Article Text

Abstract
Case Presentation A 38-year-old man was brought in by ambulance as a trauma activation after sustaining a self-inflicted stab wound in the left upper quadrant with a kitchen knife. His primary survey was unremarkable and his vital signs were normal. Secondary survey revealed a 2 cm transverse stab wound inferior and medial to the left nipple. Extended focused assessment with sonography for trauma (FAST) did not show intra-abdominal or pericardial fluid and chest X-ray did not show a definite pneumothorax or hemothorax.
What would you do?
Wound exploration at bedside.
Admit for observation and serial examinations.
Exploratory laparotomy and open repair of traumatic diaphragmatic injury (TDI).
Thoracotomy and open repair of TDI.
Diagnostic laparoscopy and laparoscopic repair of TDI.
- diaphragm
- surgical technique
- trauma laparoscopy
- penetrating trauma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What we did and why
Answer: E
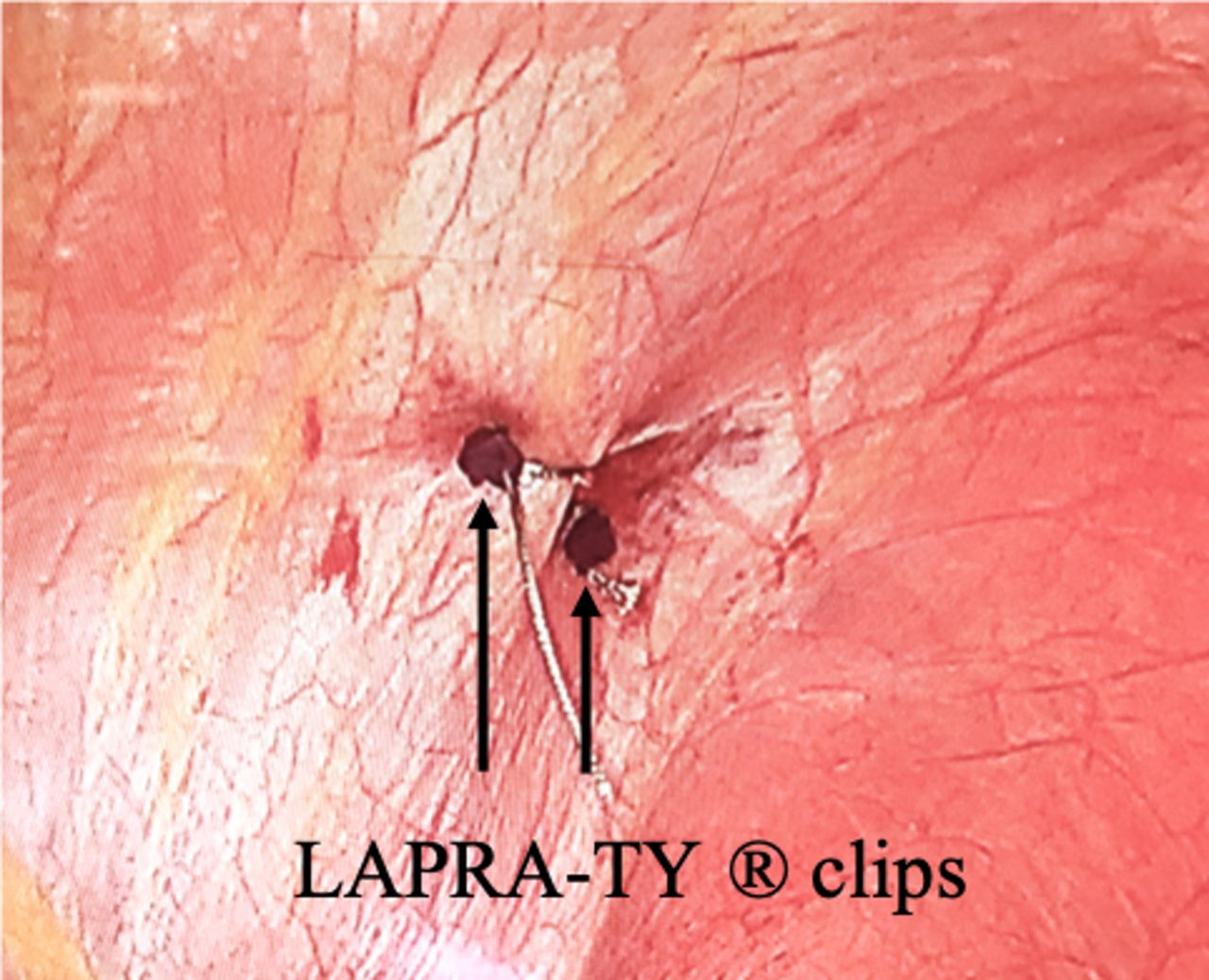
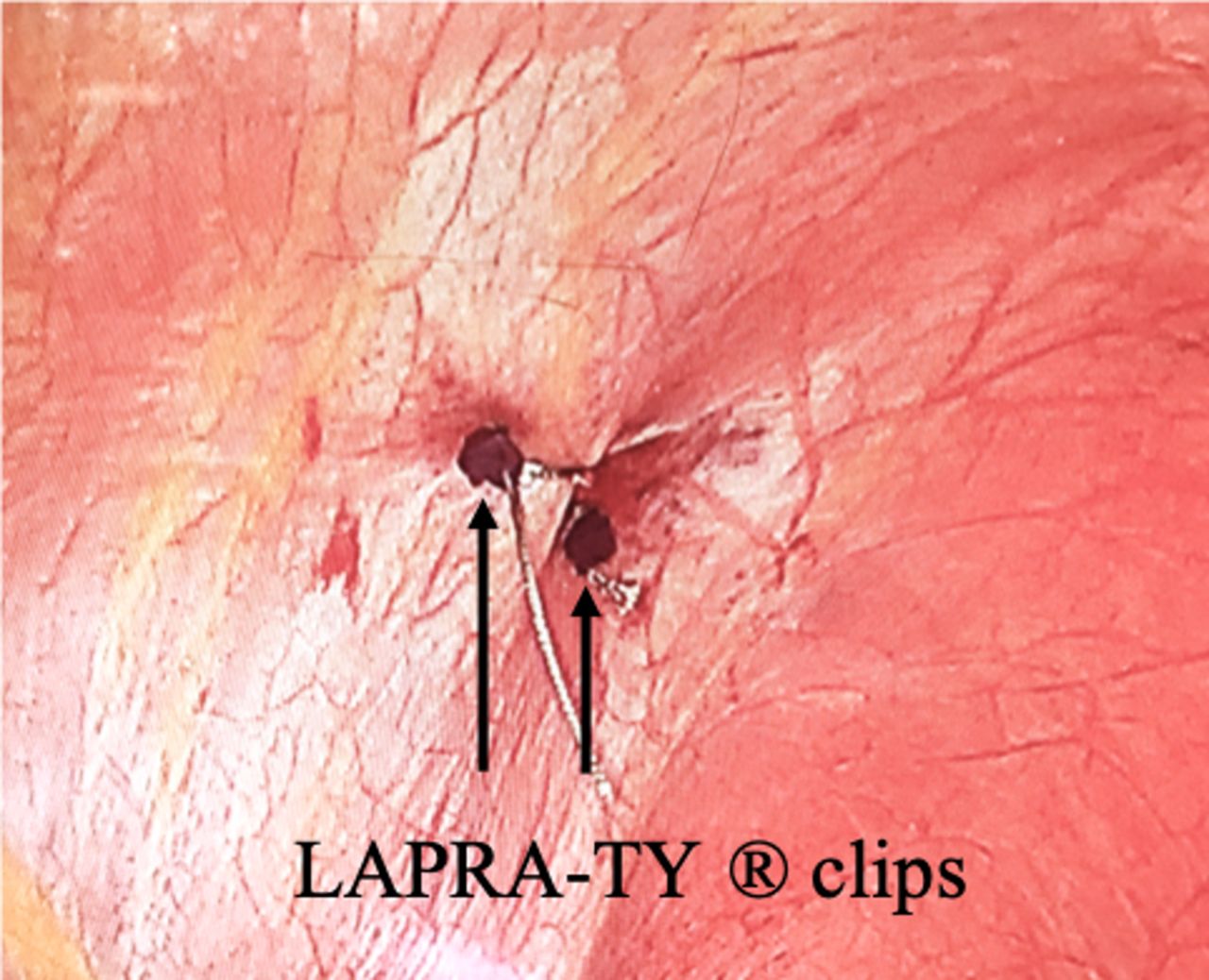
Given this penetrating injury in the left thoracoabdomen, the patient was taken to the operating room for diagnostic laparoscopy to rule out a TDI. We identified a 1.5 cm diaphragmatic injury (figure 1) and proceeded with primary repair using 0-Ethibond suture in a figure-of-eight fashion, secured with two LAPRA-TYs (figure 2). We ran the entire length of the small bowel from the Ligament of Treitz to the cecum and examined the entire stomach up to the gastroesophageal junction; no additional intra-abdominal injuries were identified. The patient had an unremarkable postoperative course and was discharged on postoperative day 3.

Traumatic penetrating diaphragmatic injury to the left hemidiaphragm with a 1.5 cm defect.
{kind=link}
{kind=link}
Postrepair of TDI with figure-of-eight 0-Ethibond suture, secured with two LAPRA-TY clips.
TDI is a relatively uncommon diagnosis, although the true prevalence is difficult to estimate because some patients present more than a decade after injury . However, missed TDIs can result in devastating consequences, such as incarceration of herniated viscus. A retrospective review of 45 patients with diaphragmatic hernias from TDI reported 25% mortality for those who re-presented late after their initial trauma admission.1
Thoracoabdominal injuries span five visceral compartments and can be accessed through the chest or the abdomen. Given the location of the patient’s injury, we had a high clinical suspicion to rule out TDI. In fact, one study showed that 36% of patients with a penetrating thoracoabdominal injury and normal chest X-ray were eventually found to have diaphragmatic injury.2 We had considered a thoracoscopic approach to evaluate for TDI. However, with a negative extended FAST and unremarkable chest X-ray, we had less suspicion for concomitant cardiac or pulmonary injury. Thoracoscopic approach would have limited our evaluation of the abdomen. Therefore, we proceeded with a diagnostic laparoscopy to rule out TDI and bowel injury.
Once we identified the 1.5 cm left TDI, we proceeded with primary laparoscopic repair using LAPRA-TY. LAPRA-TY (Ethicon Endosurgery, Cincinnati, Ohio, USA) was developed as a technically less demanding alternative to intracorporeal knot tying; securing sutures only requires placement of two clips. LAPRA-TY has been used in laparoscopic radical prostatectomy3 4 and Roux-en-Y gastrojejunostomy.5 Although trauma surgeons’ familiarity with laparoscopic TDI repair has not been studied, lack of familiarity with intracorporeal knot tying may be a barrier to proceeding with laparoscopic repair, especially in a challenging location such as the dome of the diaphragm. Indeed, a review of 454 patients with TDI from 1996 to 2011 showed that less than 2% of repairs were performed laparoscopically.6 LAPRA-TY facilitates efficient TDI repair with basic laparoscopic skills and lowers the barrier of a technically challenging laparoscopic repair.
Footnotes
Contributors JC and JP contributed equally to the work; drafted, wrote and revised the work. JP, JF, DS and TB were involved in the use of the technique during the surgery. JF, DS and TB contributed to final revisions of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.