Article Text

Statistics from Altmetric.com
Introduction
Penetrating neck trauma is common in adults but is rare in the pediatric population. Reports on penetrating neck trauma in the pediatric population is sparse. We describe the case of a 9-year-old boy presenting with a pencil penetrating the neck, discuss management, and review the literature.
Case presentation
A 9-year-old boy with no medical history presented to the trauma bay by emergency medical services (EMS) approximately 45 min after falling onto a Number 2 (No. 2) pencil which penetrated the left preauricular space. The pencil was stabilized with gauze and tape by EMS prior to arrival. In the trauma bay, the patient denied loss of consciousness, profuse bleeding, headache, dizziness, lightheadedness.
Physical examination
Vital signs were stable. The patient was lying supine in an EMS stretcher with the dull end of a No. 2 pencil protruding from the left preauricular space, pointing caudally and posteriorly. Pencil was stabilized in gauze and tape. No active bleeding was present. Patient was awake, alert, and oriented. The patient had full range of motion of the mandible.
Workup and treatment
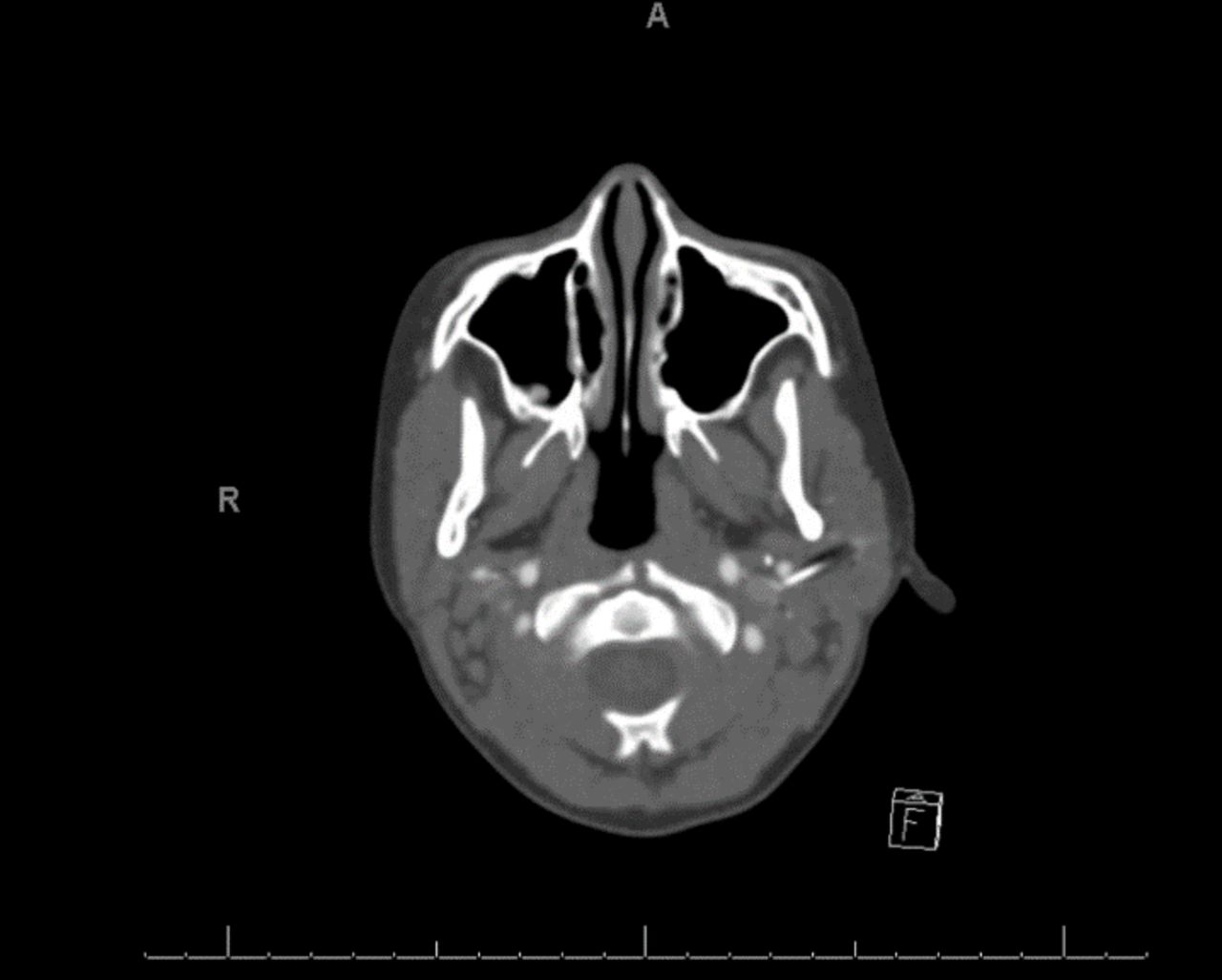
Initial evaluation was performed with CT without contrast (figure 1). On poor visualization of the associated vasculature within the carotid sheath, a CT with contrast was performed. The radiologist reported no rupture of the blood vessels (figure 2).

The initial CT without contrast was performed and showed the hyperdense graphite possibly compromising vascular structures within the neck.

{kind=link}
{kind=link}
The subsequent CT with contrast was then performed, which showed the hyperdense graphite, with point touching the internal jugular vein and abutting the external carotid artery, but without evidence of vascular rupture.
The patient was subsequently taken to the operating room. The child was placed under generalized anesthesia with appropriate preparation in the supine position. Gauze and tape were removed, and the pencil was visualized pulsating at its location (online supplementary video 1). Pencil was grasped and removed. Wound was packed, sterile dressing placed. The patient’s postoperative course was uneventful. He was discharged 2 days later. At 2 weeks follow-up, the patient was in good health and wound site was healing appropriately with mild scarring.
Supplementary video
Discussion
Penetrating neck traumas have been studied extensively in adults but are under-reported in the pediatric population. In fact, only one pediatric cervical zone 2 penetrating trauma was found when reviewing the literature.1 A study in 2016 using the National Trauma Data Bank found that pediatric penetrating neck trauma has an incidence of 0.28%.2 This makes studying pediatric neck trauma difficult. Much is adopted from adult experiences.3
Currently, there are two diagnostic approaches used to assess the need for surgical intervention in penetrating neck trauma: zone-based approach and no-zone approach. The zone-based approach is an older approach, which decides management strategy based on zone, whereas the newer no-zone approach uses CT angiography after the patient’s hemodynamic stability is determined.
More recent literature indicates that the no-zone approach can adequately identify aerodigestive and vascular injuries in penetrating neck wounds, although avoiding invasive diagnostic procedures used in the zone-based approach.4 5 Additionally, in favor of the no-zone approach, there have been reports of a 100% sensitivity and 95% specificity for CT angiogram in adults with zone 2 penetrating traumas; however, these cases had direct zone 2 penetration.6
Against the favor of the zone-based approach, penetrating neck traumas externally entering a specific zone of the neck are not confined internally to that same zone. Low et al found that there was a high incidence of non-correlation between the location of the external injury and damaged internal structures.7 Case in point, our case describes a zone 3 penetrating trauma that, due to the directionality of the penetration, almost compromised zone 2 structures (internal jugular vein, carotid artery, vertebral artery, esophagus, larynx, trachea, thyroid, thoracic duct, and major cervical nerves).8
We used the no-zone approach to assess our patient. We assessed for any vascular or aerodigestive injury that required surgical intervention. Hall et al described seven indications for immediate surgical exploration, which include expanding hematomas, significant bleeding or signs of shock, subcutaneous emphysema, bruit, thrill, crepitus, or dysphagia.9 If these signs are not evident, the literature recommends confirmatory imaging to rule out major structural compromise. On performing the CT without contrast, there was recommendation for an immediate CT angiogram due to the proximity to vital structures within the carotid sheath. This sequence demonstrates the importance of considering zone 2 structures, even in a zone 3 penetration, if directionality and mechanism of the penetrating injury make this transition possible. As such, we recommend immediate performance of a CT angiogram when there is a possible extension of injury to zone 2 structures.
Also, of note, this case provides useful information about the visibility of a Number 2 pencil on CT scans. The detail of the graphite within the pencil has a hyperdense quality that is distinguishable from neighboring soft tissue. However, the wood in the pencil was poorly visualized. This is congruent with the results found from a large animal foreign body imaging study in 2010.10
Conclusion
Penetrating trauma to the neck is an uncommon emergency in the pediatric population. Penetrating neck trauma due to a pencil is exceedingly rare. Rapid identification, proper workup and subsequent removal in the operating room can prevent significant blood loss, disfigurement, or death.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Footnotes
Contributors RB is the primary author of the case report. AM, ASI and RM are co-authors in the report. RM is the faculty advisor for the report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.