Article Text

Abstract
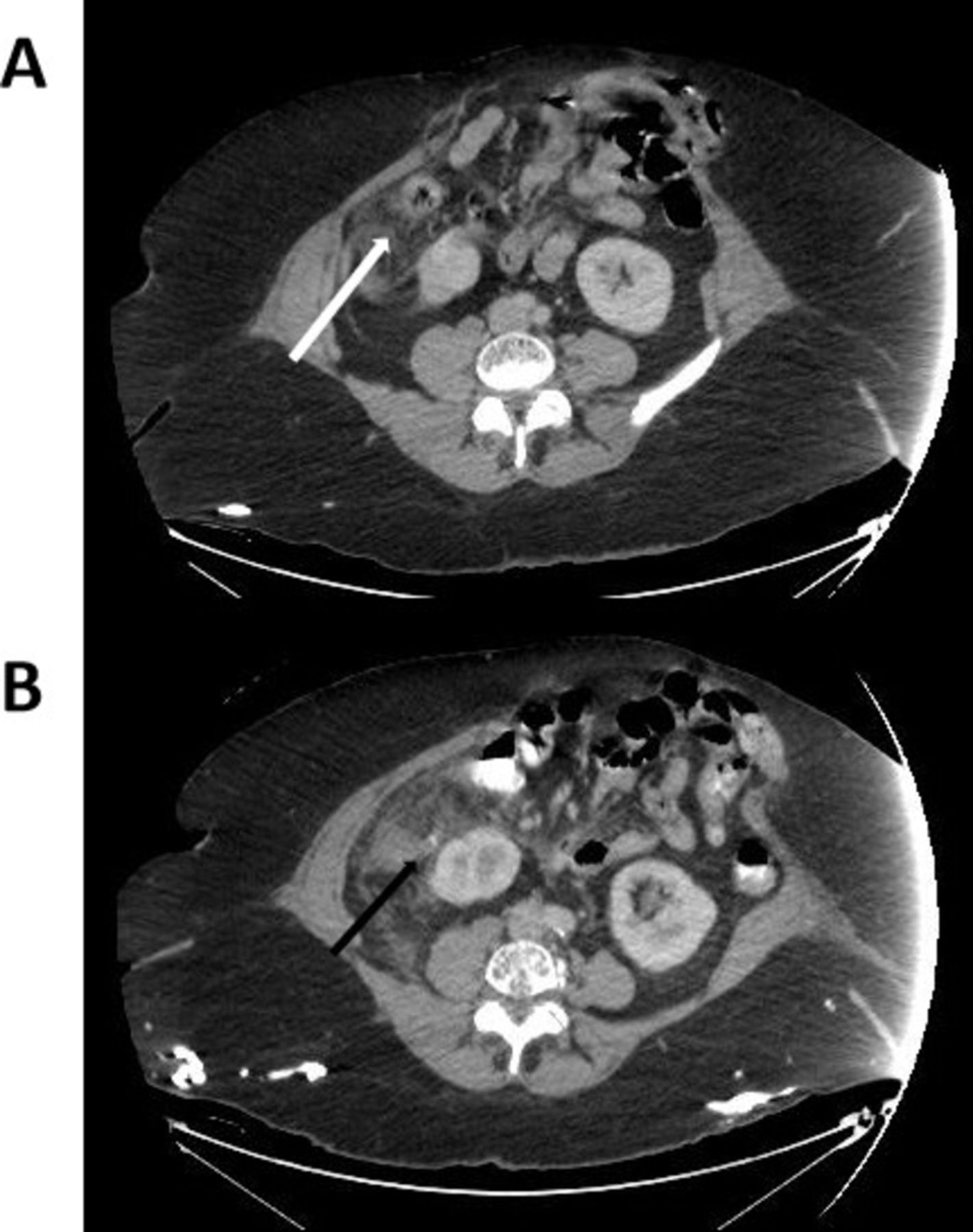
Case summary A 57-year-old woman with morbid obesity (body mass index [BMI] of 43), systemic lupus on steroids, type 2 insulin-dependent diabetes, peripheral vascular disease, unprovoked pulmonary embolism on rivaroxaban, and hypertension presented with 3 days of worsening abdominal pain and nausea. She had an extensive surgical history including a cesarean section, multiple laparotomies for small bowel obstructions (one complicated by bowel perforation requiring resection), and a double-barrelled ileostomy, which had been since reversed. As a result, she had a massive incisional hernia (figure 1). On presentation she was afebrile but tachycardic at 110 beats per minute. Physical examination revealed tenderness to deep palpation in the right upper and lower quadrants. CT demonstrated an 11 mm appendix with an appendicolith outside the hernia sac abutting the right kidney, discontinuity of the appendix tip, free fluid, and associated stranding in the subhepatic region (figure 2A). She was admitted to the surgical floor for a trial of conservative management with ancef and flagyl. On day 3, her pain worsened, her white cell count remained stable at 12 x109/L, her temperature was 37.8°C, she was not tachycardic, and a repeat CT showed a 15 mm perforated appendix with increased periappendiceal stranding and an associated small volume of free fluid. There was no phlegmon or organized abscess (figure 2B).

Patient’s abdomen demonstrating midline laparotomy incisional scar, previous ileostomy scar, and massive ventral hernia.

{kind=link}
{kind=link}
Abdominal CT showing increased stranding centered around the appendix, with discontinuity of the wall of the appendix tip and free fluid within the abdomen and pelvis. (A) Admission CT. White arrow: appendix. (B) CT on postadmit day 3 as patient worsened clinically. Black arrow: fecalith.
What would you do?
Continue non-operative management with broadened intravenous antibiotic coverage and bowel rest.
Laparoscopic ± open appendectomy without concomitant hernia repair.
Laparoscopic ± open appendectomy with abdominal wall reconstruction.
- Perforated appendicitis
- acute care surgery
- morbid obesity
- ventral hernia
- diabetes mellitus
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Footnotes
Contributors GS-G wrote the article and performed the required literature search. DG conceived of the idea for the topic and edited the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.