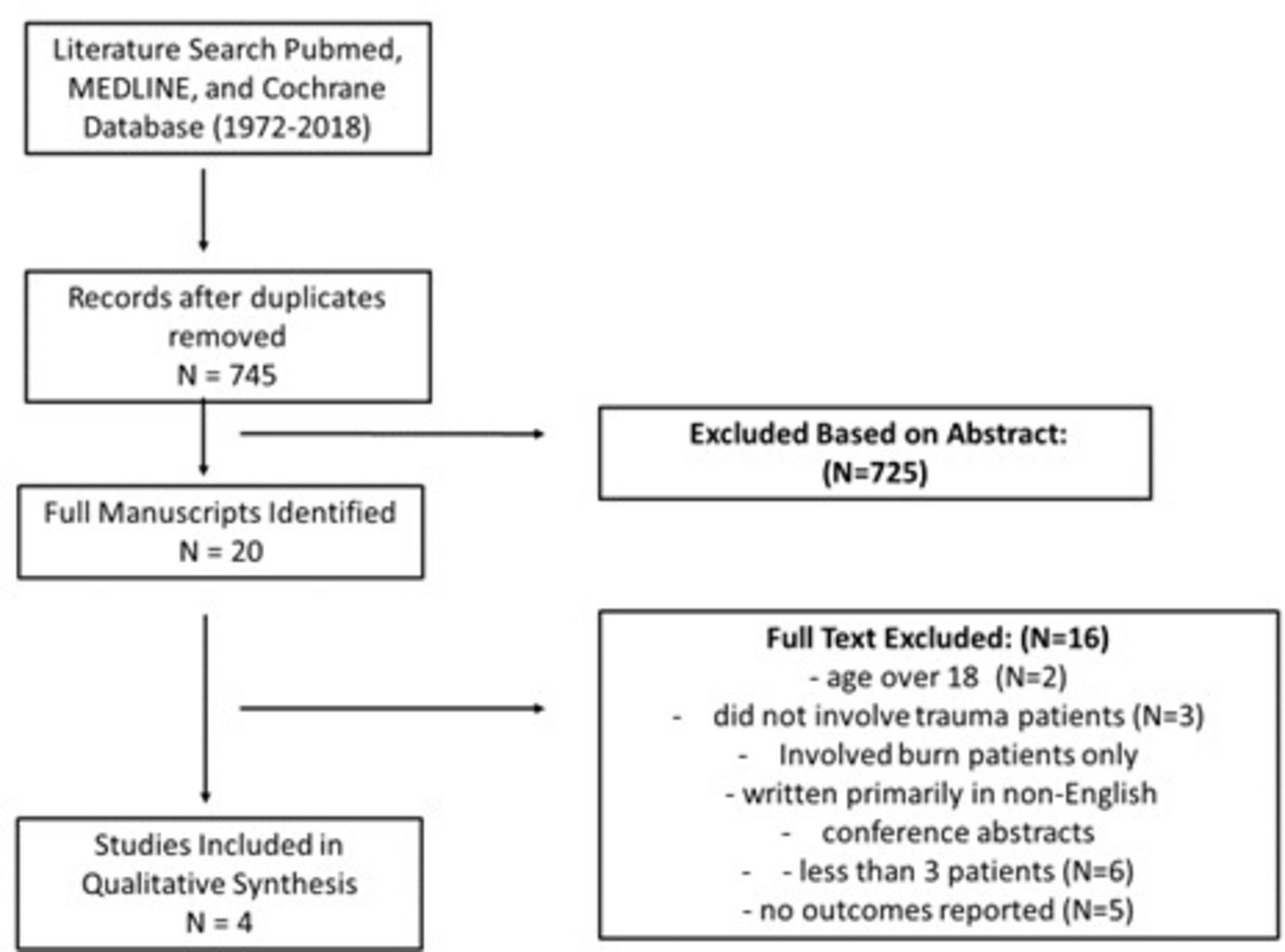
All titles and abstracts were reviewed independently by two reviewers (TP, JG). Articles selected for full review were analyzed by three reviewers (TP, GZ, PM) and consensus used for final inclusion. We included studies meeting the following criteria: patient age less than 18, trauma patients, written primarily in English, not a conference abstract, and reported survival. Studies with less than three patients (case reports) were excluded (figure 1).
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram.
Data extraction and quality assessment
A detailed review of each study was performed and extracted data included study year(s), location, population demographics, types of ECMO (venoarterial (VA), veno-venous (VV)) used and ECMO center characteristics. Finally, we extracted outcome measures including survival and complication rates. A planned meta-analysis was unable to be performed due to the variation in quality of studies and small sample size.
We assessed study quality using the Institute of Health Economics quality appraisal tool for case series.7 Study quality assessment was completed independently by two reviewers (TP and PM) and a third (JG) providing consensus for any disagreements (table 1). Studies with a score of 14 or more were considered of adequate quality.
Study quality
Results
The search returned 745 articles after removal of duplications. Twenty articles underwent full review and four met final inclusion/exclusion criteria (figure 1). All studies were retrospective or cases series in the USA (tables 2 and 3).
Characteristics of studies reporting on pediatric ECMO in trauma
Patient characteristics and outcomes of included studies
The age range of patients was 21 months to 18 years. Fifty percent of patients suffered blunt trauma, 12% suffered penetrating trauma, and 17% suffered from drowning. Twenty-nine percent of patients were cannulated at an adult ECMO center and the remainder were cannulated at a pediatric center.
The type of cannulation was known in 22 patients and 77% underwent VA cannulation. Only two patients were cannulated within 24 hours of injury. Of the 22 patients whose indication for ECMO was reported, 91% were cannulated for acute respiratory distress syndrome (ARDS) and the remaining for cardiovascular collapse. Multiple patients underwent operative exploration in the days prior to cannulation. Several patients had procedures performed while on ECMO including placement of intracranial pressure monitoring devices and open reduction and internal fixation of an extremity fracture. The most commonly reported complication was renal failure reported in eight patients. Bleeding complications were noted in five patients but all were managed without intervention and did not lead to death.
Overall 60% of patients survived and the survival rate ranged from 50% to 100% in each study. In the largest study, 47.6% of survivors (10 of 21) were discharged directly to home.5 In the remaining studies, 14 of 22 patients survived and all were noted to have excellent neurologic recovery and returned to baseline functional capacity.1 4 8
Overall study quality was poor with only a single article of adequate quality (table 1).
Discussion
The use of ECMO after pediatric trauma is not well described. We identified four studies that reported the use of ECMO in 58 patients. The most commonly reported cannulation was VA ECMO and generally occurred greater than 24 hours after injury. Overall survival was 60%, ranging from 50% to 100%. Bleeding complications were reported in 5 of 58 patients (8.6%) but none led to mortality.
The earliest report of ECMO in the neonatal population occurred in 1975 for respiratory failure after meconium aspiration.9 Since that time the technology has improved and indications have expanded.10 ECMO use in trauma patients dates back to 1971 when Hill et al used this technology in an adult patient with ARDS after a motor vehicle collision.11 The first case of ECMO utilization in a pediatric trauma patient was not described for nearly 20 years until 1991 by Steiner et al.4 Since that time there have been limited data regarding ECMO use in pediatric trauma patients.
Traumatic brain injury (TBI) and intracranial bleeding were once considered absolute contraindications to ECMO and were reasons once cited for limited use in trauma.12 In the last decade this dogma has been challenged in adult studies and has in part been driven by newer technology with improved pumps and heparin-coated lines allowing for reductions in anticoagulation.13 Several case series have described ECMO use in adult trauma patients with TBI and in extreme cases post-traumatic craniectomies have been performed while on ECMO.14 15 There has also been increasing support for heparin-free and anticoagulation-free ECMO circuits.15 16 TBI also appears to not be a definitive contraindication to ECMO in pediatric patients. In the largest study of pediatric trauma patients treated with ECMO by Watson et al there was 83% survival after head injuries with Glasgow Coma Scale score ≤8% and 55% survival for patients with major head injury.5 Additionally, survival was seen in multiple other studies which included pediatric patients with head injuries.1 8
In addition to post-traumatic ARDS, ECMO has proven useful for pediatric patients with severe multisystem traumatic injuries and cardiovascular collapse. Skarda et al described two patients with intracranial pressure monitoring devices for head injuries placed while on ECMO. Additionally, two patients had intra-abdominal injuries including a duodenal hematoma and grade II splenic laceration which did not preclude cannulation within 24 hours of injury. All patients in this small series had good outcomes including neurologic recovery evaluated after a 2-year interval.1
Another factor that may limit ECMO utilization in the trauma population is the need for emergent surgical procedures. Given the need for anticoagulation while on ECMO this may increase the hemorrhage risk of such procedures, but several adult studies indicate that interventions such as exploratory laparotomies, exploratory thoracotomies, orthopedic procedures, percutaneous tracheostomy placement, and even damage control operations have been performed while on ECMO.15 17–19 Additionally, several studies included pediatric patients who underwent emergent operations just prior to cannulation and one patient with open reduction internal fixation applied while on ECMO.1 4 8
Based on the most recent data from Pediatric National Trauma Database, there are 30 level 1 pediatric trauma centers and six level 2 pediatric trauma centers in the USA.20 Forty-one percent of these are associated with a pediatric hospital. Most pediatric ECMO cannulations occurred at pediatric trauma centers, but in the largest study of pediatric trauma patients, 47% of patients (15 of 36) were cannulated for ECMO at adult ECMO centers.5 This would suggest that adult trauma centers with ECMO capabilities should consider pediatric cannulation as a potential therapy for severely injured pediatric trauma patients.
An additional potential benefit of ECMO identified in our review is for preserved quality of life. Traditionally, most trauma literature evaluates outcomes in terms of mortality, but our data indicate that in addition to a survival benefit, pediatric trauma patients who survive with ECMO can have very little sequela. In the largest study of pediatric trauma patients who underwent ECMO, 47.6% of survivors (10 of 21) were discharged directly to home.5 In the remaining studies, 14 of 22 patients survived and all were noted to have excellent neurologic recovery and returned to baseline functional capacity.1 4 8
The extracorporeal life support organization (ELSO) registry10 is an international registry for ECMO centers and based on their most recent data, overall survival after ECMO for respiratory indications in the pediatric population is 58% and for cardiac indications the survival is 52%. In the adult population, survival after ECMO for respiratory indications is 59% and 42% for cardiac indications.21 In our review we found that overall 60% of pediatric trauma patients placed on ECMO survived and the survival rate ranged from 50% to 100% in each study. This is similar to the 50% to 79% survival seen in a review on the adult trauma population.22
Limitations
The major limitation of this review is the number and quality of the studies available for qualitative analysis. Our review was limited to retrospective data and the majority of studies were small case series, some with incomplete data. Specifically, the available data regarding anticoagulation management in this population are sparse, and the Injury Severity Score was not available to compare similarly injured patients or better define the role of injury severity in ECMO survival and associated complications. Without a comparison (ie, No ECMO) it is hard to determine if the use of ECMO was the factor which led to patient survival. Additionally, the preferred type of ECMO is potentially skewed as VV ECMO in pediatric was rare during study period of largest series.5 There were no prospective studies identified and the limited quality of studies precluded formal meta-analysis. Restricting to English-only articles may have contributed to our limited number of studies, but this allowed us to analyze practices applicable to US centers. There is a need for a study of pediatric patients in the international ELSO registry. The risk of reporting and publication bias was inherent in all included studies and is especially a concern in regard to complications.
Conclusion
Our systematic review illustrates the paucity of data regarding ECMO in pediatric trauma patients but the available literature suggests that ECMO may be a therapeutic option for the most critically ill in this population. As seen in adults, head injuries and intra-abdominal injuries do not seem to be absolute contraindications to pediatric ECMO which suggests more patients could potentially benefit from this therapy. Additionally, ECMO should not be limited to post-traumatic ARDS and there may be role for ECMO in multisystem pediatric trauma patients with cardiovascular collapse. Consideration should be taken for the establishment of a trauma ECMO registry which could help better determine indications for utilization in this population.
References
Footnotes
Twitter @@pbatesmurphy
Contributors TP, PM, JG and JLH contributed to the study conception and design, acquisition of data, analysis and interpretation of data, drafting of article and critical revision. BAC and MP contributed to analysis and interpretation of data and critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.