Article Text

Abstract
Background The obese (body mass index, BMI > 30) have been identified as a subgroup of patients in regards to traumatic injuries. A recent study found that high-grade hepatic injuries were more common in obese than non-obese pediatric patients. This study seeks to evaluate whether similar differences exist in the adult population and examine differences in operative versus non-operative management between the obese and non-obese in blunt abdominal trauma.
Methods Patient with trauma evaluated at an American College of Surgeons verified Level I trauma center from February 2013 to November 2016 were retrospectively reviewed. All patients aged >18 years with blunt mechanism of injury and a BMI listed in the trauma registry were included. Patients were excluded for incomplete data, including BMI or inability to grade hepatic or splenic injury. Data collected included age, gender, BMI, injury severity score, hospital length of stay, procedures on liver or spleen, and mortality. Organ injuries were scored using the American Association for the Surgery of Trauma grading scales, and were determined by either imaging or intraoperative findings. Obesity was classified as BMI > 30 compared with non-obese with BMI < 30.
Results During the study period, 9481 patients were included. There were 322 spleen injuries and 237 liver injuries, with 64 patients sustaining both liver and splenic injuries. No differences existed in the percentage of high-grade hepatic or splenic injuries between the obese and non-obese. Obese patients with liver injuries were more likely to have procedural intervention than non-obese liver injuries and had higher rates of mortality. No differences were found in intervention for splenic injury between obese and non-obese.
Conclusions Contrary to prior studies on adult and pediatric patients with trauma, this study found no difference between obese and non-obese patients in severity of solid organ injury after blunt abdominal trauma in the adult population. However, there was an increased rate of procedural intervention and mortality for obese patients with liver injuries.
Level of Evidence 3.
- trauma and obesity
- abdominal trauma
- liver injury
- spleen injuries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A global increase in the prevalence of obesity has increased interest in the obese patient as a subgroup in the medical field. In the field of trauma surgery, there have been multiple studies that have identified outcomes and injury patterns unique to obese patients.1–3 Many of these studies have focused on morbidity and mortality outcomes, hospital length of stay (LOS), and pulmonary dysfunction found in obese patients with trauma. However, a recent study evaluated the impact of obesity on solid organ injury among pediatric patients.4 Vaughan et al, performed a multi-centered prospective analysis, evaluating 117 pediatric patients with solid organ injury after blunt abdominal trauma, and found pediatric obese patients were more likely to sustain a high-grade hepatic injury (grade 4 or 5) with no difference in the rate of severe splenic injury. Boulanger et al also evaluated solid organ injury in the obese adult population and reported a decrease in the incidence of all hepatic injuries in the obese population.5 This study evaluated all injury patterns between obese and non-obese patients with blunt trauma, and also found there were no differences in intra-abdominal injuries with the exception of decreased hepatic injuries.
Differing injury patterns in the obese population has affected prognosis and management in patients with trauma. Therefore, we sought to evaluate solid organ injuries in the obese adult population.
Methods
A retrospective study was performed on adult patients (≥18 years of age) evaluated at Community Regional Medical Center, an American College of Surgeons-verified Level I trauma center in Fresno, California, from February 2013 through November 2016. Patients with blunt mechanism injury and a body mass index (BMI) recorded in the trauma registry were included and categorized as obese (BMI ≥30) or non-obese (BMI <30) based on the Center for Disease Control and Prevention’s definition of obesity.6 Patients with incomplete data, including missing BMI or inability to grade spleen or liver injury, were excluded from analysis.
Obese and non-obese patients were compared on age, gender, mechanism of injury, injury severity score (ISS), liver and spleen injury scores, angioembolization or operative interventions, hospital LOS, and mortality. Hepatic and splenic injuries were graded by imaging or intraoperative findings using the American Association for the Surgery of Trauma organ injury scaling system.7–9 In cases with discrepancies between imaging and intraoperative findings, the injuries were scored based on the intraoperative findings.
Categorical data are presented as percentages and continuous data are presented as mean±SD. Data were analyzed using Mann-Whitney U-test and χ2 analysis. Logistic regression was used to calculate the predicted probability for angioembolization at each BMI. Multivariate regression was used to adjust for confounding variables. Statistics were performed using the Statistical Package for Social Sciences (SPSS V.23.0, IBM) with significance attributed to a p value of <0.05. This study was performed with the approval of the Institutional Review Board of Community Medical Centers/UCSF Fresno.
Results
During the study period, 10 525 patients ≥18 years of age were seen at our institution following blunt traumatic injury. Of these, 1044 were excluded for missing data and 9481 were included in the analysis.
Overall, there were 6953 non-obese patients and 2528 obese patients. Demographics and outcomes are listed in table 1. There was a significant difference in BMI (p<0.001) between the obese and non-obese population which is to be expected. There were no differences found in age, LOS, mortality, or incidence of liver and spleen injuries between obese and non-obese patients. Differences in mechanism of injury were noted with the obese population having more motor vehicle collisions (p<0.001) and fewer assaults and falls (p<0.001). There were 322 splenic injuries (obese n=91, 4%) and 237 hepatic injuries (obese n=55, 2%), with 64 patients having both splenic and hepatic injuries.
Patient demographics
Comparisons of obese versus non-obese patients with liver and spleen injuries are listed in tables 2 and 3. Demographics of patients with liver injuries were similar between groups, but obese patients had an increased rate of motor vehicle collisions (p=0.002) and a decreased rate of pedestrian or bicycle versus automobile injuries (p=0.034). In patients with splenic injuries, there were no differences in demographics with the exception of obese patients having increased rates of motorcycle collision than non-obese patients with splenic injuries (p=0.031) (table 2).
Patient demographics, obese vs non-obese
Liver and spleen injury grades, obese vs non-obese
Grades of injury between obese and non-obese were evaluated (table 3). There were no differences in the liver injury grades between the obese and non-obese. In patients with splenic injuries, there was a higher rate of grade 1 injuries in the non-obese, and higher rate of grade 5 injuries in the obese.
Obese patients with liver injuries had an increased rate of intervention compared with the non-obese group (36% vs 22%, p=0.032), with the primary difference found in the rates of interventional radiology embolization (9% vs 2%, p=0.019). No difference in surgical intervention of the liver was observed between obese and non-obese patients (29% vs 20%, p=0.17). For splenic injuries, there were no differences found in the rates of intervention between obese and non-obese patients (table 4).
Intervention and outcomes, obese vs non-obese
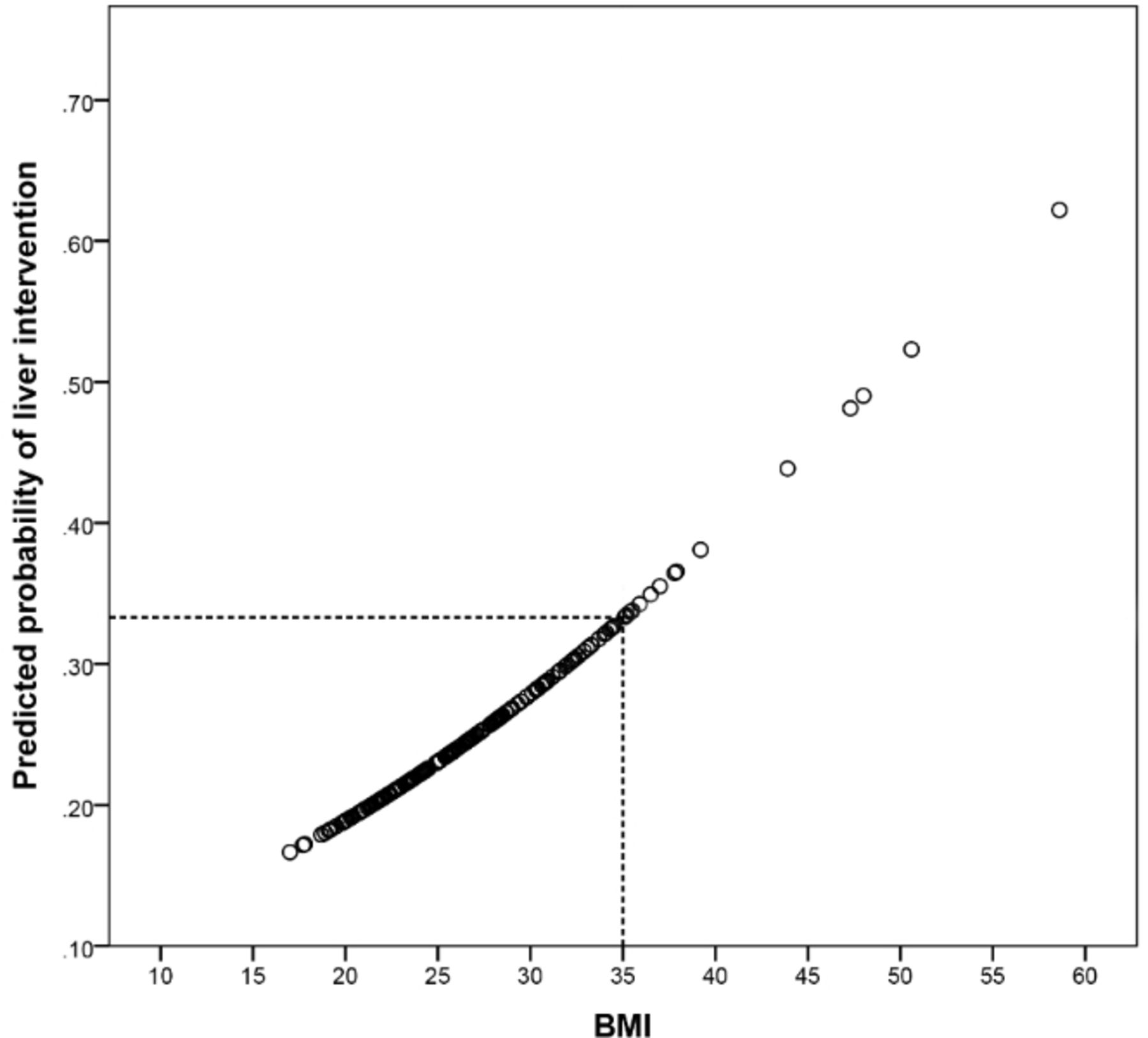
Using our linear regression, there was a positive correlation between BMI and liver intervention, with a predicted rate of intervention at 33.3% at a BMI of 35 (figure 1). Multivariate regression was used to assess confounding factors. The effects of obesity, ISS, age, and severity of liver injury on liver embolization were analyzed. Obesity and severe liver injury were the only factors correlated with liver embolization (p=0.016 and p=0.008, respectively).

{kind=link}
Correlation of BMI and intervention for liver injuries. BMI, body mass index.
Of note, there was an increased rate of mortality for obese patients with liver injuries compared with non-obese patients (22% vs 9%, p=0.009). However, 9 of 12 (75%) of these died from severe traumatic brain injury (TBI; with ISS >25), and the remaining from sepsis, cardiac failure, and withdrawal of care (advanced directives). There was no difference in mortality in patients with splenic injury. There were no differences in hospital LOS between obese and non-obese patients with liver (p=0.69) or splenic injuries (p=0.57).
Discussion
The obesity epidemic has led to an increased interest in this patient population, particularly in trauma. Multiple studies have been conducted on the outcomes of trauma in obese patients, with studies finding worse pulmonary outcomes, increased likelihood of nosocomial infections, and greater mortality.1–4 Injury patterns of obese patients have also been studied. In 1992, Boulanger et al conducted a retrospective study evaluating blunt injury patterns on 6368 adult patients and found that obese patients had an increased rate of thoracic and pelvic injuries, but decreased head and liver injuries.5 They postulated that increased abdominal wall and mesenteric fat may have had a protective effect in blunt abdominal trauma, but there was no difference in incidence of splenic trauma between the two groups. The study further speculates on the potentially protective role of fatty liver infiltration in the setting of blunt trauma. A recent study by Vaughan et al in 2016, evaluated blunt abdominal trauma in 117 pediatric patients, and found that obesity was associated with a higher likelihood of severe hepatic injury, but had no impact on splenic injury.4 This study also speculates the role of fat infiltration of the liver and its part in hepatic injury. Differences in our findings compared with Boulanger et al may be attributed to improvements in safety equipment and vehicle designs (seatbelts, air bags) and hence may explain the difference in injury patterns seen.10 11
The present study focused solely on blunt solid organ injuries in adult patients. We found that there was no difference in the likelihood of severe liver injury between obese and non-obese adults, unlike findings reported in both Boulanger et al and Vaughan et al which suggested decreased rates of liver injury and increased rates of injury severity respectively. The findings of our study suggest that obesity does not offer either protective or deleterious results from blunt abdominal trauma in regards to severity of liver and spleen injury. When evaluating for all grades of liver and spleen injury and obesity, we found that non-obese patients had higher rates of grade 1 injuries and obese patients had higher rates of grade 5 injuries that were significant. It remains unclear why this correlation exists. No differences were found between obese and non-obese patients for liver injury severity.
Unlike previous studies, our study demonstrated an increased rate of intervention in obese patients with liver injuries. There were no differences in rates of surgical intervention, but there was an increase in embolization procedures. Multivariate linear regression analysis confirmed that the rates of angioembolization were significant to BMI and severity of liver injury, and not significant to age or ISS, which suggests confounding was unlikely. Furthermore, we evaluated the predicted probability of intervention based on BMI, which found a positive correlation between the two, with BMI of 35 having a 33.3% probability of requiring intervention.
Furthermore, obese patients with liver injury also had an increase in mortality. The mortality of obese patients with liver injury in this study was overwhelmingly from TBI and none were attributed to the liver injury. Prior studies suggested that increasing BMI was associated with worsening morbidity, but without any change in mortality.2 The effect of liver injury does not translate to increased mortality in the non-obese populations, and there are no differences in mortality in splenic injury between obese and non-obese.
Non-alcoholic fatty liver disease (NAFLD) is a manifestation of metabolic syndrome and is highly associated with obesity,12 but its role in hepatic friability during abdominal trauma remains unclear. The nature of fatty infiltration and the role of NAFLD on blunt abdominal trauma remain to be elucidated but had been cited previously in two other studies focusing on obesity and blunt abdominal trauma. Fatty liver was previously mentioned as possibly having a role in increasing hepatic injury severity in obese pediatric patients. However, our study did not demonstrate more severe hepatic injury with obese patients. Using obesity as a correlate for NAFLD, it did appear to have an impact in obese adult patients with liver injuries in that it required increased intervention and those patients had increased mortality. However, the true nature and pathophysiology between obesity, NAFLD, and its effect on traumatic liver injury remains unclear. Future studies should be conducted to clarify the role of NAFLD in the outcomes in obese patients with trauma.
This study has all the limitations of retrospective study and from a single institution. Differences in patient demographics, such as increased rates of male gender and ISS in the non-obese patient population, did reach statistical significance, but it is questionable on whether or not this difference had any real clinical significance (ie, male gender 68% vs 64% and ISS 11 vs 10). Differences in mechanism of injury between obese and non-obese liver and splenic injuries are also noted. Although obese patients did have statistical significant differences in some of their mechanism of injury, we feel there are ultimately a balance among high and low impact injuries (decreased rates of assault, but increased rates of pedestrian/bike vs auto). Our study has the benefit of being the largest study on impact of obesity on blunt abdominal trauma that we are aware of.
Conclusion
This study of blunt liver and/or splenic injury found no difference in the likelihood of high severity solid organ injuries between obese and non-obese patients. Obese patients with blunt liver injury were found to have increased rates of intervention, namely embolization, and increased mortality.
Footnotes
Presented at Preliminary results presented October 4, 2017, at the Committee on Trauma, American College
of Surgery, Oakland, CA.
Contributors AKC, DJ, and JWD conceived the idea for the study. AKC, JCS, KM, and RB contributed toward data collection. RD performed statistical analysis and development of all figures and tables. The manuscript was written by AKC, RD, and JWD. The article was reviewed and edited by LPS, AMK, and MMW.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article.