Article Text

Abstract
Background Hemorrhage remains a major cause of death around the world. Eighty percent of trauma patients in India do not receive medical care within the first hour. The etiology of these poor outcomes is multifactorial. We describe findings from the first Stop the Bleed (StB) course recently offered to a group of medical providers in southern India.
Methods A cross-sectional survey of 101 participants who attended StB trainings in India was performed. Pre-training and post-training questionnaires were collected from each participant. In total, 88 healthcare providers’ responses were analyzed. Three bleeding control skills were presented: wound compression, wound packing, and tourniquet application.
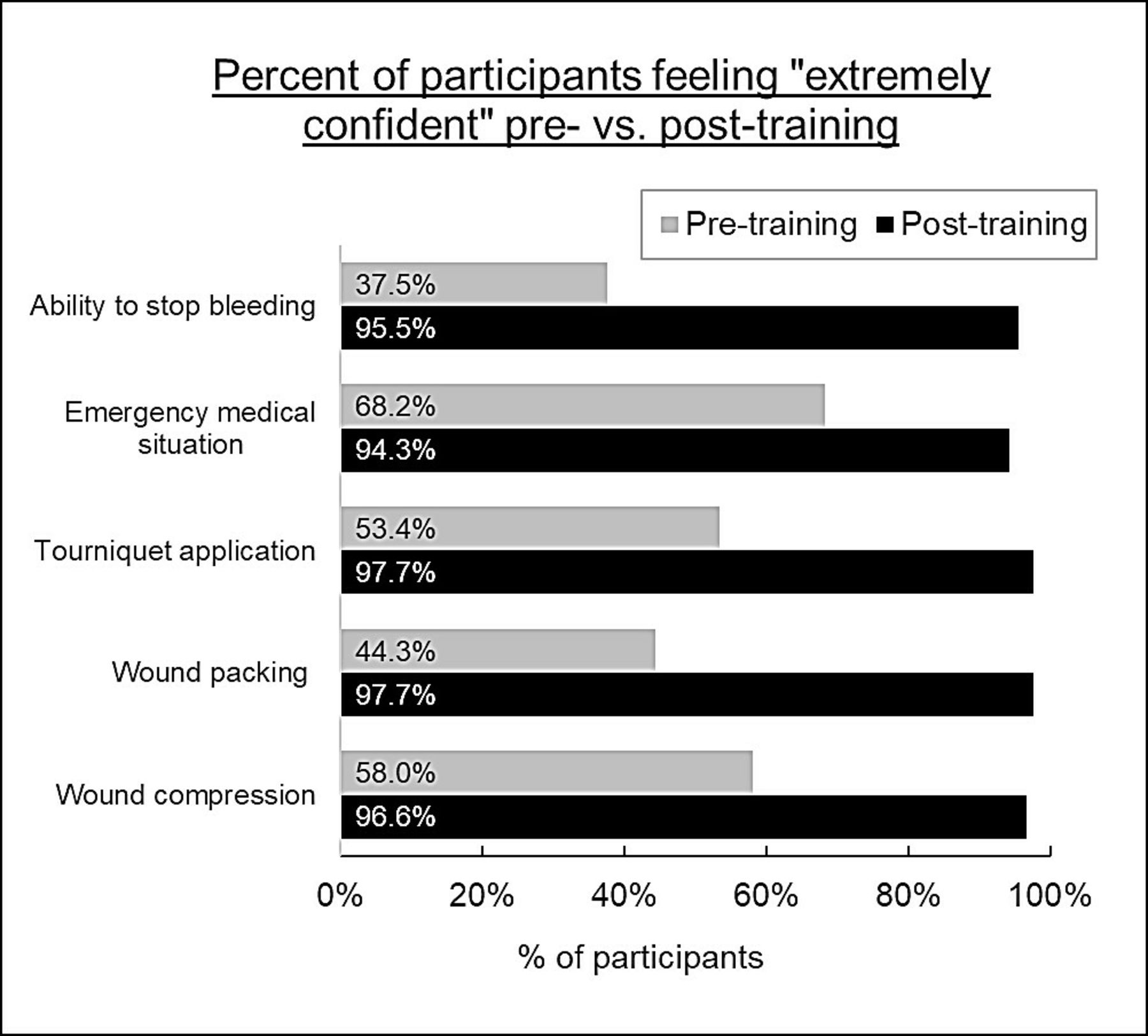
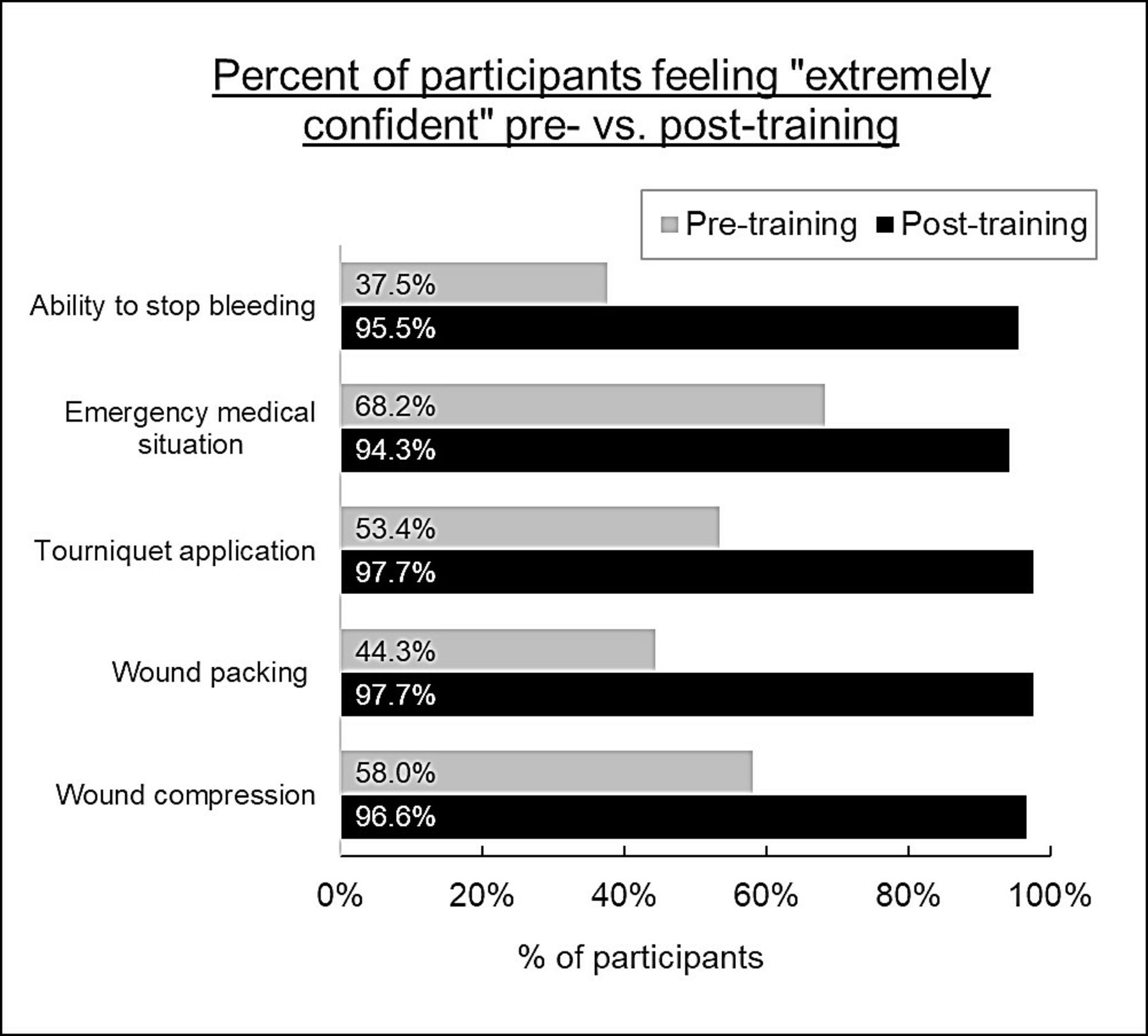
Results Among participants, only 23.9% had received prior bleeding control training. Participants who reported feeling ‘extremely confident’ responding to an emergency medical situation rose from 68.2% prior to StB training to 94.3% post-training. Regarding hemorrhage control abilities, 37.5% felt extremely confident before the training, compared with 95.5% after the training. For wound packing and tourniquet application, 44.3% and 53.4%, respectively, felt extremely confident pre-training, followed by 97.7% for both skills post-training. Importantly, 90.9% of StB trainees felt comfortable teaching newly acquired hemorrhage control skills. A significant majority of participants said that confidence in their wound packing and tourniquet skills would improve with more realistic mannequins.
Conclusion To our knowledge, this is the first StB training in India. Disparities in access to care, long transport times, and insufficient numbers of prehospital personnel contribute to its significant trauma burden. Dissemination of these critical life-saving skills into this region and the resulting civilian interventions will increase the number of trauma patients who survive long enough to reach a trauma center. Additionally, considerations should be given to translating the course into local languages to increase program reach.
Level of Evidence Level IV.
- EMS
- first-aid
- traumatic hemorrhage
- prehospital care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hemorrhage remains a major cause of death around the world, with the highest mortality in low-income and middle-income nations.1 In India, seriously injured trauma patients are six times as likely to die compared with patients in high-income nations.2 Eighty percent of trauma patients in India do not receive medical care within the first hour.1 Disparities in access to care, long transport times, and insufficient numbers of prehospital personnel contribute to the nation’s significant trauma burden.3 4 A recent study of trauma in urban areas of India showed that 58% of all trauma deaths could be prevented and that among preventable deaths, hemorrhage was a leading cause.4 The etiology of these poor outcomes is multifactorial,1–4 with road crashes accounting for 2% of all deaths in India in 2005.5 Minimal enforcement of traffic safety laws contributes to high morbidity and mortality, with helmet and seatbelt use rates in road crashes only 63.3% and 32.4%, respectively.6 Healthcare providers (HCPs) in India do not receive routine, standardized training in hemorrhage control. Similarly, there are no trauma response public education programs for laypersons. To address the trauma crisis in India by creating an initial pool of trainers, the first Stop the Bleed (StB) hemorrhage control course7 was recently offered to a group of medical providers in southern India. A cross-sectional survey comparing participants’ hemorrhage control competency pre-training and post-training was performed to assess program effectiveness and identify opportunities for improvement.
Methods
The first two StB trainings were conducted in the rural town of Puttaparthi, Andhra Pradesh and the city of Bangalore, Karnataka in India during August 2017. Each training consisted of two sections: a 30 min lecture and a 30 min skills/practice portion. Three bleeding control skills were presented: wound packing, wound compression, and tourniquet application. Trainings were taught in English using the official StB ‘Bleeding Control Basic 2017’ slideshow presentation. At each training, the lecture was given by the same certified StB instructor (a US-based trauma surgeon). Skills sessions were led by certified StB instructors with a ratio of one instructor to eight trainees. Official StB training kits, containing rubber mannequins, gauze, and tourniquets, were used at all trainings. Only questionnaires from HCPs were included in the analysis; data from the five laypersons was excluded from the study. Pre-training and post-training questionnaires with a five-point Likert scale were used to collect data from participants. After subtracting eight incomplete questionnaires, response data was analyzed from 88 HCPs (figure 1). Questionnaires were written exclusively in English. The pre-training questionnaire consisted of 10 questions with scaled answer choices. The post-training questionnaire contained 17 questions with scaled answer choices and one free-response field for additional feedback. Each participant was directly observed correctly performing the three skills (wound packing, wound compression, and tourniquet application) by a certified instructor before passing the training. Certificates were given on completion. Data was analyzed in Microsoft Excel. Percentages were calculated using a sample size of 88 participants.
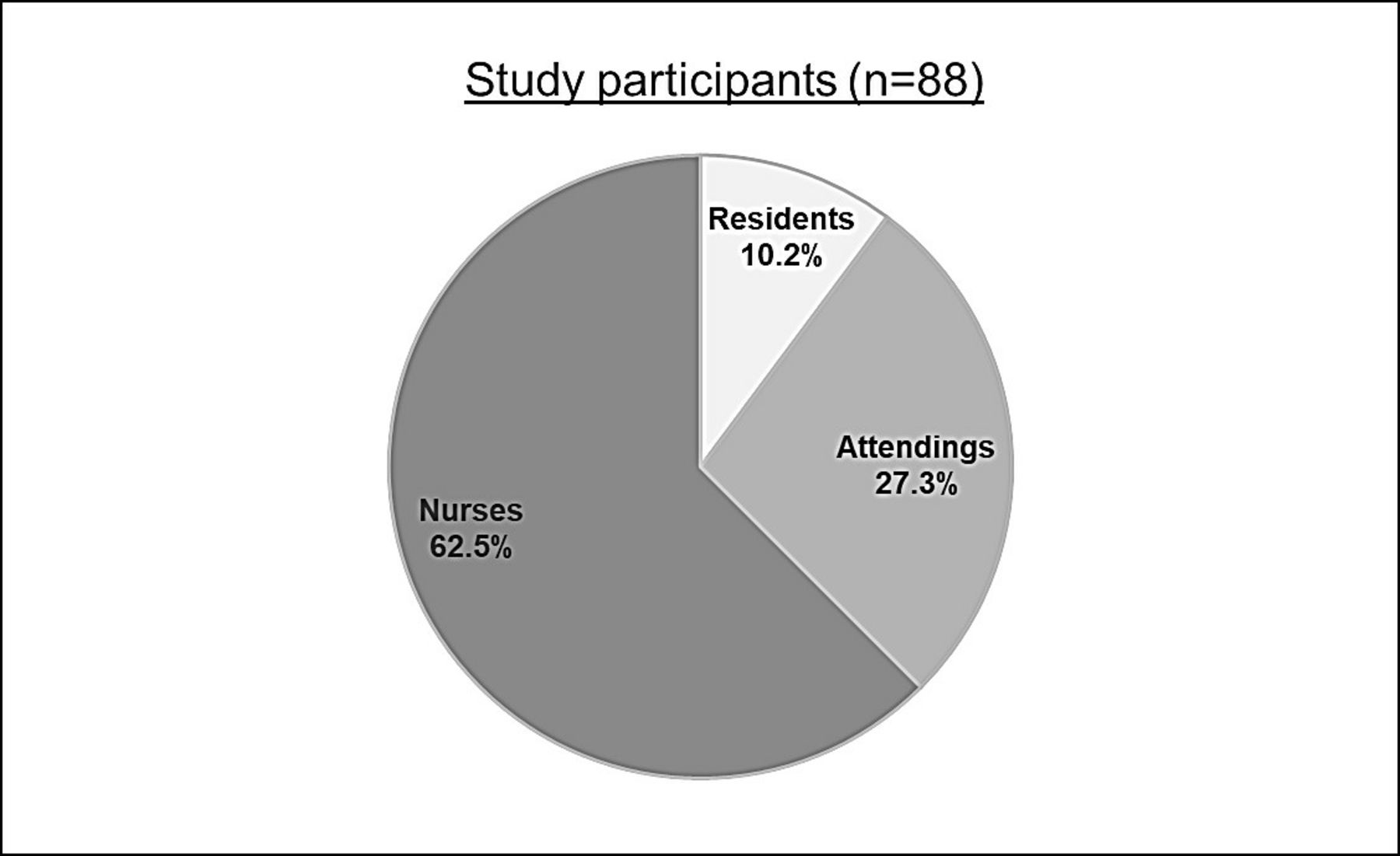
Study participants consisted of 88 healthcare providers, including nine resident physicians, 24 attending physicians, and 55 nurses.
Results
A total of 101 participants were trained and assessed on StB hemorrhage control skills. Participants included 96 HCPs and five laypersons, aged 19–75 years. Data from eight HCPs was excluded due to incompleteness. In total, 88 HCPs’ pre-training and post-training questionnaires were included in the analysis. The 88 HCPs consisted of nine resident physicians (10.2%), 24 attending physicians (27.3%), and 55 nurses (62.5%). Among HCPs, 88.6% had previously taken a cardiopulmonary resuscitation or first-aid training course. Only 23.9% reported any prior bleeding control training. Participants who reported feeling ‘extremely confident’ responding to an emergency medical situation rose from 68.2% prior to the training to 94.3% post-training. Regarding hemorrhage control abilities, 37.5% felt extremely confident before the training, compared with 95.5% after the training (figure 2). For wound packing and tourniquet application, 44.3% and 53.4%, respectively, felt extremely confident pre-training, followed by 97.7% for both skills post-training. Importantly, 90.9% of StB trainees felt comfortable teaching newly acquired hemorrhage control skills, as all the physicians and nurses who completed this course were certified as StB instructors. The training was well received, with 96.6% stating they would recommend the course to others. Only 76.1% of trainees said the model for wound packing was extremely realistic. When evaluating instructional equipment, 95.5% and 94.3% of participants stated that confidence in their wound packing and tourniquet skills would improve with a more realistic mannequin. Most participants (95.5%) said that material was presented using terms that were easy to understand. Additionally, the free response field of the post-training questionnaire revealed several trends. Three participants suggested translation of this program into local languages. Seven trainees requested supplementary videos or case discussions clarifying situations when hemorrhage control skills should be used.
{kind=link}
{kind=link}
Participant confidence in hemorrhage control and emergency response skills increased after the one-hour Stop the Bleed training.
Discussion
To our knowledge, this is the first StB training in India.1 This initial study confirmed our suspicion that Indian healthcare providers, in both rural and urban settings, are given little to no formal hemorrhage control training but are very eager to receive it. As India continues its tremendous economic growth, the purchasing power of its citizens will lead to more automobiles and motorcycles on roads that are poorly equipped for such high capacity. In addition to the sheer volume of people (current population 1.2 billion), there was previously no official national emergency response phone number in India. In 2017, the Telecom Regulatory Authority of India (TRAI) proposed ‘112’ as a single number to be used for all emergency phone calls, including police, fire and emergency medical service (EMS)/ambulance services.8 It has yet to be widely implemented across the country.
Unfortunately, India also lacks ambulances. The WHO recommends that for every 100 000 people, there should be at least one ambulance. New Delhi, the capital of India, with a population of 22 million people and growing, has only 152 state-run ambulances.9 This is approximately one ambulance for every 144 736 people, well below the WHO threshold. According to a 2012 study by the All India Institute of Medical Sciences, 28% of the 70 768 emergency calls received between March 2009 and May 2010 in the city were refused due to a shortage of ambulances.9 The ambulances that do exist often lack basic life support, such as oxygen or medications, let alone advanced equipment. Many ‘ambulances’ are simply white vans containing stretchers. If an ambulance does arrive on scene, response times can vary significantly based on rural or urban setting. Major traffic delays coupled with a lack of training for drivers on giving an ambulance the right of way exacerbate poor response times. Making the problem even worse is a lack of prehospital personnel in India. There are currently no standardized prehospital training standards or curriculum for designating emergency medical technicians.
Given the lack of resources, it is imperative that courses such as StB be taught across the country to provide laypersons a basic skill set to save a life until EMS/prehospital staff arrive. Importantly, work by non-governmental agencies, such as SaveLIFE Foundation and Save a Life, Give a Life Foundation, have helped champion the importance of trauma care in India. SaveLIFE, for example, helped create legislation to safeguard bystanders, or ‘good samaritans’, who come forward during emergencies to help the injured.10 This was passed into law in 2016 by the Supreme Court of India. By initially training HCPs in both rural and urban settings, we aimed to enhance the capabilities of trainers who will in turn train others using a train-the-trainer model.
This study has several limitations. Importantly, the study analyzed data from a small sample of HCPs (n=88). The StB program is intended for widespread public education. To that end, the program’s effectiveness should be studied in larger groups that include Indian laypersons to determine what changes must be made to terminology, skills practice, and teaching pace. Notably, pre-training and post-training questionnaires were written in English; this was not the first language of most participants and therefore may have impaired data validity. The questionnaire was also first-person subjective: it asked participants to rate their ‘confidence’ level with their new hemorrhage control skills. Measuring training success by participants’ self-perceived competency introduces potential bias, as participants are inexperienced and may try to give responses that flatter trainers and validate the training. The training was taught entirely in English, which is the second or third language of most HCPs in India. The potential language barrier may have led to miscommunication between trainers and trainees, or even prevented participants from asking more technical or nuanced questions about the training material. Future trainings, particularly directed toward laypersons, should be offered in the local language.
Improvements to the training kit should be made. Over 90% of participants recommended the use of more realistic mannequins. ‘Realistic’ was not explicitly defined but may refer to anatomical accuracy (resembling an arm or leg) or hemorrhage feedback (bleeding that stops when enough pressure is applied). Trainers also noted the heaviness and bulkiness of the training kits as deterrents to traveling with them. The high cost of the official StB mannequin training kit (over US$900) is prohibitive to program adoption and uptake, particularly in low-income countries like India. It should be noted that the StB course does not currently mandate any one training kit. This enables opportunities to develop inexpensive models with local materials. In fact, several US-based trainers have successfully performed StB training with inexpensive ‘home-made’ kits rather than the high-cost commercial equipment. Jugaad, a word in Hindi and a concept taught in business schools around the world, captures the meaning of finding a low-cost solution to any problem in an intelligent way.11 Developing a cost-effective StB training kit, particularly for low-income and middle-income countries, would be an example of Jugaad innovation.
The inclusion of expensive specialty gauze in some kits provided no benefit over generic gauze and could potentially be replaced with cheaper alternatives. Consideration should be given to using lighter-weight, anatomically accurate mannequins and generic gauze.
During conversations with participants, questions frequently arose about the circumstances in which one should apply hemorrhage control skills. It may therefore be useful for future versions of StB to include additional guidelines for intervention. Though not discussed in the questionnaires, conversations with participants during trainings also revealed widespread skepticism about the usefulness of learning tourniquet application. Participants wondered if a tourniquet would be available during an emergency and expressed interest in learning how to create make-shift tourniquets from everyday objects. Another limitation is the lack of delayed reassessment of knowledge and skills to quantify how much information participants had retained over a set time period. Despite these limitations, Indian HCPs benefited from StB trainings and felt confident using and teaching the skills to others after just one hour of training.
Dissemination of life-saving basic hemorrhage control skills into both rural and urban settings in India has significant potential to increase the number of trauma patients who survive long enough to reach a trauma center. Much more work is needed to match the training required for the large population.
Acknowledgments
The authors would like to thank the staff physicians and nurses of the Sri Sathya Sai General Hospital, Puttaparthi, Andhra Pradesh, India, and the Sri Sathya Sai Institute of Higher Medical Sciences, Bangalore, Karnataka, India, for their assistance in providing the trainees and venue for these training sessions.
Footnotes
Contributors LAS, SC, MK, AG, RJW, and MN served as STB instructors. LAS, SC, SL, CV, AG, RJW and MN drafted the manuscript and were integral in its editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.