Article Text

Abstract
Background The postoperative outcomes of emergency general surgery patients can be fraught with uncertainty. Although surgical risk calculators exist to predict 30-day mortality, they are often of limited utility in preparing patients and families for immediate perioperative complications. Examination of trends in mortality after emergent colectomy may help inform complex perioperative decision-making. We hypothesized that risk factors could be identified to predict early mortality (before postoperative day 5) to inform operative decisions.
Methods This analysis was a retrospective cohort study using the American College of Surgeons National Surgical Quality Improvement Program database (2012–2014). Patients were stratified into three groups: early death (postoperative day 0–4), late death (postoperative day 5–30), and those who survived. Multivariable logistic regression was used to explore characteristics associated with early death. Kaplan-Meier models and Cox regression were used to further characterize their impact.
Results A total of 18 803 patients were analyzed. Overall 30-day mortality was 12.5% (3316); of these, 37.1% (899) were early deaths. The preoperative factors most predictive of early death were septic shock (OR 3.62, p<0.001), ventilator dependence (OR 2.81, p<0.001), and ascites (OR 1.63, p<0.001). Postoperative complications associated with early death included pulmonary embolism (OR 5.78, p<0.001), presence of new-onset or ongoing postoperative septic shock (OR 4.45, p<0.001) and new-onset renal failure (OR 1.89, p<0.001). Patients with both preoperative and postoperative shock had an overall mortality rate of 47% with over half of all deaths occurring in the early period.
Conclusions Nearly 40% of patients who die after emergent colon resection do so before postoperative day 5. Early mortality is heavily influenced by the presence of both preoperative and new or persistent postoperative septic shock. These results demonstrate important temporal trends of mortality, which may inform perioperative patient and family discussions and complex management decisions.
Level of evidence Level III. Study type: Prognostic.
- emergency general surgery
- colectomy
- inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Emergency general surgery (EGS) patients suffer worse outcomes as compared with their elective counterparts.1 Historically, surgeons have struggled to adequately communicate risk of complications or death to high-risk patients, particularly in situations that require emergency operations.2 3 Although surgical risk calculators exist, they are often of limited utility, particularly in determining which patients will suffer from serious and immediate postoperative complications.4–9 Identification of preoperative variables associated with high risk may aid both surgeons and patients when faced with urgent choices regarding preoperative decision-making. Likewise, identification of early postoperative variables associated with especially high risk may aid decision makers with realistic goals of care conversations.
This analysis sought to define variables associated with temporal trends after emergent surgery: those that resulted in early death versus late death. We hypothesized that by examining trends in mortality after emergency colectomy (a known high-risk procedure representative of the EGS population) we could identify both preoperative and early postoperative factors that lead to an increased risk of early death. We theorize that an understanding of this information will improve both preoperative and immediate postoperative decision-making, overall risk stratification, and communication between patients and providers.
Methods
Database
These data are analyzed from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) during a 3-year period (2012–2014). The NSQIP database is a peer-generated high-fidelity repository of over 200 preoperative, perioperative and postoperative variables of patients undergoing operations at participating institutions. The database tracks patient outcomes for a maximum of 30 days postoperatively.10
Variable definitions
Ascites is defined as the presence of any fluid accumulation in the peritoneal cavity prior to 30 days of the operation. Obesity is defined as body mass index >30. Wound complications are defined as any postoperative surgical site infection or dehiscence. Cardiac complications are defined as postoperative myocardial infarction or arrest. Respiratory complications are defined as the development of pneumonia, prolonged intubation (greater than 48 hours postoperative) or the occurrence of an unplanned reintubation. Bleeding complications are the transfusion of at least 1 unit of packed or whole red blood cells given from the surgical start until 72 hours postoperatively. Neurologic complications are defined as either postoperative stroke or coma. Renal complications are defined as development of progressive renal insufficiency or acute renal failure. The reoperation variable is defined as any unplanned reoperation within 30 days of the principal operative procedure. Sepsis complications are defined as postoperative sepsis or septic shock. Notably, NSQIP definitions of sepsis and septic shock differ from the most recently published guidelines. In this study, sepsis is defined as systemic inflammatory response syndrome (SIRS; temperature >38°C or <36°C, HR >90, RR >20 or PaCO2<32 mm Hg, white cell count >12 k x10^9/L or <4 k x10^9/L, anion gap acidosis) with the presence of positive blood cultures or other obvious signs of infection (purulence or positive fluid culture) while septic shock includes the above definition of sepsis coupled with ‘documented organ and/or circulatory dysfunction.’
Patient selection
Patients selected for analysis underwent emergent colectomy as defined by coding of the emergency variable (as reported by either surgeon or anesthesiologist) as well as coding of selected Current Procedural Terminology codes (online supplementary table 1). The selection of emergent colectomy as a representative operation was based on the fact that emergent colectomies constitute a large proportion of overall EGS Cases and are known to have high complication rates. Patients were excluded if they met the exclusion criteria of the database which include being <18 years of age, concurrent cases, cases for which variables were not included, and transplant or trauma patients.
Supplemental material
Data analysis
Patients were stratified into three groups: early death (postoperative day 0–4), late death (postoperative day 5–30), and those who survived. The definition of ‘early’ death (in-hospital death on hospital day 0–4) was determined based on the complication rates observed in our cohort. By day 5, more than half of the serious cardiac, respiratory, renal, and/or infectious complications have already occurred, thus making the 0–4 day time frame significant. Furthermore, and importantly, this definition of ‘early’ is consistent with other common conditions diagnosed in the intensive care unit, such as ‘early’ hospital acquired pneumonia. Accordingly, death from hospital day 0–4 was thought to be easily referenced and conceptualized by surgeons and other providers, as well as patients and family members. Categorical variables among the three groups were compared via percentages and the χ2 test.
Logistic regression modeling using patient, preoperative, and early postoperative variables was performed to determine independent risk factors for early death as compared with late death or survival. This modeling was performed in a backward fashion using an inclusion value of 0.1 and significance value of p<0.05. Adjusted multivariable Cox regression analysis was performed predicting death before postoperative day 5. Lastly, Kaplan-Meier plots demonstrating 30-day survival stratified by preoperative inflammation with 95% Hall-Wellner bands were constructed. Those suffering from preoperative sepsis or septic shock were considered to have shock postoperatively if postoperative sepsis or septic shock was also coded.
All data were analyzed using the SAS V.9.4 statistical software program (SAS Institute).
Results
A total of 18 803 patients were analyzed. The overall 30-day mortality was 12.5% (3316); and of those 37.1% (899) were early deaths. The time to death among the whole cohort at the 25th, 50th and 75th quartiles were postoperative days 2, 8 and 16, respectively. The percentage of overall death stratified by postoperative day is displayed in figure 1. Significant differences were present in the make-up of each cohort. The early group suffered from the highest proportion of inflammation; septic shock was present in almost 60% of these patients, and sepsis or SIRS criteria were present in an additional 25%. When compared directly with the late group, the early group also had high rates of preoperative ventilator dependence (37.0% vs. 20.2%, p<0.001) and end-stage renal disease (12.2% vs. 8.1%, p=0.001). Other patient and preoperative cohort characteristics are presented in table 1 and online supplementary tables I–III.
Patient variables and comorbidities stratified by time of death
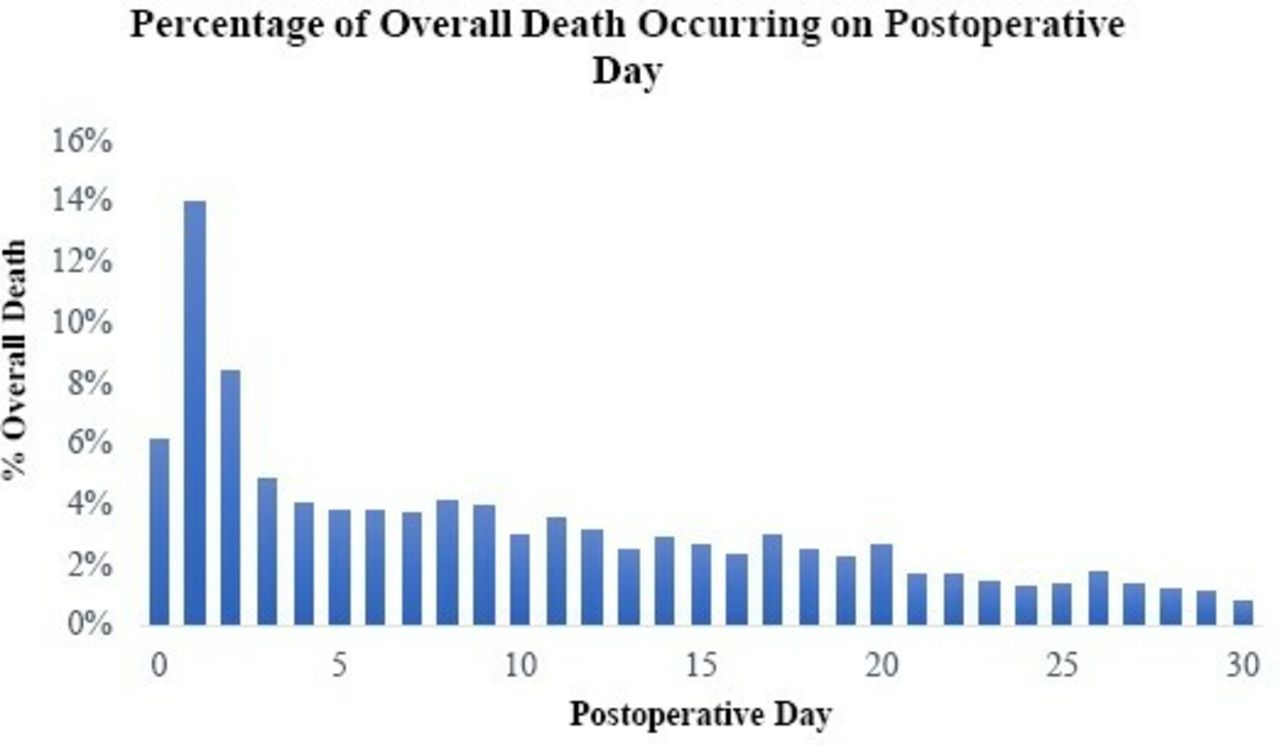
Percentage of overall death occurring on postoperative day. Shown is the percentage of death that occurred in the overall patient cohort stratified by postoperative day.
There were also significant differences in postoperative complications. Those suffering from early death were more likely to have cardiac complications (26.4% vs. 17.7% among those who died later and 2.1% among those who survived) and less likely to suffer from neurologic, respiratory or thromboembolic complications as compared with the other two cohorts. Other differences in postoperative and hospitalization characteristics are summarized in table 2 and online supplementary tables IV–VI.
Patient operative and postoperative characteristics stratified by time of death
Of the 2710 patients with preoperative septic shock, 52% continued to have shock in the early postoperative period. Those patients with both preoperative and postoperative shock had an overall mortality rate of 47% with over half of all deaths occurring in the early period.
Logistic regression modeling demonstrated several preoperative and postoperative variables independently associated with early death; these are summarized in table 3. Variables with significantly increased odds of early death versus later death or survival included age >80 (OR 3.42, p<0.001), preoperative septic shock (OR 3.62, p<0.001), new or persistent postoperative septic shock (4.45, p<0.001) and preoperative ventilator dependence (OR 2.81, p<0.001).
Logistic regression demonstrating characteristics associated with death before postoperative day 5
Multivariable Cox regression modeling likewise identified several significant preoperative and postoperative variables predictive of early death, including preoperative septic shock (HR 1.48, p<0.001), preoperative ventilator dependence (HR 1.41, p<0.001) and postoperative septic shock (HR 1.52, p<0.001).
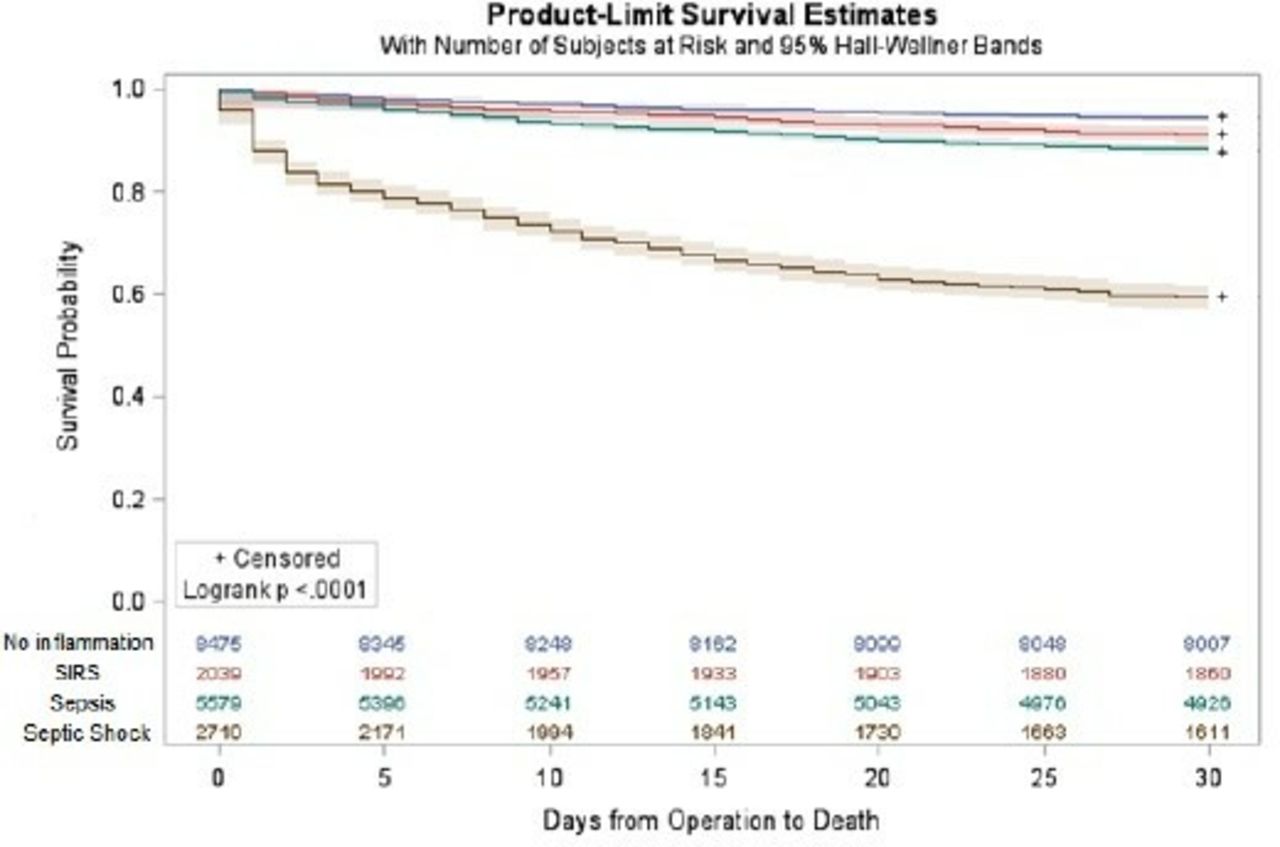
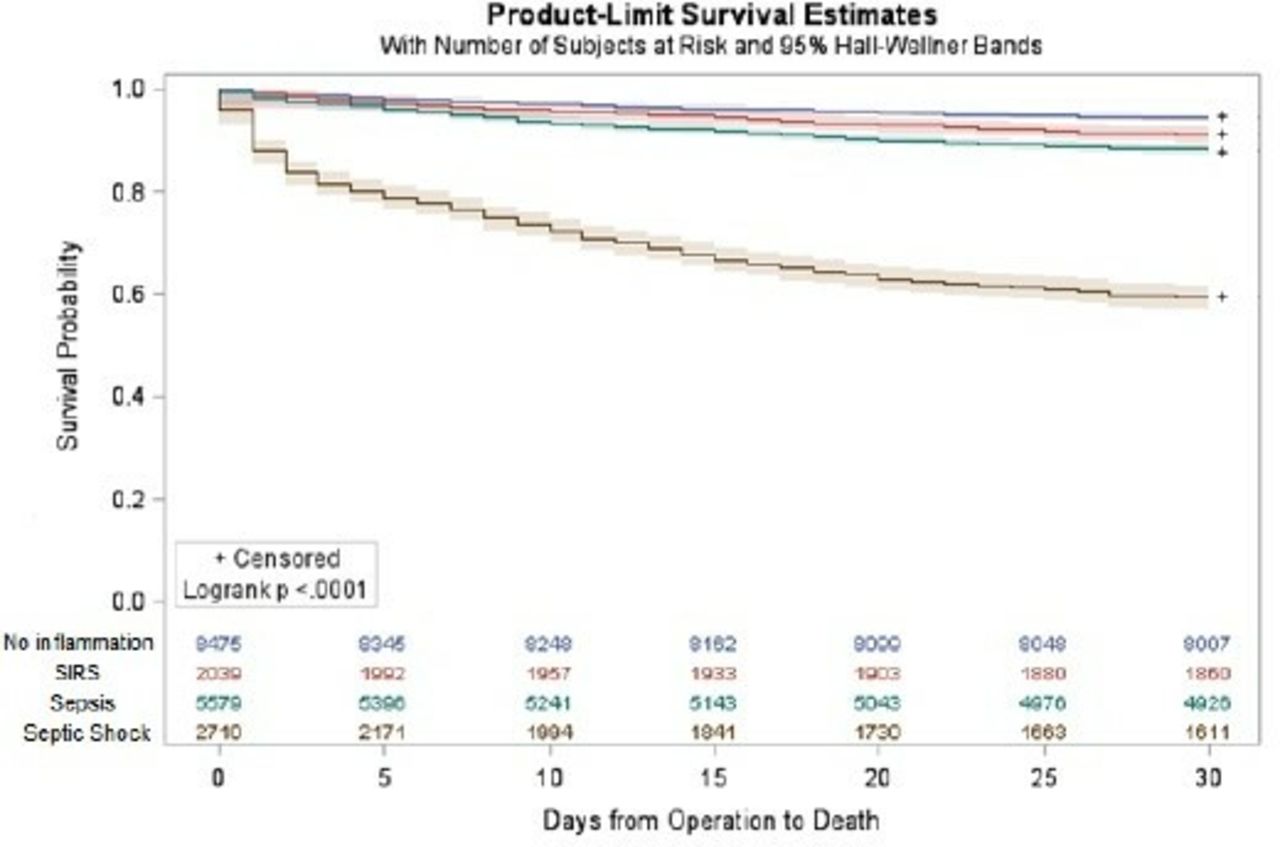
A Kaplan-Meier plot stratified by preoperative inflammatory state is demonstrated in figure 2 and shows early and significant effects on survival.
{kind=link}
{kind=link}
Kaplan-Meier plot stratified by preoperative inflammatory state. Shown are the Kaplan-Meier plots during the 30-day postoperative period stratified by respective inflammatory state: no inflammation, systemic inflammatory response syndrome (SIRS), sepsis and septic shock.
Discussion
Temporal trends exist throughout surgery and are important for their ability to inform operative decision-making. Understanding the timing of complications is an area that has received little study in the EGS population. This analysis used a large heterogeneous population undergoing EGS operations and identified several important preoperative and postoperative patient variables associated with early death. The novel definition of ‘early death,’ or before postoperative day 5, highlights a population suffering from rapid complications and mortality after surgery. The choice of postoperative day 5 is also thought to be reflective of a lack of operative success intended to be easily understood by both patient and provider alike.
Increased knowledge of preoperative and immediate postoperative variables associated with early death may prompt providers and family members to re-evaluate operative success and expected outcomes. If a patient is found to be at high risk for early death in the immediate postoperative period, this knowledge provides providers and families alike with an opportunity to clarify goals of care for a patient. The difficulty in making decisions for patients who are acutely ill and suffering from sepsis or septic shock in an intensive care setting is often compounded by the situation’s sudden and emotional nature.11 12 A lack of information or previous miscommunication regarding prognosis can further complicate these conversations. The results of this analysis provide an opportunity to fill in gaps or correct missing information to aid in treatment decisions. Conversely, this study may also be used in counseling patients and families who have suffered postoperative complications but do not appear to be at increased risk of early death to continue to pursue therapy rather than transition to more comfort-based care.
Specific preoperative variables associated with early death were identified in this analysis. Perioperative sepsis has long been demonstrated to be a cause of mortality after EGS operations and in this study preoperative septic shock and postoperative septic shock combined to be two of the largest predictors of early death. This is in contrast to the influence of sepsis alone, whose impact on early death was less than half that demonstrated by septic shock. The influence of preoperative sepsis and septic shock on postoperative outcomes is multifactorial and likely represents sequelae of tissue hypoperfusion.13 The results of this analysis suggest the existence of an early time point for some patients after which dysregulation of the inflammatory process is unlikely to be reversed by operative intervention or postoperative critical care. Although sepsis and septic shock were shown to be strongly associated with early death, careful interpretation and caution is warranted in applying these results directly to clinical scenarios. Future studies focused on arresting or mitigating the impact of sepsis and septic shock could use the parameter of early death to further explore the impact of intervention timing on outcomes.
Other drivers of inflammation were also implicated as contributors to early death in this study. Preoperative ventilator dependence has been demonstrated in many models to contribute to overall inflammation, and patients suffering from sepsis or septic shock often require mechanical ventilation due to arterial hypoxemia or inability to protect their airway due to cerebral hypoperfusion.14 15 Thus, ventilator dependence as both a product and cause of inflammation in part explains why requiring ventilator support prior to EGS operations was such a large predictor of early death. Similarly, severe medical comorbidities shown to increase risk for early death in this study, such as liver or renal failure, likely reflect reduced physiologic reserve available to combat the effects of sepsis and septic shock in the immediate postoperative period after EGS operations.
This analysis also isolated specific postoperative variables associated with early death, knowledge of which may aid decision makers in early goals of care discussions. A large proportion of patients in this study who entered the operating room in septic shock continued to suffer from septic shock postoperatively and subsequently suffered high mortality. The influence of septic shock on early death in this study demonstrates the importance of mitigating inflammatory dysregulation to improve patient outcomes and suggests a need to study interventions to achieve source control in this population. One such intervention that may improve outcomes in select populations is a damage control operation, a well-studied surgical technique that uses planned reoperation to arrest the cyclical nature of inflammatory mediated physiologic derangements to decrease mortality.16 17
This study brings to light the stark difference between patients undergoing emergent as opposed to elective colectomies. Operations done emergently are often done in the face of profound physiologic dysregulation due to systemic sepsis or septic shock.18 Patients rarely are able to benefit from preoperative risk stratification or optimization as opposed to their elective counterparts and are more likely to require more morbid operations performed under expedited circumstances. One solution that has arisen in the face of these challenges has been the advent of specialist Acute Care Surgery services that have demonstrated an ability to provide more timely care, improve patient outcomes, and benefit the overall health system from a cost perspective.19–22 This, combined with the known relationship between volume and outcomes in EGS, suggests that patients may benefit from early referral to centers that specialize in caring for these patients who are critically ill.23
This study has important limitations. Its retrospective nature subjects it to all the biases inherent in a study of its type. As it is drawn from a large heterogeneous national sample it is not known how individual hospital and provider practices have biased outcomes. Given the complexity of the clinical question, there is an opportunity to further investigate this question with newer statistical methodologies such as artificial intelligence.24 It is possible that the influence of sepsis and septic shock on mortality is secondary to centers failing to employ source control or damage control strategies. Likewise, we are unable to control for which patients, if any, received damage control operations or achieved adequate source control and how this information may have biased our conclusions. Equally likely to bias outcomes are differences in opinion regarding the appropriateness of operating on patients who suffer severe physiological derangement from preoperative sepsis and might be considered inappropriate surgical candidates at some centers. As this study employs a novel definition of early death that to our knowledge has not been employed elsewhere, we are unable to externally validate the results of our study with other risk calculators. There are many different possible criteria for defining early death and our novel definition, based in part on the timing of complication occurrence, may not represent the most effective definition for other operation types. This study cannot control for differing conceptualizations of surgical futility among providers or patients.25 26 To maintain the generalizability of this study and due to a lack of granularity regarding reasons for surgery, diagnosis codes were not included in this analysis. This is a further limitation of our study.
In conclusion, increased knowledge of contributors to early death in the EGS population potentially empowers patients, families and clinicians to make reasoned choices regarding the potential utility and expected outcome of large EGS operations. Death within 30 days is a standard outcome measure for postoperative mortality (eg, it is used by NSQIP). Based on the present analysis, risk of death within 5 days may also be a useful metric, especially as it relates to multiple perioperative decisions, for surgeons and families alike: offering an operation, establishing goals of care, and setting expectations.
References
Footnotes
Contributors MPDW, RDB: literature search, study design, data analysis, data interpretation, writing and critical revision. KAD, KMS, AAM: data analysis, data interpretation, writing and critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer American College of Surgeons NSQIP Disclaimer. The following disclaimer is required of all studies published using the NSQIP database as a data source: The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the American College of Surgeons NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open-access repository.