Article Text

Statistics from Altmetric.com
A 60-year-old man presented to our clinic with a 5-year history of severe, chronic chest pain. His symptoms began in September 2013 when he had a prolonged upper respiratory illness and persistent cough. After 2 weeks of coughing, he awoke one morning with severe left-sided chest pain and a large bruise over his left chest wall. He presented to his local hospital, where he was found to have a displaced left sixth rib fracture and a large left hemothorax, eventually requiring video-assisted thoracoscopic surgical (VATS) evacuation. After recovering from his acute illness, he developed chronic left chest wall pain and persistent clicking and popping of his costal margin. Along with the pain, he developed symptoms of depression and post-traumatic stress to a point at which he lost his business and had considered suicide.
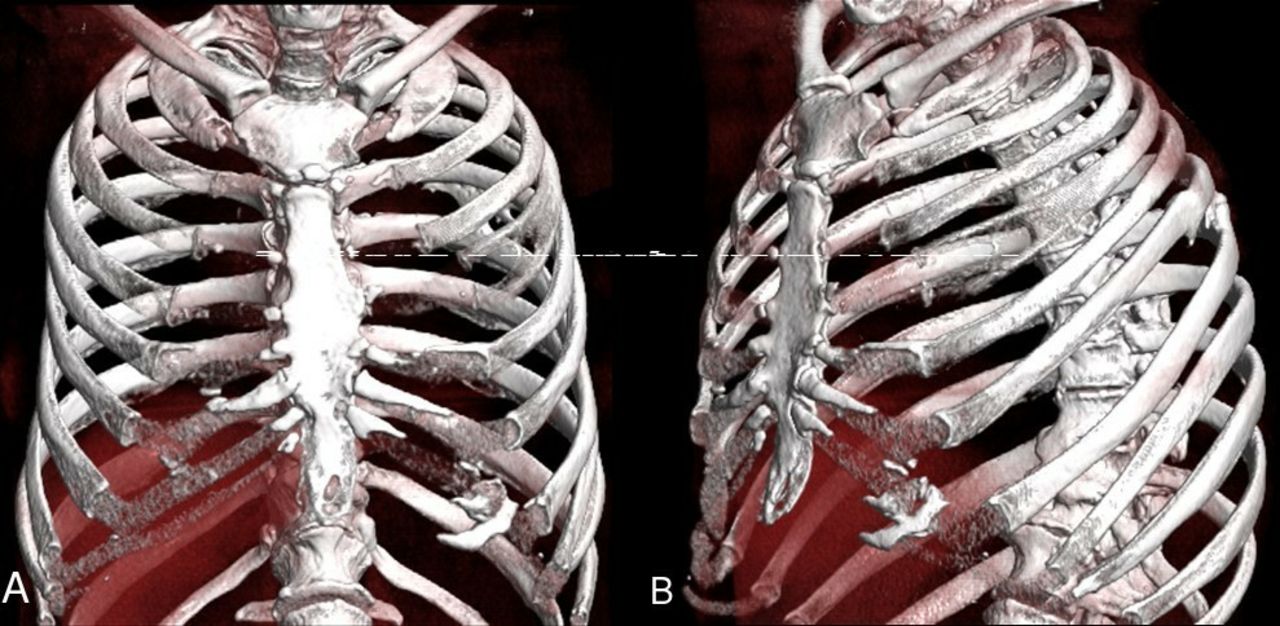
On physical examination, he had normal vital signs and a body mass index of 28.3 kg/m2. He had two scars on his left chest from his VATS. His left chest wall was severely tender to palpation from the midaxillary line to the sternum. He had marked, palpable instability of his costal margin on deep inspiration. He had no pain or tenderness on the right side of his chest, and the remainder of the examination was unremarkable. A CT scan of the chest demonstrated a healed fracture deformity of the left fifth rib laterally. Small near-bridging synostosis of the left posterior sixth and seventh ribs and mild gapping of the left sixth and seventh ribs laterally with no costochondral joint dislocation were identified. Reconstructions were performed on his chest CT and representative images are shown in figure 1.

Preoperative CT scan, three-dimensional reconstructions: (A) anterior view and (B) left anterolateral view.
What would you do?
Pain management consultation.
Psychiatry referral.
Chest wall reconstruction.
What we did and why
The patient was booked for chest wall reconstruction, resection of the pseudarthrosis formation at his costal margin rupture, and stabilization of his anterior chest wall. After informed consent, epidural placement, and induction of general anesthesia, the anterior chest was prepped and draped in its entirety. An incision was carried along his left costal margin extending onto his sternum. The left anterior costal margin was encased in a large pseudarthrosis which was opened and resected. The costal cartilages had been ruptured and these were debrided to healthy tissue. After adequate debridement, we identified a small gap between segments of approximately 0.5 cm, and a decision was made to fixate the costal margin using a single 30-hole titanium plate (DePuy Synthes, Westchester, PA). This was hand-bent to recreate the three-dimensional shape of his native costal margin and was fixed to the ninth rib laterally using titanium screws. At the area of rupture and gap, we secured the plate to the underlying cartilage using three zip-ties made of polyetheretherketone (DePuy Synthes). Additional titanium screws were placed in the cartilage to maximize stability. Finally, the titanium plate was secured to the sternum using titanium screws. This overall led to an extremely stable and secured chest wall reconstruction with an excellent synchronous movement with deep positive pressure inspiration. Figure 2 shows his intraoperative anatomy. The wound was irrigated and closed. A 19-French Jackson Pratt drain was left in the subcutaneous space. The estimated blood loss was 50 mL.

Intraoperative anatomy after fixation.
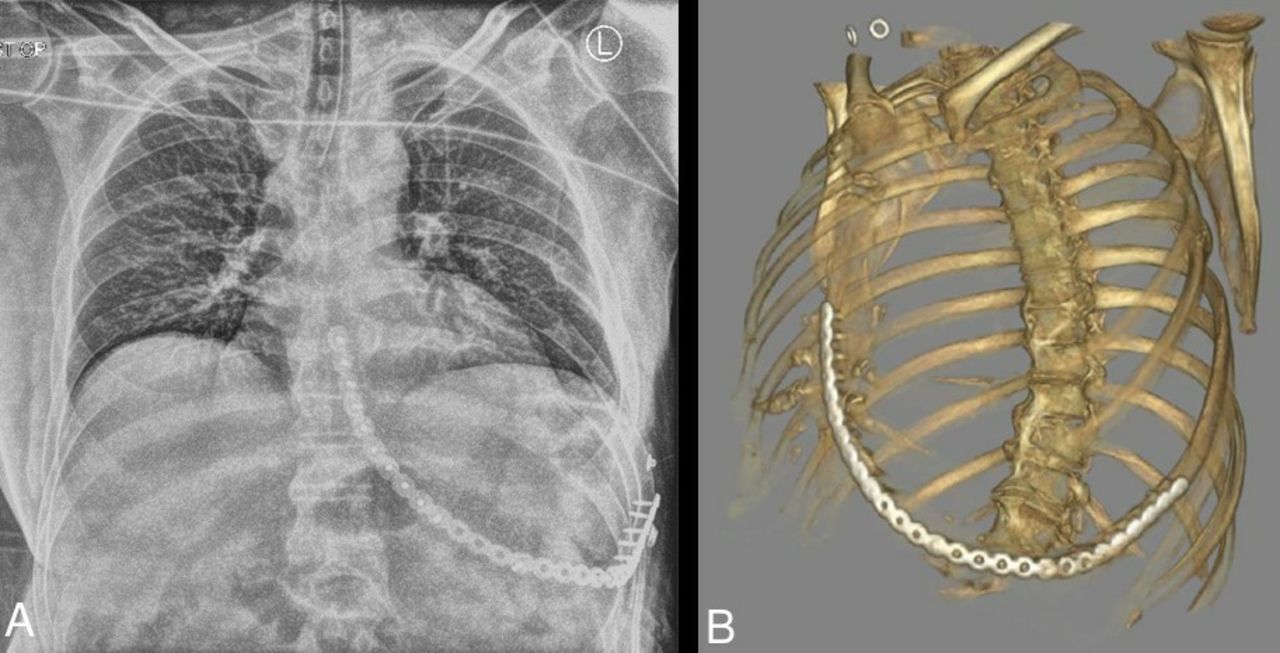
The patient had an uncomplicated recovery and was discharged home on postoperative day 3. A postoperative chest X-ray is shown in figure 3. He was seen in the office 2 weeks postoperatively and was doing very well. He reported that his pain had improved greatly, although he still had occasional pain with rotation of his torso and lateral bending. He was no longer requiring narcotics for pain. His drain output was minimal and the drain was removed.

{kind=link}
{kind=link}
{kind=link}
Postoperative chest imaging: (A) postoperative chest X-ray and (B) postoperative CT scan, three-dimensional reconstruction.
Rib fractures are common after blunt trauma, affecting approximately 10% of patients.1 The mainstay of treatment is pain control and pulmonary support, with operative fixation remaining relatively rare. Recent years have seen a resurgence in clinical and research interest in surgical stabilization of rib fractures after trauma. Use of rib fixation increased by 76% from 2007 to 2014.2 The clearest indication is in cases of flail chest. Multiple randomized controlled trials and meta-analyses have found benefit with rib fixation for flail chest in terms of reductions in ventilator days, tracheostomy, intensive care unit length of stay, pneumonia, and pain. 3–6 There may also be benefit in patients with severe, displaced rib fractures without flail physiology.4
Indications for chest wall reconstruction in chronic unstable chest walls such as that seen here are less clear, with only anecdotal reports in the literature indicating improved pain with rib fixation. Recent consensus guidelines suggest operative repair of chronic nonunion for “persistent disabling pain,” as a level 3, grade B recommendation.5
Patients with poorly healed rib fractures are at risk of chronic pain, as their symptoms are exacerbated with each breath they take. Our experience, including with this patient, suggests that surgical stabilization may be of great benefit to this population, reducing symptoms, improving function, and reducing dependence on narcotics.
Footnotes
Contributors EK drafted the article. AS critically reviewed the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AS is a consultant and speaker for DePuy Synthes, and consults for KLS Martin Group and Globus Medical.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.