Article Text

Abstract
Background Misplacement of enteral feeding tubes (EFT) in the lungs is a serious and potentially fatal event. A recent Food and Drug Administration Patient Safety Alert emphasized the need for improved technology for the safe and effective delivery of EFTs.
Objective We investigated the feasibility and safety of ENvue, a novel electromagnetic tracking system (EMTS) to aid qualified operators in the placement of EFT.
Methods This is a prospective, single-arm study of patients in intensive care units at two US hospitals who required EFTs. The primary outcome was appropriate placement of EFTs without occurrence of guidance-related adverse events (AEs), as confirmed by both EMTS and radiography. Secondary outcomes were reconfirmation of the EFT tip location at a follow-up visit using the EMTS compared with radiography, tube retrograde migration from initial location and AEs.
Results Sixty-five patients were included in the intent-to-treat analysis. EFTs were successfully placed in 57 patients. In eight patients, placement was unsuccessful due to anatomic abnormalities. According to both the EMTS and radiography, no lung placements occurred. No pneumothoraces were reported, nor any guidance-related AEs. Precise agreement of tube tip location was achieved between the EMTS evaluations and radiographs for 56 of the 58 (96.5%) successful placements (one patient had two placements). Tube tip location was re-confirmed 12–49 hours after EFT insertion by the EMTS and radiographs in 48 patients (84%). For 43/48 patients (89.5%), full agreement between the EMTS and radiography evaluations was observed. For the five remaining patients, the misalignment between the evaluations was within the gastrointestinal tract. Retrograde migration from the initial location was observed in 4/49 patients (8%).
Conclusion A novel electromagnetic system demonstrated feasibility and safety of real-time and follow-up tracking of EFT placement into the stomach and small intestine, as confirmed by radiographs. No inadvertent placements into the lungs were documented.
Level of evidence Level V (large case series).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Enteral nutrition (EN) is generally the preferred route of nutritional support in critically ill patients with a functional gastrointestinal (GI) tract. In addition to the effective delivery of nutrients, the multiple benefits of EN include preservation of gut mucosa integrity, reductions in infectious complications and enhanced GI motility and immune responses.1 A systematic review and meta-analysis of 18 randomized controlled trials (RCTs) concluded that EN compared with parenteral nutrition decreases infectious complications and length of stay in intensive care units.2 Enteral nutrition is also associated with significant cost saving.3 Postpyloric feeding tube placement has been shown to reduce the risk of ventilator-associated pneumonia and may improve nutritional delivery by overcoming decreased gastric motility.4–7 However, due to technical difficulties, attempts to insert tubes into the postpyloric region may delay feeding, and ultimately gastric placement may have to be accepted.8–10 Approximately 6.7 million feeding tubes are placed blindly each year in the USA.11 While blind insertion of nasogastric tubes has generally been considered safe, severe and even fatal complications have been reported.12–14 In patients undergoing small-bore feeding tube procedures, respiratory misplacement was reported in 3.2% of placements with 39% of them resulting in pneumothorax.15 Of 9931 blindly inserted nasoenteric tubes inserted in five studies, 1.9% were placed in the tracheobronchial tree; of the 187 tube misplacements, pneumothoraces occurred in 35 (18.7%), at least 5 of which were fatal.16 Other studies have reported airway tube misplacements of up to 15% and pneumothorax events of up to 60% due to feeding tube placement.17–21 Adverse outcomes following blind insertions may be more common than has been acknowledged; recently published clinical and autopsy data demonstrate that some deaths assumed to be caused by underlying disease are apparently due to fatal problems with blind insertions.22
Various adjuvant techniques are currently in use for confirmation of placement of small-bore feeding tubes. These mainly comprise radiography23 and electromagnetic (EM) technology, the latter enabling real-time visualization of feeding tube placement. Initial studies suggested that the commercially available EM Placement Device, the Cortrak Enteral Access System, (Avanos Medical, Alpharetta, Georgia, USA), could reduce the need for radiographic confirmation.24–28 However, a substantial proportion of misplacements have been documented using this system, including undetected lung misplacements, some of them fatal.18 29–31 In January 2018, the Food and Drug Administration (FDA) issued a Safety Alert regarding pneumothoraces associated with inadvertent lung placements of feeding tubes using the Cortrak Enteral Access System.32 This Patient Safety Alert emphasizes the need for improved technology for safe and effective delivery of enteral feeding tubes. This is the first feasibility study of a novel EM tracking system (EMTS), the ENvue system (ENvizion Medical, Tel-Aviv, Israel). The EMTS is designed to aid qualified operators in the placement and tracking of feeding tubes into the stomach or small intestine of adult patients, using an approach that is not affected by patient movement and less prone to operator misplacement. This study aimed to determine the feasibility and safety of this novel EMTS during bedside placement of small-bore enteral feeding tube (EFT).
Materials and methods
Study design
This prospective, single-arm study was conducted in the intensive care units of two institutions in the USA: the Cleveland Clinic Foundation (CCF), Cleveland, Ohio and St. Vincent Indianapolis Hospital and Health Care Center (St. Vincent), Indianapolis, Indiana. Patients who met study eligibility criteria were enrolled during December 2017–March 2018 at CCF, and during April 2018–August 2018 at St. Vincent. Written informed consent was obtained from the patients or their legal authorized representative prior to study participation.
The placement team at CCF consisted of 3 nurses and 2 physicians; and at St. Vincent, 10 nurses. All clinicians involved in this study were previously trained in the placement of small-bore feeding tubes as per institution requirements.
All clinicians received formal training on the EMTS by a company representative. A dedicated session consisted of an overview of the system components and EFT, system set-up and EMTS image interpretation. Training also included a return demonstration of proper procedure on a mannequin with airway and GI structures that enabled visualization of airway misplacement and correct gastric and postpyloric placement. Each nurse completed one to two demonstrations to ensure competency operating the system. Moreover, a representative of the company was present to observe each placement and to ensure safety and proper use.
Patient selection
Study inclusion criteria were age 21 years or above, requiring placement of an EFT; who either had an endotracheal tube (ETT), or did not have an ETT but were sedated (Richmond Agitation-Sedation Scale of −2 or less) or obtunded (Glasgow Coma Scale (GCS) of 9–12). Eligibility for participation in the study also included the ability of the patient or legally authorized representative to understand and adhere to all protocol procedures and to provide written informed consent.
Exclusion criteria included a history of esophageal varices or ulcers, upper GI stenosis or obstruction, upper airway obstruction, trauma involving the sinuses, the nares, the face or the neck that would preclude EFT insertion in the oral or nasal route, deformities of the sinus cavities or skull base, esophageal cancer or neoplasm, a significant concomitant illness that would adversely affect participation and pregnancy or lactation.
Electromagnetic tracking system
All EFTs were placed with the aid of the EMTS. The system is composed of a dedicated mobile cart and is equipped with a battery-operated all-in-one computer. The computer runs the software, which controls the EMTS. The system uses a field generator and several EM sensors, which enable proper scaling of the display to the patient’s body contour. The EFT was designed to operate specifically with the EMTS. The EFT contains an EM sensor incorporated into its distal tip, enabling continuous position confirmation, and creating a path on the monitor. The EMTS field generator produces a series of varying magnetic fields that create a known sensing volume of varying magnetic flux. The position and orientation of the distal tip of the EFT is tracked by the EMTS and the system displays the placement pathway. This pathway is shown on the monitor in three views: frontal, lateral and axial, to allow for a more accurate three-dimensional interpretation of placement. The frontal view represents the tube tracing looking towards the patient. The lateral view represents a side view of the patient and depth of the tube relative to the patient’s chest. The axial view is the transverse view of the patient looking from foot to head. The system does not require placement of a device on the patient’s body as the EM field generator is located on the system cart, which is placed at bedside. Additionally, as the EM sensor is embedded within the tube tip, the EMTS enables re-confirmation of the EFT tip location by simply reconnecting the EFT to its cable.
The marking of the two anatomical landmarks: (1) suprasternal notch and (2) xiphoid process using a registration pen, together with the positioning of the reference sensor on the midaxillary line enables scaling of the display to the patient’s upper body outline. An ideal division of the frontal screen on the EMTS into four quadrants is created by means of a crosshair. In contrast to the Cortrak receiver, which must be placed on the patient’s abdomen during the entire insertion procedure, the origin of the crosshair on the ENvue EMTS screen is determined only once during the initial set-up by marking the xyphoid process and remains stable and accurate throughout the subsequent procedure even with patient movement. With the Cortrak system, any movement of the receiver may impact the display grid and result in an inaccurate tracing.
With the ENvue EMTS, the two upper quadrants indicate the area of the lungs. The xiphoid process (lower anatomical landmark) represented by the central crosshair of the grid, specifies the transition from the esophagus to the stomach, with the left lower quadrant containing the stomach area and the right lower quadrant the area of the duodenum. The vertical line of the crosshair below the horizontal axis marks the area from which the stomach transitions to the pylorus and beyond to the duodenum and small intestine. The EFT is deemed MRI conditional per FDA.
Study protocol
Patients were screened to ensure compliance with the study inclusion and exclusion criteria. Following enrollment, baseline data were collected, and a physical examination was performed. All patients were placed in supine or semi-Fowler’s position for the start of the placement. All EFTs were placed using the EMTS at bedside according to the manufacturer’s instructions. The clinician performing the placement selected one of two sizes of EFTs: 10 Fr, 140 cm or 12 Fr, 140 cm, according to the patient’s clinical needs; the protocol for placement was the same for both size options. The EMTS monitor with visualization of the insertion tracing was used for guidance throughout placement. Following tube placement, an abdominal radiograph was obtained to verify tube location. Tube tip location was then verified by the EMTS and by radiography at 12–49 hours following placement (at a follow-up visit). EFT tip locations per EMTS and radiograph were adjudicated and compared by a specialist in GI medicine. The GI specialist, who was blinded to the procedure, interpreted tip location according to EMTS and radiograph. The EMTS insertion tracing and radiograph of the same procedure were not viewed at the same time. The study coordinator then assessed agreement between the EMTS and radiographs regarding placement within the GI tract. For the EMTS and radiograph results, the tip location was designated as: small intestine (duodenum or jejunum), stomach, pylorus region, lung or ‘other’. If ‘other’, a specific location was recorded. Vital signs were collected prior to tube placement and during the follow-up visit. Occurrences of any adverse events (AEs) or device-related side effects were also recorded.
Outcomes
The primary outcome of the study was the placement of the EFT in an appropriate anatomical position, that is, within the GI system, without the occurrence of guidance-related AEs, such as pneumothoraces. Correct placement was determined by comparing tube tip location observed by the EMTS with an abdominal radiograph. This comparison verified that there was no mismatch between the EFT location as observed on the screen of the EMTS and the radiograph. A critical mismatch was defined as a scenario in which the EMTS would show placement in the GI tract, while the EFT was observed in the airways according to the radiograph. Any guidance-related serious AEs (SAEs) or AEs occurring during patients’ participation in the study were evaluated and documented.
The secondary outcome was the accuracy of re-confirmation of tube tip location using the EMTS. This was evaluated 12–49 hours after the procedure (at a follow-up visit), by re-connecting the EFT to the EMTS and comparing the EFT tip location on the screen with that observed on radiography. Timing varied based on patient condition and/or scheduling needs. In addition, the possibility of retrograde tube migration from the initial location was examined, and safety assessments that were not guidance-related were performed. Safety of the EMTS was evaluated by assessment of vital signs (pulse, respiration, blood pressure and oxygen saturation) during the procedure visit and during the follow-up visit. Non-guidance-related SAEs and AEs occurring during study were recorded.
Data collection
The study database was designed and managed using Medrio Electronic Data Base (Medrio, San Francisco, California, USA). Following patient enrollment, baseline data were collected; these data included patients' demographics, weight, height, medical history, concomitant medications and the presence of an ETT. If a patient did not have an ETT, the level of sedation or obtundation was evaluated. Prior to tube placement, a physical examination was performed, and vital signs were recorded. These data were also recorded prior to the follow-up re-confirmation of tube tip location. Additional variables related to the EFT placement procedure were documented, such as tube size and insertion route (oral or nasal). The occurrence of AEs and device-related side effects during the study were also recorded.
Results
Study population
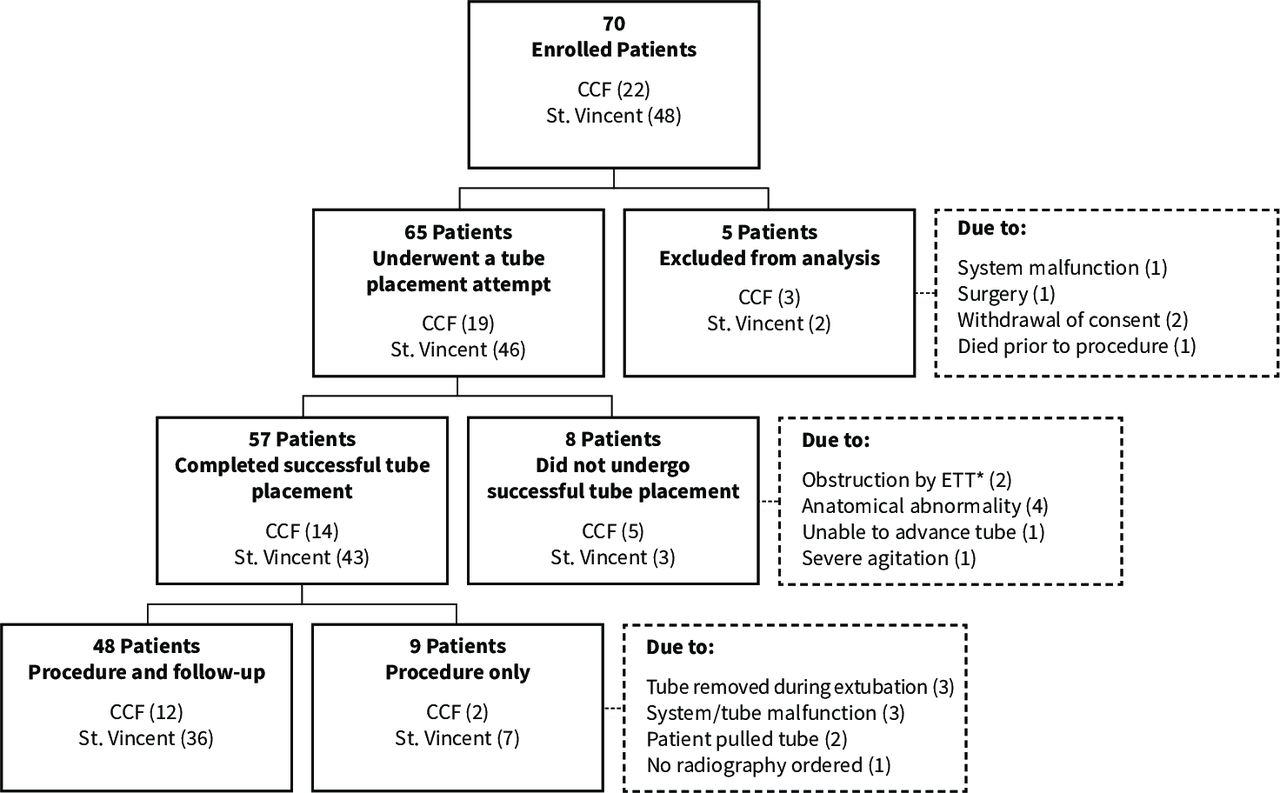
Seventy consecutive patients in total were enrolled (22 at CCF and 48 at St. Vincent). Five patients were excluded from the study analysis. Reasons for exclusion are shown in figure 1. The remaining 65 patients were included in the intent-to-treat analysis and underwent a tube placement attempt. Of these, 57 (88%) completed a successful placement procedure and 8 did not (see reasons in figure 1). Of the 57 patients who completed a successful placement procedure, 48 (84%) underwent a successful tube tip position re-confirmation at the follow-up visit. Two patients pulled the EFT out and a new tube was placed several hours later in one of them. In total, 58 tubes were placed in 57 patients. Twenty-five procedures were performed using a 12 Fr tube and 33 with a 10 Fr tube. Of the successful tube placements, 31 (53.4%) were oral and 27 (46.6%) nasal.

Flow diagram of the study population. CCF, Cleveland Clinic Foundation. *ETT,Endo Tracheal Tube.
Demographic characteristics and baseline data of the patients included in the analysis, according to successful placement are presented in table 1. Patients’ age ranged from 23 to 88 years (median age 64 years). Twenty-four (37%) were females and 41 (63%) males. All patients had an ETT except for six patients who were obtunded (two patients with GCS of 9, two with GCS of 10 and two with GCS of 11). Placement was successful for all the obtunded patients.
Demographic and baseline data
Primary outcome
For all 58 successful placements, an EFT was appropriately placed in the GI tract, according to radiography. According to both the EMTS and the radiographic confirmation (figure 2), there were no lung placements and no pneumothoraces or any other guidance-related AEs. In two patients, feeding tube deviation from midline (vertical line of crosshair) above the horizontal axis was noticed on the EMTS screen suggesting EFT passage towards pulmonary structures. This was recognized by the clinician and EFT was removed promptly. Radiography showed 27 tubes placed in the small intestine, 22 tubes in the stomach and 9 tubes in the pylorus region. Complete agreement of tube tip location between the EMTS evaluations and radiographs was achieved for 56 of the 58 placements: 22/22 in the stomach, 9/9 in the pylorus region and 25/27 in the small intestine (shaded values in table 2A). One patient was described by the EMTS as having the distal feeding tube tip in the pylorus region and by the radiograph as being positioned in the gastric antrum, or first portion of the small intestine. The location reported by the EMTS is in between the two locations described by the radiograph; therefore, the placement was categorized in the pylorus region according to both the EMTS and the radiograph. Two patients were described by the EMTS as having the distal feeding tube tip in the stomach region and by the radiograph as being in the small intestine.

{kind=link}
{kind=link}
Postprocedural radiograph (A) with comparison to electromagnetic tracking system screen (B).
Comparison between EMTS tip location and radiograph tip location
Secondary outcomes
Re-confirmation of tube tip location using the EMTS
During the follow-up visit, tubes were re-connected to the EMTS and tip location was compared with that demonstrated by radiography. Follow-up radiographs were taken between 12 and 49 hours after the procedure, and the data were compared with tube tip location re-confirmation using the EMTS in 48 (84%) of the patients. Two patients pulled the EFT out, three patients were extubated and the EFT was removed with the ETT prior to the follow-up visit and three patients did not undergo tube tip location re-confirmation using the EMTS due to system or tube malfunction. For one patient, tube tip location was re-confirmed using the EMTS, but a radiograph was not ordered.
For 43/48 (89.5 %) of the patients for whom EMTS screen and radiography data were available at the follow-up visit, there was full agreement between the evaluations (shaded values in table 2B). For the five remaining patients, the misalignment between the evaluations was within the GI tract (pylorus vs stomach, small intestine vs stomach, stomach vs pylorus, small intestine vs pylorus and stomach vs small intestine, according to the EMTS and radiograph, respectively).
Retrograde tube migration
The position of the distal feeding tube tip according to the EMTS screen during the follow-up visit was compared with the initial position at the time of procedure performance. Comparison of these findings are presented in table 3. If a retrograde migration of the EFT from its initial location was identified, then the EFT was repositioned based on clinical discretion. The patient who had EMTS evaluation but not radiography was included in the current analysis. Therefore, in total, there were 49 patients who underwent re-confirmation of tube tip location using the EMTS. Of the 49 patients, 4 (8%) demonstrated retrograde tube migration (shaded values, table 3). For two patients, the EFT migrated from the small intestine to the stomach, in one patient from the small intestine to the pylorus and in one from the pylorus to the stomach.
Tube migration as assessed by EMTS tip location immediately after placement and EMTS tip location at the follow-up visit
Safety assessment
All vital signs were stable throughout the entire study. One non-guidance-related AE was reported during the study course, which was related to tube manufacturing.
Discussion
This is the first clinical study to use a novel EMTS for the placement of EFTs into the stomach or small intestine of adult patients. We demonstrated the feasibility and safety of the system by confirming that 100% of the EFTs were placed in appropriate anatomical positions, that is, in the GI tract and not the respiratory system, and without the occurrence of any guidance-related AEs. The avoidance of airway misplacement in all patients is a significant clinical finding of the current study. Given the concerns of patient safety, and the potential for morbidity and even mortality, avoiding lung placement is essential for any placement device or system.
In this study, the anatomical positions of the EFT tip were confirmed both by the EMTS and by abdominal radiographs. High agreement (96.5%) was demonstrated between tube location according to the EMTS and the location observed with the abdominal radiograph. Discrepancies in confirming location were evident in only two patients; for both, the EMTS designated the tip position in the stomach region and the radiograph located it in the small intestine. This difference could be related to lag time (28 and 77 min) between EFT placement and radiographic confirmation, since tube migration may occur at any time after (or during) feeding tube placement, due to normal peristaltic activity.33 34
This report of successful placement of all EFTs in anatomically correct positions, together with the high agreement between the EMTS and radiography, contrasts with recent documentation of inadvertent EFT placements in the respiratory system, using the Cortrak system, as detected on radiographs.18 29–31 Several events of pneumothoraces using the Cortrak system were associated with cardiopulmonary arrest, and 11 reports of patient deaths were considered by the FDA to be possibly related to those lung injuries.32 Reasons for unsuccessful placement with the Cortrak system include technical difficulties and the specialized skills required in its operation. A transmitting stylet is used in that system, and a receiver unit is placed over the patient’s xiphoid process. The receiver tracks the location of the feeding tube tip, displaying a two-dimensional image on the monitor. However, the receiver must be stable and properly positioned throughout the entire procedure. Incorrect positioning or movement of the patient can alter the insertion tracing, potentially missing pulmonary placement.18 29–31 Accordingly, the FDA warned that extra precautions must be taken when placing a feeding tube using the Cortrak system.32 The FDA recommendations include the use of the Cortrak device only by a trained clinician, ensuring stability and correct positioning of the receiver throughout the procedure, and proper tube tracing. If any signs of respiratory distress are noticed during the procedure, the EFT should be withdrawn immediately. Moreover, tube tip location should be confirmed per institution protocol and not rely on the centimeter marking or the quadrant on the screen. Importantly, the EMTS used in the current study does not require placement of a device on the patient’s body, as the EM field generator is located on the system cart, which is placed at bedside. Moreover, the sensors of the system compensate for any natural movement by the patient.
An advantage of the novel EMTS demonstrated in this study was the ability to verify tube location after the initial tube placement procedure without the need for stylet re-insertion, as the EM sensor is embedded within the feeding tube tip. This important feature could eliminate the need for radiographic exposure for ongoing verification. A few studies have shown the inaccuracy of auscultation and the recommendation of other methods to confirm tube location.35 36 Confirmation of tube location is easily performed with the EMTS, by simply re-connecting the EFT to the system.
For 4 of the 49 patients (8%) who underwent re-confirmation of tube tip location at a follow-up visit using the EMTS, retrograde tube migration was demonstrated from the initial location. Tube migration is not an abnormal occurrence, and the causes are multifactorial including surgery, type of tube, inflammatory response, hormonal response, immobility, use of opioids, prokinetic agents, critical illness, mechanical ventilation and the presence of enteral nutrition.1 33 34 37 Little information exists in the literature to quantify the extent of tube migration, especially retrograde migration, and more research is warranted in this matter.
A strength of this study is the prospective design. One limitation of the study is the relatively small convenience sample. A larger sample is recommended to validate these initial findings.
In conclusion, we showed that placement of EFT using this EMTS is feasible and safe and can be used as an adjunct to current practices for placement of enteral feeding tubes. The system received FDA clearance in January 2019. The ENvue system is intended as an adjunct to current placement practices for assisting clinicians who place feeding tubes. The ENvizion EFT position must be confirmed per institutional protocol.
Acknowledgments
The authors would like to thank the nurses in the Trauma/Neuro ICU at St. Vincent and the Nutrition team members at Cleveland Clinic for their participation in placement of feeding tubes at the bedside for this research study.
References
Footnotes
Contributors LEJ participated in data analysis and interpretation, and preparation and critical review of the manuscript. MO participated in data analysis and interpretation, and preparation and critical review of the manuscript. JMW, JFS, AS, RB, ME, HMW, HV, DFK participated in data analysis and interpretation, and critical review of the manuscript. JMS participated in critical review of the manuscript.
Funding This research was sponsored by ENvizion Medical Ltd.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the review boards of both Cleveland Clinic Foundation (CCF), Cleveland, Ohio and St. Vincent Indianapolis Hospital and Health Care Center, Indianapolis, Indiana.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.