Article Text

Abstract
Background Traumatic brain injury (TBI) is an important cause of morbidity and mortality in low/middle-income countries. The objective was to assess causes and outcomes of unintentional and intentional TBI among patients presenting to a tertiary care hospital in Uganda.
Methods This study was conducted at Mulago National Referral Hospital, Kampala, Uganda, for 15 months in 2016–2017. Patients of all ages, males and females, presenting to the emergency department with suspected or documented TBI were enrolled. Patient demographics, TBI causes and outcomes were recorded. The outcome of interest was unintentional and intentional TBI.
Results Intent was known for 3749 patients, of these 69.7% were unintentional TBI and 30.3% were intentional TBI. The average age of patients in both groups was similar (28±14 years) with over 70% of patients between 19 and 45 years age group. About 80% were males in both groups. The main causes of unintentional TBI were road traffic injuries (RTI) (88.9%) and falls (11.1%). Pedestrians (42.1%) and motorcycle drivers (28.1%) were the most common road users. Among patients with unintentional TBI, about 43.6% were admitted, 34.0% were sent home. There were 73 deaths: 63 were patients with RTI and 10 had a fall. Although assault (97.1%) was the main cause of intentional TBI, those patients with self-harm were likely to be in severe Glasgow Coma Scale range (39.4%) compared with victims of assault (14.2%). Among patients with intentional TBI, 42.6% were admitted and 37.1% were sent home. There were 30 deaths: 29 were assault victims and 1 of self-harm.
Discussion Unintentional TBI caused by RTI and intentional TBI caused by assault are common among young males attending Mulago Hospital in Kampala.
Level of evidence Prospective observational study, level III.
- traumatic brain injury
- unintentional injury
- intentional injury
- trauma
- Uganda
- Africa
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Globally, traumatic brain injury (TBI) is an important cause of hospitalization, death and disability, disproportionality affecting people in low/middle-income countries (LMIC).1 2 TBI has both short-term and long-term implications for victims; and even a mild injury could lead to a lifelong disability.3 According to estimates by the WHO, about 10–69 million people across the world suffer from all-cause TBI. This wide range is possibly due to differences in data sources used for estimates, thus emphasizing the need to have accurate measures for assessing TBI burden.2 4
Some of the important causes of TBI globally are road traffic injuries (RTI), falls and violence.4 5 Rapid motorization especially with two and three wheelers, urbanization, lack of safety for high-risk occupations like construction industry and increasing conflict and crisis situations have escalated the TBI burden in LMICs. TBI is found to be common among children and young adults. In addition, males are more predisposed to suffer from TBI compared with females due to higher risks for RTI and violence-related injuries.6
There is great variation in TBI incidence across various regions of the world. TBI incidence is found to be higher in sub-Saharan Africa (SSA) where TBI rates due to RTI and violence are reported to be 156 and 144 per 100 000, respectively. These rates are 1.5 and 3.3 times higher than the global rates for RTI and violence resulting in TBI. Similarly, rates of intracranial long-term injuries due to war, violence and other unintentional injuries are much higher in SSA compared with global rates.2
Uganda, an SSA country with a population of about 42 million, has over 80% living in rural areas.7 In Uganda between 1990 and 2016, deaths due to unintentional injuries increased by 48% and years lived with disability (YLD) also increased by 118%. Whereas transport injuries resulting in deaths increased by 103% and its YLD by 147%, intentional injuries leading to death also increased by 111% and YLD by 105%.8 These upward trends in mortality and disability are alarming for a country like Uganda.
In the face of an increasing injury burden, understanding the burden of TBI is crucial in planning and implementation of preventive interventions to reduce its incidence. However, evidence informed programming and policymaking are impeded by the scarcity of such data in Uganda despite efforts to establish trauma registries.9 10 The objective of this study was to assess the burden of unintentional and intentional TBI, their causes and outcomes among patients presenting to a tertiary care hospital in Kampala, Uganda. The ability to show the burden on the healthcare system is a first step in generating attention to this injury.
Methods
This prospective observational study was conducted at Mulago National Referral Hospital, Kampala, Uganda; the current analysis is based on the pilot data collection spanning over 15 months during 2016–2017. The hospital is the largest public sector, tertiary care hospital in the country.
Study setting and participants
Patients of all ages, males and females, presenting to the emergency department (ED) of the hospital with suspected or documented TBI were potential participants. TBI was evaluated based on a history of direct injury to the head, or a mechanism involving injuries to multiple body regions such as fall or RTIs or assault. Loss of consciousness after the injury was not a requirement for inclusion. Patients with no mechanism suggestive of head injury or TBI, or who had other reasons to have a depressed level of consciousness, such as those with meningitis, stroke or psychotropic medications were excluded from the study.
Enrollment
Eligible patients were enrolled in the ED after their initial assessment. Suspected patients of TBI, where a history was not available immediately, were logged and evaluated later for eligibility based on their in-depth assessment in the ED. Data were collected by designated ED staff members and covered ED round the clock, thus included all suspected patients of TBI during the study period. Oral informed consent was taken from all adult patients, assent from patients between 13 and 17 years of age and permission from the parents or guardians for all children under 13 years of age. Patients for whom consent, assent and/or parental permission could not be obtained were excluded.
Data collection and follow-up
Enrolled patients were followed until their discharge from the ED. Data were collected using an electronic hospital-based registry, Kampala internet-based Traumatic Brain Injury Registry, developed specifically for TBI; details on the development of this registry are given elsewhere.11 The registry includes data on patients’ demographics, place of residence (rural vs. urban), injury circumstances, prehospital care, hospital assessment and care, TBI causes, injury severity, and patient outcomes. Data on demographics, prehospital care and injury event were collected as soon as the patient was stabilized, whereas data related to ED outcome were collected at the time of patient discharge from the ED. Data collection was done by nursing staff who were trained specifically on TBI surveillance, care and outcomes, using android tablets with the mHealth-based app for the TBI registry. The data on tablets were submitted via secure networks to a secure server protected by limited access and strong password systems. The data received on the server were monitored by investigators for data quality and timeliness.
Outcome variable
The outcome of interest was the intent of injury among patients with TBI presenting to the ED of Mulago Hospital. Other variables included in the analysis were patient characteristics such as age, sex, area of residence, marital status, and education level. Differences in TBI event characteristics for unintentional and intentional injuries were analyzed for cause and type of injury, care received prior Mulago Hospital, mode of arrival to Mulago, and ED discharge status.
Statistical analysis
For the analysis, age was categorized into three groups: 0–18 years, 19–45 years and >45 years based on the age distribution of enrolled patients. TBI severity was assessed based on the Glasgow Coma Scale (GCS) and categorized into mild, moderate and severe. The Kampala Trauma Score (KTS) was also calculated based on age, number of serious injuries, systolic blood pressure, respiratory rate and neurological status. This score has been previously validated in the Ugandan setting.12 Descriptive analysis was run on data related to patient demographics and clinical characteristics, causes of TBI and ED outcome. χ2 test of association was used for categorical variables whereas t-test was done for continuous variables.13 14 Simple and multivariable logistic regression was conducted with <0.05 level of significance to analyze factors associated with intentionality of TBI.15 The independent variables considered include age group, sex, area of residence, marital status, education level, whether patient is a breadwinner or not, mode of arrival to the hospital, type of head injury, KTS, GCS category on arrival to the hospital, and ED outcomes. Data were analyzed using STATA V.14.16
Results
During the study period, a total of 4735 patients were eligible for enrollment (figure 1). Out of these, 3944 (83.3%) were enrolled into the study. Seven hundred and ninety-one patients were excluded because they did not fulfill the inclusion criteria or did not give consent or assent or parental permission. Out of 3944 enrolled patients, the intent of TBI was known for 3749 (95.1%); analysis in this study is therefore limited to these 3749 patients (figure 1). Of these, 2614 (69.7%) patients were of unintentional TBI and 1135 (30.3%) were of intentional TBI.

Flow chart of patient enrollment for Kampala internet-based Traumatic Brain Injury Registry (KiTBIR). TBI, traumatic brain injury.
Patient demographics
There was no statistical difference between the unintentional and intentional TBI groups except for mode of arrival to Mulago Hospital (table 1). Two-thirds of patients with unintentional TBI were brought to the ED by private vehicles (31.3%) and ambulances (31.1%), however, about 48.5% of patients with intentional TBI were brought by police vehicles (table 1). The average age of patients in both groups was similar, with over 70% of patients between 19 and 45 years age group. More than 80% were males, with a little over 50% coming from urban settings. The proportion of single and married patients was almost similar in both groups. Over 50% had received primary education in both groups and more than 60% were breadwinners of their families (table 1).
Demographic characteristics of patients with traumatic brain injury (n=3749)
Unintentional TBI
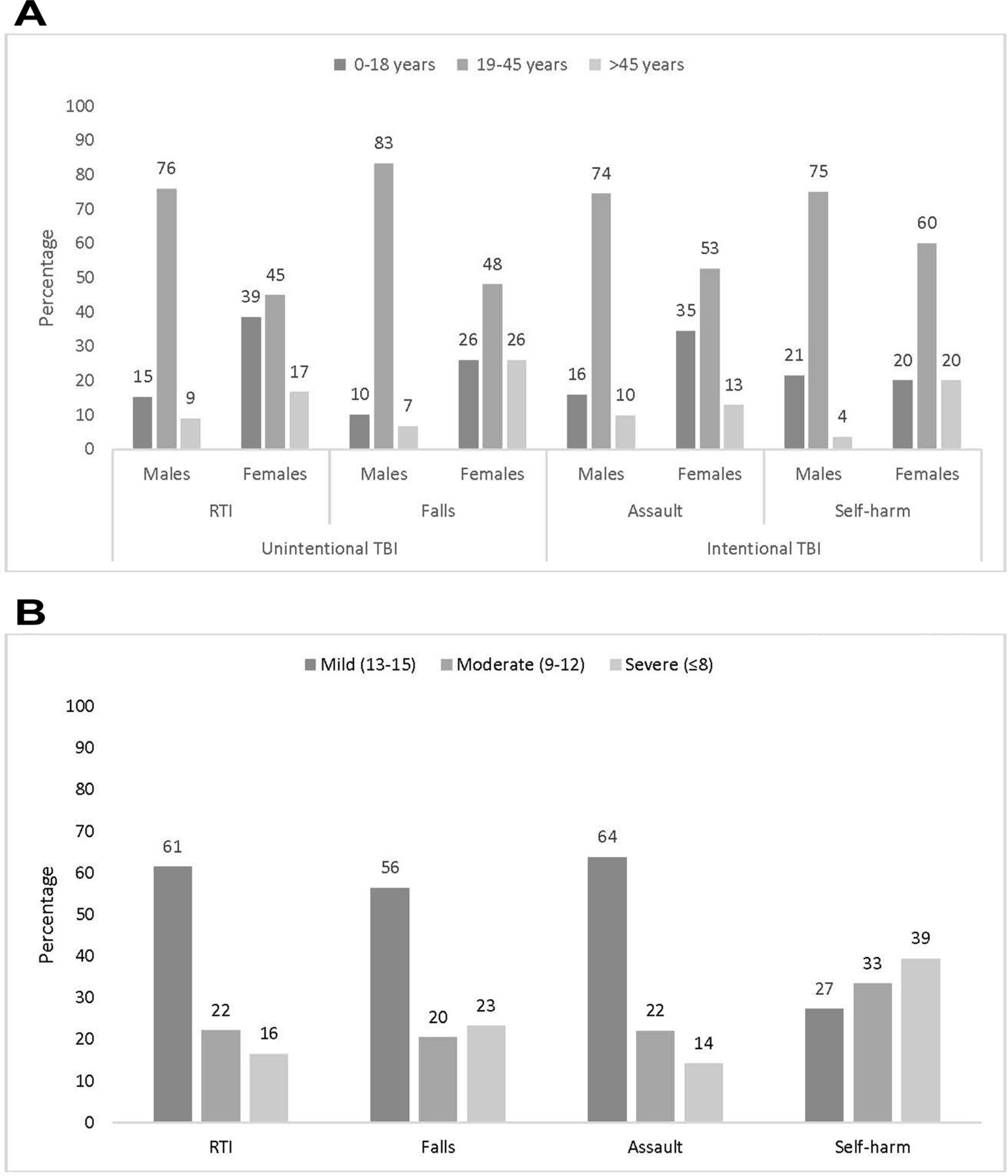
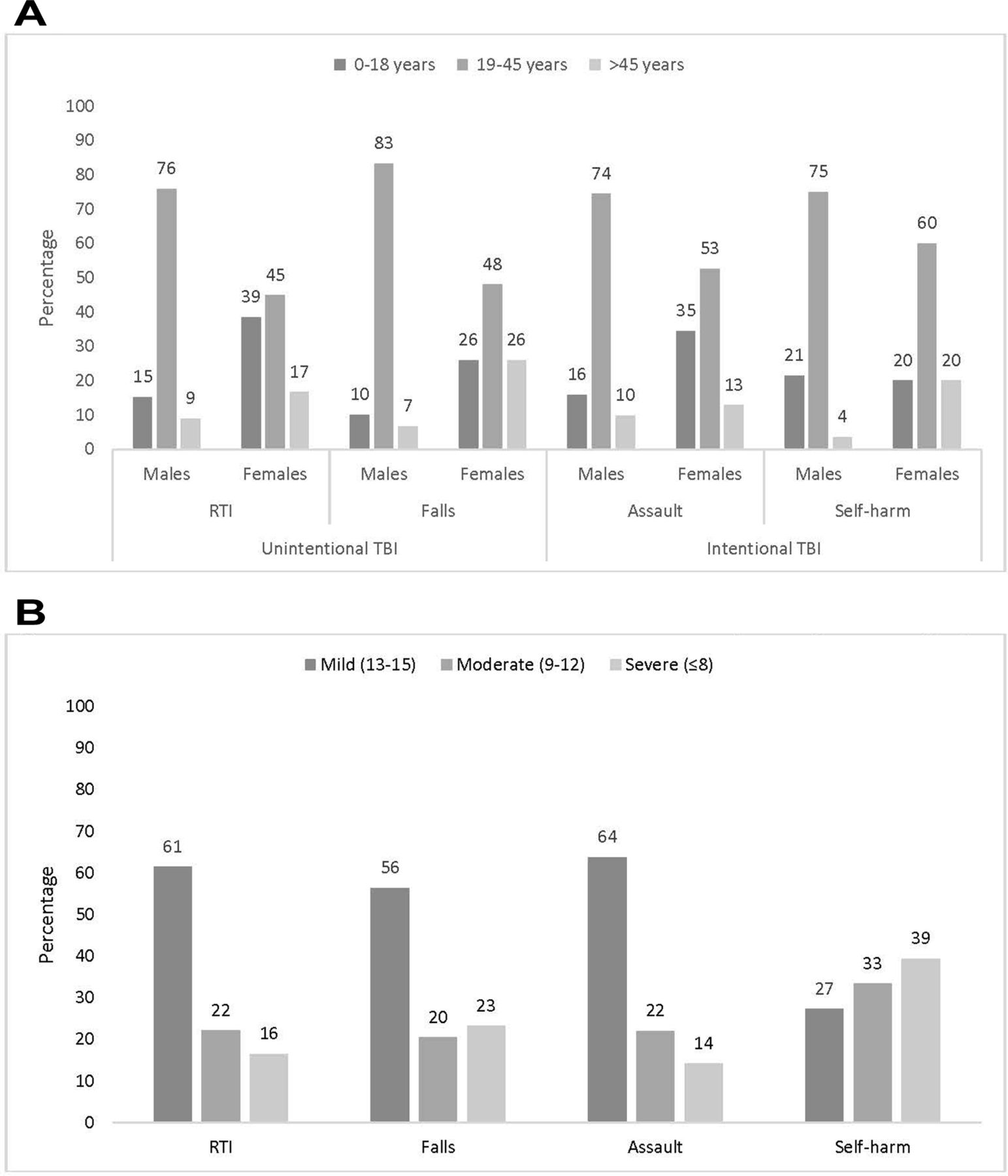
The majority of patients in this category were in 19–45 years age group (figure 2A). RTI (88.9%) was the main cause of unintentional TBI. Among patients with unintentional TBI who had an RTI, most victims were vulnerable road users, including pedestrians (42.1%) and motorcycle drivers (28.1%) across all age groups. These patients were hit by cars (46.9%) and boda-bodas (motorcycle taxi) (34.6%). Only a small proportion of patients with RTI used a helmet (16%) or wore seat belts (12.2%) at the time of the crash. A significant proportion of patients with TBI with fall-related injuries fell from a height of ≥3 m (41.8%) across all age groups. Around 33.7% had a fall from a height of <3 m.
{kind=link}
{kind=link}
(A) Causes of unintentional and intentional traumatic brain injuries (TBI) by sex and age groups. (B) Causes of unintentional and intentional traumatic brain injuries by Glasgow Coma Scale (GCS) category. RTI, road traffic injury.
Around 16.5% of patients with RTI and 23.2% of fall patients had a GCS score below 8 (p<0.001) (figure 2B). The KTS category was noted to be severe for 5.3% of patients with RTI and 8.7% of fall patients (p<0.001). About 43.6% of the patients were admitted for inpatient care and 34.0% were sent home (p=0.387). There were 73 deaths: 63 from RTI and 10 from fall injury (table 2).
Clinical characteristics of patients with traumatic brain injury (n=3749)
Intentional TBI
Like unintentional injuries, the majority in this category were between 19 and 45 years age group (figure 2A). Assault (97.1%) was the main cause of intentional TBI. Common assault methods were use of bodily force (33.7%), iron bar (24.2%) and hammer (12.0%). Firearms were extremely uncommon, documented in only three patients.
About 63.8% of assault patients were in mild GCS category, 22.1% in moderate and 14.2% were in severe category. Patients with TBI with deliberate self-harm were likely to be in the severe GCS category (39.4%) compared with victims of assault (14.2%) (p<0.001) (figure 2B). The KTS category was also noted to be severe for 3.1% of assault patients (p<0.001). About 42.6% of patients were admitted for inpatient care and 37.1% were sent home (p=0.387). There were 30 deaths: 29 were assault victims and 1 was a suicide (table 2).
Multivariate analysis
Comparing between patients with unintentional and intentional TBI, multivariate logistic regression showed statistically significant differences in the mode of arrival and severity of injury measured by KTS category. Controlling for other covariates, the odds of arriving by motorcycle taxi (compared with private vehicles) were 1.55 times greater for individuals with intentional TBI compared with patients with unintentional TBI. Meanwhile, adjusted odds of being transported in a police vehicle were 2.36 times greater for patients with intentional TBI compared with unintentional TBI. The adjusted odds of being in severe category of KTS were 45% lower in patients with unintentional TBI.
Although other independent variables in the model did not show statistically significant association, it was interesting to note that the adjusted odds of unintentional TBI were 10% lower in 19–45 years age group and 14% lower in >45 years old compared with ≤18 years old age group. Patients with unintentional TBI were 12% more likely to be married compared with those who were single (p=0.208). Individuals with unintentional TBI were more likely to be in mild GCS category compared with those with intentional TBI (moderate adjusted OR (aOR): 0.97 and severe aOR: 0.86). Individuals with unintentional TBI were more likely to be discharged from the ED compared with those with intentional TBI. The adjusted odds of admission were 0.88 compared with being discharged home (table 3).
Association of intent of traumatic brain injury with patient demographic and clinical characteristics*
Discussion
These prospective data from a hospital-based registry provide insight into risk factors and outcomes associated with intent of TBI in urban Uganda. TBI affects young males, and most risk factors including age, sex, education, area of residence and ED outcomes are comparable between two groups. A significant difference was found between mode of arrival to ED and intent of TBI, where police are more likely to transport individuals with intentional TBI to the hospital. The study also showed that RTI and falls are main causes of unintentional TBI whereas assault makes up most of intentional TBI. Although RTI and falls have been previously listed as main causes of TBI in Uganda, this study highlights the burden of ED visits associated with TBI associated secondary to assault and deliberate self-harm.17–22
RTI is an important cause of unintentional TBI among young males in Kampala. The majority of TBI victims were vulnerable road users including pedestrians and motorcycle riders who share the same road space with motorized vehicles. In a country where road infrastructure is rapidly growing, road designs must support easy and risk-free mobility of pedestrians and consider designated pedestrian crossing for pedestrians.23 24 In addition, interventions for road safety such as enforcement to control speeding, promotion of helmet wearing, and seat belt use may require urgent attention. Uganda does have a helmet law applicable to drivers and passengers, but the law does not require fastening of the helmet and there is lack of enforcement of the law.25
A third of all patients with TBI sustained intentional injuries. These violent assaults threaten the physical health and long-term outcomes of victims, and reflect on society and social issues. The near absence of firearm injuries in this hospital population could be an indicator of the low incidence of firearm assaults in the community, but it might also be because most such injuries result in fatalities before patients are able to access care, especially in a setting where prehospital care is largely lacking. It has been reported that intentional TBI results in high injury severity along with higher burden on caregivers.26–28 TBI can cause physical, cognitive, and behavioral or emotional impairments.29 30 These consequences are further worsened given fragile health systems in LMICs like Uganda where lack of appropriate and timely care, and scarce resources for management of such patients are challenging.2
During the past two decades, despite improvement in healthcare systems across the world, mortality associated with TBI remains at 30% to 35%.31–33 This has consequences for LMICs like Uganda.18 20 This is crucial for developing preventive programs that focus on primary prevention within communities as well as for secondary and tertiary prevention to reduce mortality and disability associated with TBI in LMICs. There is a need for further exploration of risk factors like use of alcohol, substance abuse among youth, and family cohesion in the country to avoid consequences of intentional injuries.3 34 It is essential to develop programs to engage youth in productive activities for contribution towards country’s economic development.35 Positive youth development programs have shown promising results through holistic approach involving identification of problem, skill building, developing healthy relationships with peers and community, and supporting youth as a key stakeholder by giving them voice and opportunities for personal, professional and economic growth and development.36 Such programs can be developed for TBI prevention at community level.
Another important finding in the study was the role of police in transportation of individuals with intentional TBI to the hospital for further care. This is an opportunity to assess their role as first responders and development of skills required to integrate police into the trauma care system within Uganda. As first responders, they can be provided with first aid training which may impact patient outcome and injury severity.37 Although police in high-income countries (HICs) have been trained to provide basic life support and perform life-saving interventions, such a training is lacking at national and subnational levels in Uganda.38
One of the main strengths of the study is that it collected prospective data on a large number of patients with TBI seen in a tertiary care hospital. This study was conducted in a tertiary care center; therefore, results are not reflective of burden of TBI in the community. The study highlights association between TBI intent and various patient demographic and clinical factors but it cannot assess temporality between outcome and independent variables due to nature of study design. Future studies need to focus on patient outcomes and recovery patterns once they are discharged from the hospital. The intent of TBI was documented based on what patients and their guardian reported. It was not possible to analyze the true intent of TBI, thus intentional TBI may be under-reported in this study. Although data on intent were available for 95% of the patients, there was no mechanism in place to explore TBI intent in 5% of the patients for which no intent was documented. It cannot be concluded whether these data were missing at random or were associated with intent of TBI itself.
Conclusion
This hospital-based registry provides insight into risk factors, causes and outcomes associated with intent of TBI in Uganda. Being young and male is an important risk factor for TBI in urban Uganda. RTI for unintentional TBI and assault for intentional TBI are the main causes. Although there was no significant difference in outcomes in the two groups, severity of injury as assessed by KTS was more among patients of intentional TBI.
Acknowledgments
The authors acknowledge the data collection team and staff at the Mulago Hospital, Kampala, Uganda, for their efforts during the data collection process and their valuable feedback related to the tool and data collection processes.
References
Footnotes
Presented at This work was presented at the 4th World Trauma Congress held in San Diego, CA, USA, from September 26–29, 2018.
Contributors NZ, AM, OK, HS and AAH were involved in the conception and design of the tool and the study. NZ conducted data analysis and wrote the first draft of the article. AM, RHN, HS, OK and AAH provided critical review. All authors revised the article critically for important intellectual content and approved the final version.
Funding The study was supported by grant (R21NS085094) to Johns Hopkins University under the Global Brain Disorders Research award of the Fogarty International Center at the US National Institutes of Health (NIH).
Disclaimer The funding agency had no role in study design, data collection, data analysis, data interpretation, or decision to submit this article for publication. The corresponding author has full access to all the data. The authors are solely responsible for the views mentioned in the article.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical review and approval for this study was taken from the Institutional Review Boards of the Johns Hopkins School of Public Health (USA), Makerere University School of Public Health (Uganda) and Uganda National Council.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data are available with the authors and any questions related to the data can be directed towards the corresponding author.
Author note AAH was based at the Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD, USA, at the time when study was conducted.