Article Text

Abstract
Background Resuscitative endovascular balloon occlusion of the aorta (REBOA) is regaining popularity in the treatment of traumatic non-compressible torso bleeding. Advances in invasive radiology coupled with new damage control measures assisted in the refinement of the technique with promising outcomes. The literature continues to have substantial heterogeneity about REBOA indications, applications, and the challenges confronted when implementing the technique in a level I trauma center. Scoping reviews are excellent platforms to assess the diverse literature of a new technique. It is for the first time that a scoping review is adopted for this topic. Advances in invasive radiology coupled with new damage control measures assisted in the refinement of the technique with promising outcomes. The literature continues to have substantial heterogeneity about REBOA indications, applications, and the challenges confronted when implementing the technique in a level I trauma center. Scoping reviews are excellent platforms to assess the diverse literature of a new technique. It is for the first time that a scoping review is adopted for this topic.
Methods Critical search from MEDLINE, EMBASE, BIOSIS, COCHRANE CENTRAL, PUBMED and SCOPUS were conducted from the earliest available dates until March 2018. Evidence-based articles, as well as gray literature at large, were analyzed regardless of the quality of articles.
Results We identified 1176 articles related to the topic from all available database sources and 57 reviews from the gray literature search. The final review yielded 105 articles. Quantitative and qualitative variables included patient demographics, study design, study objectives, methods of data collection, indications, REBOA protocol used, time to deployment, zone of deployment, occlusion time, complications, outcome, and the level of expertise at the concerned trauma center.
Conclusion Growing levels of evidence support the use of REBOA in selected indications. Our data analysis showed an advantage for its use in terms of morbidities and physiologic derangement in comparison to other resuscitation measures. Current challenges remain in the selective application, implementation, competency assessment, and credentialing for the use of REBOA in trauma settings. The identification of the proper indication, terms of use, and possible advantage of the prehospital and partial REBOA are topics for further research.
Level of evidence Level III.
- resuscitative balloon occlusion of the aorta
- REBOA
- balloon vascular occlusion
- resuscitative aortic occlusion
- therapeutic occlusion of the aorta
- damage control occlusion of the aorta
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- resuscitative balloon occlusion of the aorta
- REBOA
- balloon vascular occlusion
- resuscitative aortic occlusion
- therapeutic occlusion of the aorta
- damage control occlusion of the aorta
Introduction/background
Hemorrhage remains the leading cause of preventable death in trauma.1 To control exsanguinating bleeding from non-compressible torso injuries, damage control measures use a variety of techniques to limit the blood loss. Invasive modalities, such as emergency room thoracotomy and aortic cross-clamping, have been used to control blood flow from the aorta.2 3
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is regaining momentum as a damage control measure applicable to patients in extremis. Refinement of the technique supported by advances gained from invasive radiology, endovascular treatment of abdominal aortic aneurysms, in addition to damage control measures previously unavailable assisted in driving this technique forward with promising outcomes.4 5 Despite the recent advancements, the literature is heterogeneous in regard to the indication, patient population, and challenges faced when implementing REBOA at a level I trauma center. Scoping reviews constitute an effective strategy to categorize heterogeneous research activity in a contradictory field and function as an excellent platform to assess the diverse literature of a new technology.6 We believe this review will assist in mapping key concepts and identify current knowledge gaps within the literature in regard to REBOA. This is the first scoping review adopted for this topic.
Review questions/objectives
Using a scoping review methodology, a systematic review of the literature was conducted from the earliest available reporting. The following research questions were addressed:
Benefits of REBOA—What are the clear indications, pitfalls, and advantages of its use compared with other available modalities?
Application of REBOA—Which selective population will benefit the most from its application through comprehensively designed algorithms?
Implementation of REBOA—What are the challenges in the adoption of the technique into the armamentarium of advanced trauma centers? Special attention was paid to the credentialing, quality indicators, and competency assessment parameters.
In addition, emphasis will be focused on the following:
Mapping the existing literature on REBOA technique.
Identifying features needed for the successful implementation of REBOA into trauma programmes.
Clarifying the important variables necessary for the evaluation of the technique, its outcome, and its efficacy.
Reporting the complications and long-term outcomes associated with REBOA.
Identifying areas for future development.
Material and methods
To the authors’ knowledge, there is no existing published scoping review of the new generation REBOA catheter usage within a trauma setting. This study follows the scoping review framework developed by Arksey and O’Malley,7 which has been enhanced further by Levac et al8 and Joanna Briggs Institute (JBI).9 The results are reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Protocols (PRISMA-P) guidelines.10
This method includes the following five steps: (1) identifying the research question; (2) identifying relevant studies balancing breadth and comprehensiveness; (3) study selection using an iterative team approach; (4) charting the data; and (5) collating, summarizing, and reporting the results as they relate to the study purpose and implications of the study findings for policy, practice, and research.
Search strategy
In collaboration with a hospital librarian, a systematic search strategy was applied to the following databases: MEDLINE, EMBASE, BIOSIS, COCHRANE CENTRAL, PUBMED, and SCOPUS from the earliest available date to March 2018. The search strategy included text words and indexing relevant to the identification of articles that discussed the use and the applications of REBOA. Our search terms included: ‘balloon occlusion’, ‘embolization, therapeutic’, ‘therapeutic occlusion’, ‘aorta’, ‘aorta occlusion’, or ‘artificial embolization’, combined with ‘resuscitation’, as well as ‘REBOA’. These terms were searched in article text, title, abstract, and keywords. The search strategy was applied to all databases, with modifications to search terms when necessary. Furthermore, the gray literature including clinical guidelines, trauma websites, recommendations from trauma associations and societies (American College of Surgeons, American Association for the Surgery of Trauma, Eastern Association for the Surgery of Trauma, American Trauma Society, Western Trauma Association, British Trauma Society, Trauma Association of Canada, Australasian Trauma Society, Trauma.org), all articles—research and non-research—regardless of quality, as well as the first 10 pages of Google were reviewed with the term REBOA or with scientific terms related to the technique.
A primary screening analysis of both the title and the abstract was performed by two independent reviewers (TP and YS) in conjunction with the inclusion and exclusion criteria.
The following study characteristics were excluded: studies describing the outcomes of REBOA use in non-trauma cases such as gastrointestinal bleeding and postpartum hemorrhage, studies describing the use of REBOA in the setting of limb amputation or solely for orthopedic indications (other than pelvic), pediatric studies, animal studies, cadaveric studies, and elective procedures.
Disagreements about study eligibility were discussed between the two reviewers until a consensus was reached. In circumstances where discussion did not result in an agreement, a third reviewer (OB) was consulted. Subsequently, full texts were reviewed independently by TP and YS using a predetermined standardized data collection spreadsheet. Variables extracted include type of study, country of publication, patient age and mechanism of injury, anatomical location of injury, location of REBOA insertion, medical personnel performing REBOA insertion, arterial access used, use of guided REBOA insertion, catheter size, zone of REBOA deployment, occlusion duration, complications, and implementation process of REBOA protocol. Potential bias was evaluated based on the methodological approach of each article; for example, retrospective analysis and case reports contain a limited sample size. The limitation of these studies and their influence are herein reported.
Data collection and statistical analysis were performed using Microsoft Excel for Mac V.15.27 (Seattle, Washington, USA). Data report was synthesized by TP as total number and percentage. All values reported were collected directly from the articles, and the graphs include the absolute number of studies that have reported on the specific variable.
Results
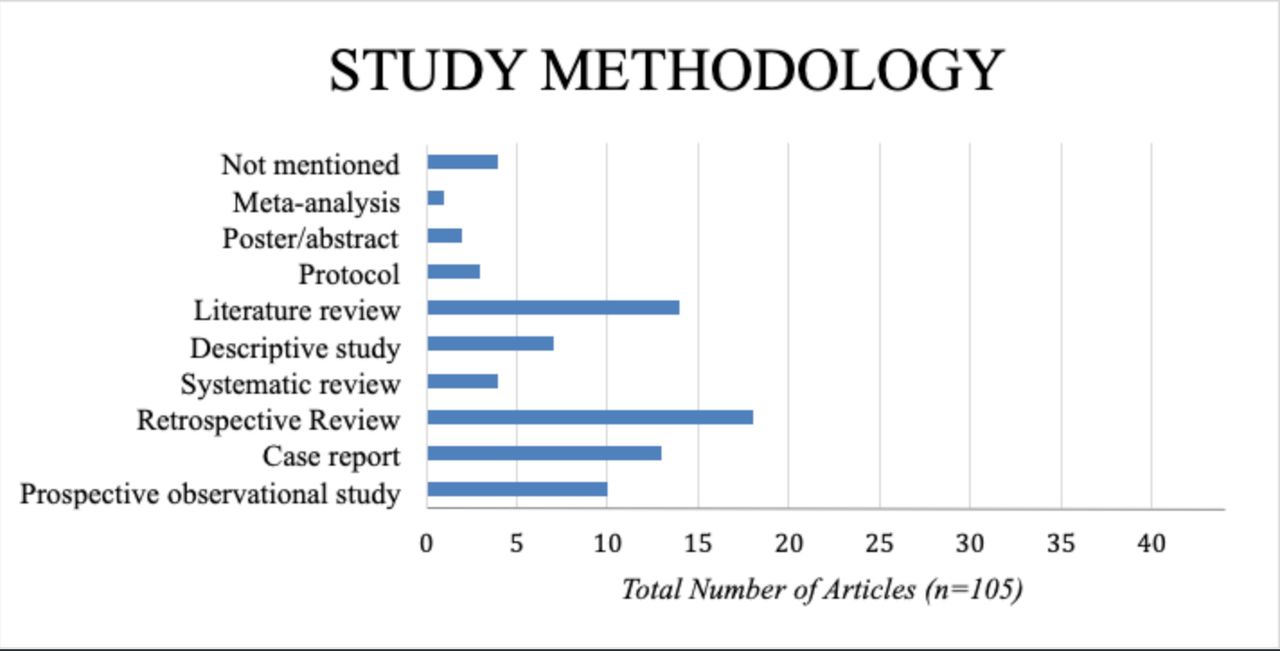
Database and gray literature analysis yielded 1244 articles (figure 1). After subsequent duplication removal, primary and secondary screening analysis based on inclusion and exclusion criteria, 105 articles were included in the study (figure 1).3 11–70 A large proportion of articles were retrospective. 13 studies were case reports, and 10 were prospective observational studies (figure 2). A total of 8741 patients were included in this report, with an age range of 17–93 years. Most articles were published within the USA (31 articles). The second most published country was Japan with 18 studies (table 1).
Depiction of article demographics and country of publication

2018 Preferred Reporting Items for Systematic Reviews and Meta-Analysis diagram and study outline. AAST, American Association for the Surgery of Trauma; ACS-COT: American College of Surgeons Committee on Trauma; EAST, Eastern Association for the Surgery of Trauma; TAC, Trauma Association of Canada.
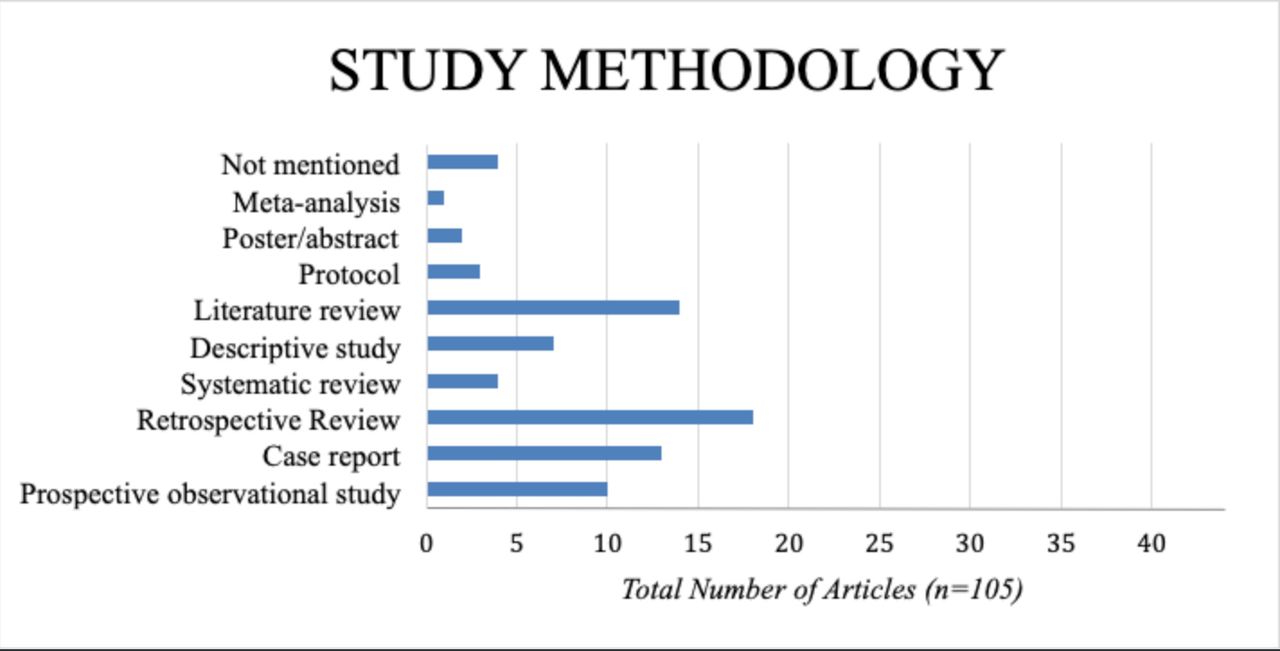
Different methodologies used by each study (not mentioned=4 (3.8%), meta-analysis=1 (0.9%), poster/abstract=2 (1.9%), protocol=3 (2.8%), literature review=14 (13.3%), descriptive study=7 (6.6%), systematic review=4 (3.8%), retrospective review=18 (17%), case report=13 (12.3%), prospective observational study=10 (9.5%).
When analysing the indications for REBOA, our findings demonstrated that 35 studies did not report on the mechanism of traumatic injury. Among those reporting on injury type, 32 articles were blunt trauma, 18 were penetrating, and only one article reported on REBOA usage in a mixed blunt and penetrating mechanism. Thirty-nine articles did not report a specific anatomical topography. The most common injury location was abdominal and pelvic trauma, although only seven studies reported thoracic injuries.
The emergency department was the most frequent location of REBOA insertion, followed by the operating room. Three studies reported REBOA insertion within the radiological suite or hybrid room.15 25 44 Interestingly, two studies discussed field insertion including road and air ambulance25 29 (figure 3). Trauma/acute care surgeons and emergency physicians performed most REBOA insertions. Vascular surgeons, interventional radiologists, intensive care physicians, and anesthesiologists were among the other specialties involved.

Location of resuscitative endovascular balloon occlusion of the aorta (REBOA) insertion: emergency department (ED), 19 (18.1%); operating room (OR), 15 (14.3%); radiological suite, 2 (1.9%); field or air ambulance, 2 (1.9%); hybrid room, 3 (2.8%); not mentioned, 43 (40.9%)
When examining the arterial access, over half of the studies reported the common femoral artery to be the arterial access of choice. Few studies reported the use of brachial and astonishingly the carotid arteries.13 15 Percutaneous access was reported in 24 studies, with only eight discussing the cut-down method. Guidance for REBOA positioning was reported in 22 studies with 10 using ultrasound guidance, and 11 using fluoroscopy. Majority of current articles reported the use of a 7-French catheter. As for the zone of deployment, most studies reported the balloon to be deployed in zones I and III, whereas six studies reported zone II deployment. Regarding the timing of aortic occlusion, 10 articles did not specify the duration. Only four articles reported aortic occlusion for 60 min,13 19 36 63 although nine studies reported 20 min to be the most observed occlusion time (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Duration of aortic occlusion: 10 min, 2 (1.9%); 20 min, 9 (8.5%); 30 min, 5 (4.7); 40 min, 3 (2.8%); 60 min, 4 (3.8%); other 10 (9.5%).
When analysing the complications, 19 studies mentioned complications related to REBOA. Thromboembolic events leading to lower limb amputation were reported in eight studies,12 19 22 28–32 pseudoaneurysm in six,12 19 24 29 32 34 and thrombosis with limb ischemia in three.18 54 64 One article reported the development of compartment syndrome in the lower limb.44 Other complications listed included cerebral hemorrhage,15 23 45 acute kidney injury,13 25 28 34 54 multisystem organ failure,28 and femoral artery injury.63 Balloon exiting through the aortic injury, balloon migration, and balloon rupture were also reported to a lesser degree.37 Complication rates were as follow: distal ischemic events and amputations in 12%,28 0.07% rate of balloon rupture,63 0.15% of balloon migration to zone II,58 and pseudoanyeurysm was reported in 6.5% of cases.12 A recent review of the literature on REBOA-associated complications emphasized the need for research on the complications associated with each stage of the balloon deployment.71 The table 2 depicts the reported complications found in the study analysis.
Reported complications associated with resuscitative endovascular balloon occlusion of the aorta
Our review also examined the gray literature related to REBOA (table 3). Most of the literature discussed clinical guidelines, associations’ recommendations, and unpublished reports of successful REBOA cases in the form of news articles, podcasts, and interviews.72–75 Five articles described the need for prospective REBOA data collection and the collaboration of multicentre reporting to an international registry. A large proportion of the literature describes the REBOA technique and indications for its use as well as its contraindications. Training and physician workshops are also topics of discussion, with some authors favoring a certified physician performing the technique, and others describing non-physician trained individuals. The use of REBOA in the field is mainly discussed in the setting of road and air ambulance and the potential use of REBOA within the military setting.76 Skepticism exists regarding REBOA usage and its associated complications; three reports discussed the risk of limb ischemia after aortic occlusion.
Summary of the gray literature (n=31)
Discussion
The principles of REBOA were first described during the Korean War by Colonel Hughes.11 Since that time, numerous articles of high and low quality, evidence-based and non-evidence based have accumulated. Few reports included systematic reviews, international registries, and meta-analysis,12–17 58 concluding at either equivalence or superiority of the technique when compared with other modalities. However, a recent review questioned the safety of the procedure, showing no evidence of improved survival.70 Other studies have shown the technique to be associated with an increased complication rate, notably lower limb amputations and acute kidney injuries when compared with a similar cohort of patients.23 77
Presently, there are 14 types of reviews available in the literature.78 Scoping review, or mapping review, is a relatively new methodology developed in 2005 to evaluate the existing literature by examining the high-quality and low-quality studies. This method focuses on identifying current gaps within the literature and identifies areas for future research and advances.6 79
Most of the published literature comes from the USA22 and a substantial portion from the military experience.21 27 The number of publications originating from Japan was also noted.16 17 23 28 46 60 62 64–66
Conducting a coordinated clinical randomized controlled trial is difficult to perform in trauma, especially when dealing with unpredictable life-saving procedures with a possible ethical dilemma. The majority of study designs are case reports, case series, literature reviews, or retrospective analysis. Article integrity was evaluated based on the methodological approach of each article. Therefore, with a large proportion of retrospective analysis and case reports, our findings were limited to the nature of these studies. Our analysis depicted only four systematic analysis and one meta-analysis discussing REBOA. The number of cases per article rarely exceeded 10–20 cases per article, with scattered reports collecting 900 patients or 1400 cases per study (figure 2).12–17
The most common location of insertion was the emergency department followed by the operating room (figure 3). If the condition of the patient allows, inserting the catheter in the operating room’s controlled settings would be advisable, especially when starting a new REBOA programme. The ‘on-field’ or ‘during-transport’ insertions should be approached with caution and be kept for a very restricted selection of cases with a well-defined postinsertion plan.70
Trauma surgeons shared the highest reporting rate of insertion along with the emergency doctors.
Most of the early reports discussed the open approach to be the standard of care, but with growing evidence of improved insertion skills and expertise following training courses using the percutaneous and ultrasound-guided approach, this modality is slowly replacing the cut-down access, which is reserved for difficult approaches or failure percutaneous trials.
Every effort should be made to cannulate the common femoral artery, considered by most authors to be the rate-limiting step for the success of every procedure.70 Cannulating the superficial femoral artery will result in a high rate of thromboembolic events with subsequent adverse effect on the blood supply of the corresponding lower limb.54 Most guidelines discussed the advantageous use of immediate arterial line insertion at the groin site for patients presenting with hypotension to the trauma bay without chest exsanguinating injuries. The line insertion might assist in the monitoring of the hemodynamic parameters and improve the technical accessibility skills of the inserting person attempting a quick cannulation. The arterial line can be upsized with ease to accommodate the REBOA sheath in case of need.39
As abdominal and pelvic injuries made the vast majority of injury localization, balloon deployment occurred mostly in zone I and zone III. Although considered to be a ‘non-inflatable zone’, inadvertent or temporary inflation in zone II was reported rarely. Most of these inflations happened either during the first reports of the initiation of the catheter insertion programme or as a result of the utilization of low profile—wire free—devices.33 44
The use of REBOA in thoracic trauma either isolated or combined with other torso injuries is debatable. Current recommendations are against its use in injuries above the point of REBOA deployment as it could increase the bleeding and worsens the patient’s outcome. However, one recently published case series of seven patients by Ordonez et al challenged these recommendations, as they successfully used REBOA in conjunction with a median sternotomy in patients with penetrating thoracic trauma and significant intrathoracic injuries. The use of REBOA in those patients significantly increased the systolic blood pressure through intravascular blood redistribution and likely better cardiac and cerebral perfusion, till definitive control was established, without worsening bleeding or reported adverse effects; thus, its role in chest trauma is yet to be studied.80
Some reports have shown the possible aortic occlusive tolerance with subsequent warm ischemia up to an hour, even some articles reporting durations as long as 90 min.19 Our review shows that the most described reportable occlusion time was 20 min (figure 4). Most trauma centers are trying to avoid occluding the vessel for more than 60 min to prevent deleterious thromboembolic complications and reperfusion events.
Among the reported adverse events related to REBOA, the development of cerebral bleeding should be evaluated with caution. Some reports showed the complication to be related to the balloon deployment itself rather than to the primary traumatic injury,23 which might raise concerns about the safe use of the catheter in the concomitant presence of traumatic brain injuries; an area for furthermore studies.25 26 61
In a meta-analysis addressing the incidence of complications of groin access after the use of REBOA, 13 studies with a total of 424 patients having REBOA were evaluated. There was an overall incidence of complications related to groin access equivalent to 4%–5%, including serious complications such as lower limb ischemia necessitating amputation in 2.1% of cases. Inserting the balloon catheter through the superficial femoral artery instead of the common femoral artery was a likely cause of such complications.77
Davidson et al assembled a list of complications encountered in high-volume REBOA users centers in a trial to recognize, mitigate, and manage anecdotal events. Among other complications, hepatic and renal failures were more particularly observed after prolonged inflation time in zone I.54
As the main aim of this review is to point at gaps in the knowledge, the following are recommendations for future studies and researches.
The literature remains deficient in regard to the best indication. Studies are needed to specify the subcategory of patients that will benefit the most from the balloon deployment.
A recommendation to have an update from the Aortic Occlusion for Resuscitation in Trauma and Acute care surgery registry58 after 3 years of the primary report is needed. It is important to include the high flux of articles coming from Japan.
Objective and transparent reports should be issued to validate the advantage of commercialized training courses versus peer-trained trends.24 50 51 Subgroup analysis of the level of expertise of the inserting person and whether training was acquired after a certified course or a peer-training process was not analyzed because of unavailability of such data in most articles reviewed.
Further studies are needed to define the role of REBOA in penetrating mechanism, especially with high-velocity missiles injuries.18 19 80
The 7-French and ultrasound-guided insertions are used more widely and becoming the standard of care. However, comparative studies are required for better validation of these results. Larger caliber catheters that require reconstructive vascular repair after removal are becoming obsolete.
More reports are showing the bridging use of REBOA as a damage control measure in complex pelvic injuries before shifting to invasive radiology suite. Follow-up studies are required to better define the advantage of use in these settings and perhaps incorporate it in the future pelvic fracture management algorithms and protocols.
The optimal occlusion time should be defined accurately in the context of trauma settings without extrapolation from the open elective aortic experience. Twenty minutes seems to be the golden number, after which, the catheter should be either removed or switched to the inflation–deflation mode, or the so-called temporary, intermittent, or ‘Partial’ REBOA. Another area of needed future studies.36 59
The innovative resuscitation with angiography percutaneous treatments and operative resuscitations in a hybrid room with simultaneous resuscitation, angiography, radiography, percutaneous therapies, and operating room capabilities seems to be the best place for the application of REBOA.81 However, further studies are needed to justify the cost and validate the expenses.
Finally, the issue of prehospital insertion should be approached with extreme caution.29 Even though the UK experience with London Helicopter Emergency Medical Service is very encouraging with remarkable reported improved survival,29 the modality and the results are not easily reproducible. Until further studies are conducted, it should be reserved for a selected type of cases in advanced centers with high expertise and a very well-defined postinsertion protocol.
Limitations
Scoping reviews are primarily descriptive in nature, and therefore quantitative data analyses have some limitations. First, it searched only the English language literature. As seen in the review, a significant number of publications originate from countries where the main language is not English, and articles in their native language could have been missed. Second, there was a limitation in contacting the authors for further information not found in their articles. Our initial standardized sheet included more than 30 variables, and it is difficult to capture these parameters in all articles. Nevertheless, conducting a prospective study design where all relevant items can be traced could be a solution.
Finally, we excluded the non-traumatic use of REBOA. A variety of studies showed its advantage as a life-saving measure especially in exsanguinating gastrointestinal or obstetrical cases.82 The main focus of our study was to highlight its use solely in trauma-related cases.
Conclusion
REBOA is bringing a definite welcomed addition to the armamentarium of the trauma surgeon and emergency room physicians. Whether it will stand the test of time and remain as an important adjunct to the resuscitation period is a question still to be answered. It is important to note that REBOA is not a permanent solution. It is rather a temporary hemodynamic stabilization measure of the patient in extremis until further definitive surgical management is applied.
There is a scarcity of high quality, prospective studies, which is impeding the ability to make evidence-based management decisions in this field. A collaborative effort is needed to identify the subtype of patients that will benefit the most from such a promising technique.
We analyzed the whole body of the current existing literature using a scoping review methodology and came out with recommendations to plan further research activities, highlighting potential gaps in the field and proposing research initiatives.
Acknowledgments
The authors would like to acknowledge the assistance of Mrs Tara Landry (Librarian at MUHC) for her remarkable help in the acquisition of the research material and to recognize the great support of the Montreal General Hospital Foundation, the McGill University Health Centre Emergency Medicine and Adult Trauma Programs.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
Footnotes
Collaborators Tara Landry (health research librarian at MUHC Library, University of McGill) for the help in the search strategy.
Contributors OB, TP, YBS and AB contributed to the project idea and the conceptual design of the review. OB, TP and YBS conducted the research. OB, AE and AB supervised the research. OB, TP and YBS conducted the literature review and the search strategy. OB and TP drafted the protocol. AE, JG, DD, PF, KK and TR contributed to editing and supervising of the research. All authors approved the final article. AB and TR are the guarantors of the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.