Article Text

Abstract
A 48-year-old man was admitted for medical management of recurrent Clostridium difficile (C-dif) colitis. One month prior to presentation, he underwent right thoracotomy and lower lobectomy for a carcinoid tumor at another hospital. His postoperative course was complicated by C-dif colitis, gastroesophageal reflux, and epigastric pain. He underwent two esophagogastroduodenoscopy (EGD) procedures demonstrating mild esophagitis on the first procedure, followed by a linear ulcer on the second procedure 2 weeks later. On hospital day 9 of his current admission, he developed an acute abdomen and underwent an urgent exploratory laparotomy for presumed fulminant colitis. Findings included a healthy-appearing colon with only moderate distension, so a loop ileostomy was created for antegrade colonic irrigation. Postoperatively, a chest X-ray demonstrated a tension-appearing left pleural effusion, prompting tube thoracostomy placement. Initial output was greater than 2L of thin dark-brown fluid. An esophagram demonstrated a distal esophageal perforation (EP) and EGD was performed. Two medium-sized EPs were identified which appeared to arise from chronic-appearing ulcerations, one at 39 cm and one at 45 cm from the incisors (figure 1). A single 19mm×100 mm EndoMAXX fully covered stent was placed. Video-assisted thoracoscopic (VATS) drainage of the left hemithorax was performed in addition to placement of a right tube thoracostomy. Due to continued high output from the left thoracostomy tube, the stent was exchanged for a longer 23mm×100mm EndoMAXX fully covered stent. The patient stabilized for several days but again developed worsened sepsis, with EGD demonstrating inadequate coverage of the proximal perforation.

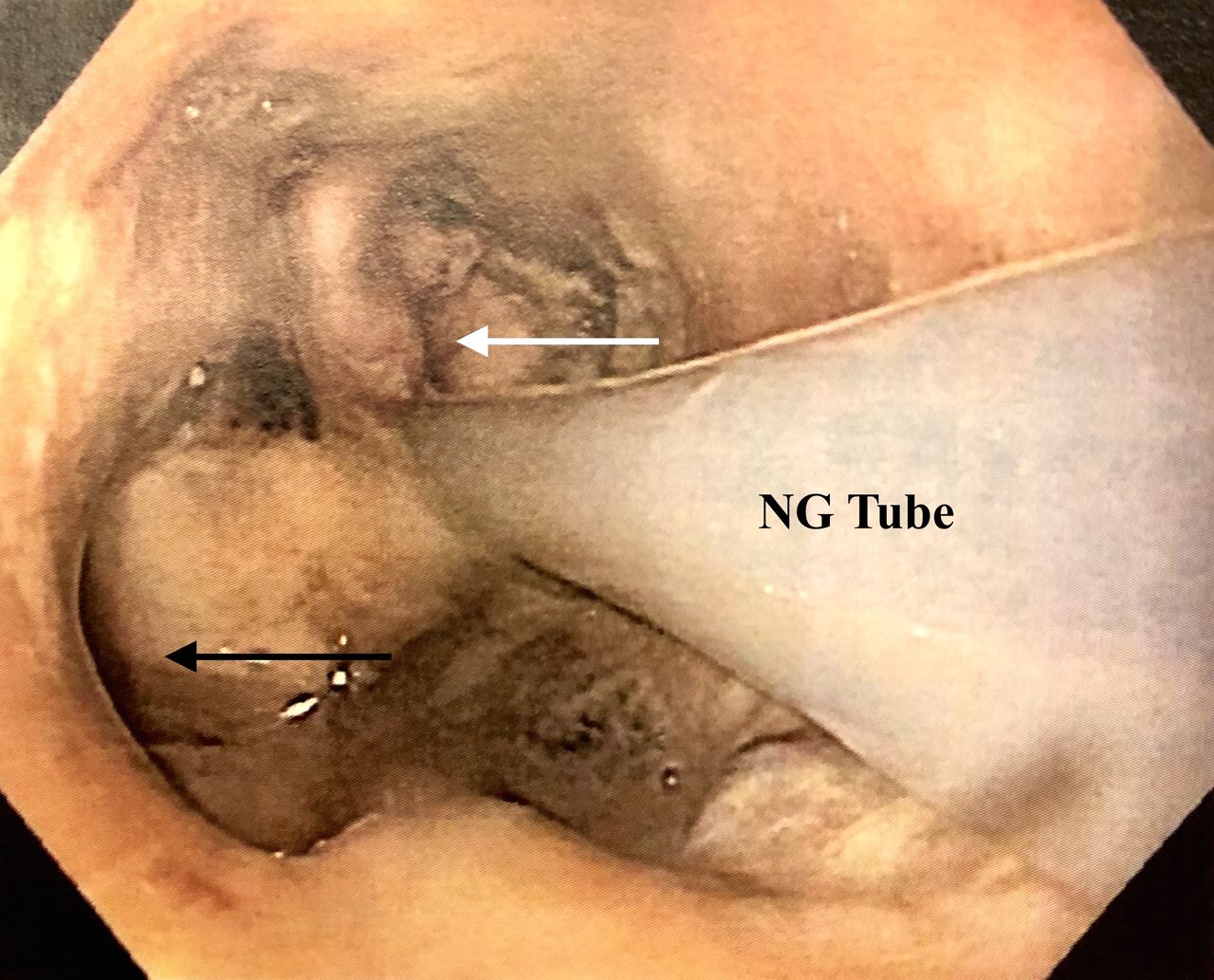
Endoscopic photograph showing left-sided esophageal perforation/fistula (black arrow). Gastroesophageal junction indicated by white arrow. NG, Nasogastric tube.
What would you have done?
Repeat esophageal stenting with wide drainage of the thoracic cavity.
Esophageal T-tube placement and wide drainage of the thoracic cavity.
Esophageal resection with gastrostomy drainage and proximal diversion.
Bilateral tube thoracostomies and antibiotic/antifungal therapy.
- esophageal perforation
- clostridium difficile
- stent
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What we did and why
Choice B
The esophageal stent was removed and a right VATS was performed. A 24-French T-tube was placed in the inferior mid-EP and externalized. The pleural space was irrigated and widely drained (figure 2). A re-exploration of his abdomen was performed and an 18-French Stamm gastrojejunostomy tube was placed. We attempted to mobilize his gastroesophageal junction for proximal gastric exclusion; however, adhesions from his recent exploratory laparotomy precluded adequate mobilization. The following day, a left thoracotomy was performed and a 24-French T-tube was placed in the lower thoracic EP just proximal to the gastroesophageal junction. The T-tube was secured to the diaphragm, externalized through the left chest, and the pleural space was irrigated and widely drained (figure 3). Intraoperative cultures of the pleural fluid grew Candida albicans, C. glabrata, and Serratia liquefaciens, which were treated with broad-spectrum intravenous antibiotic and antifungal therapy. A complicated postoperative course ensued, including reintubation, fluctuating vasopressor requirements, and development of a subsegmental pulmonary embolism requiring anticoagulation therapy. He developed an acute right hemothorax requiring packed red blood cell transfusion on hospital day 32. Additionally, he became more fatigued and frustrated with his oscillating clinical course and requested no further resuscitative efforts. He died on hospital day 35 after initiating comfort care measures.

Intraoperative photograph demonstrating the T-tube within the right mid-thoracic esophageal perforation (white arrow). The left-sided perforation was of similar size, quality and configuration.
{kind=link}
{kind=link}
{kind=link}
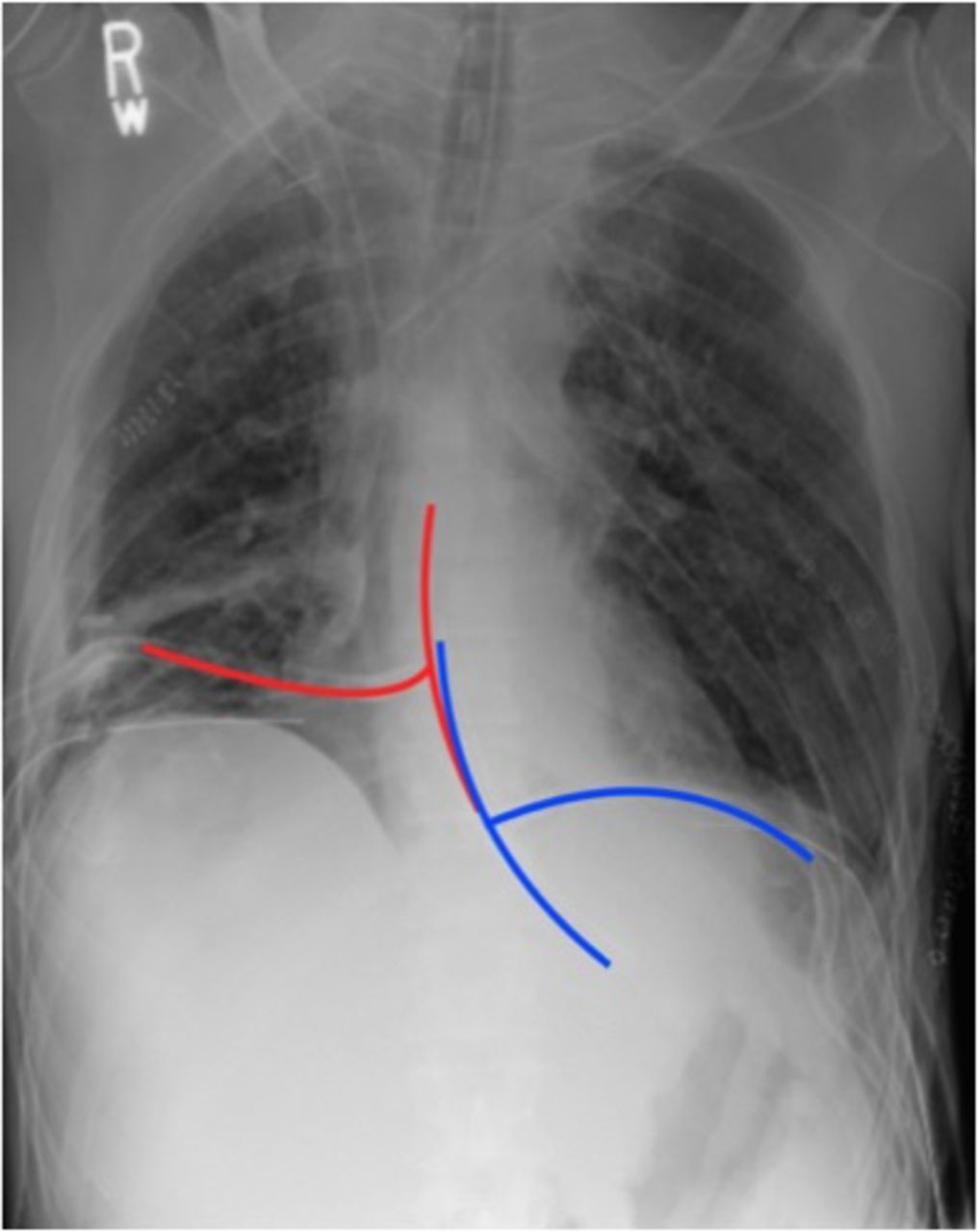
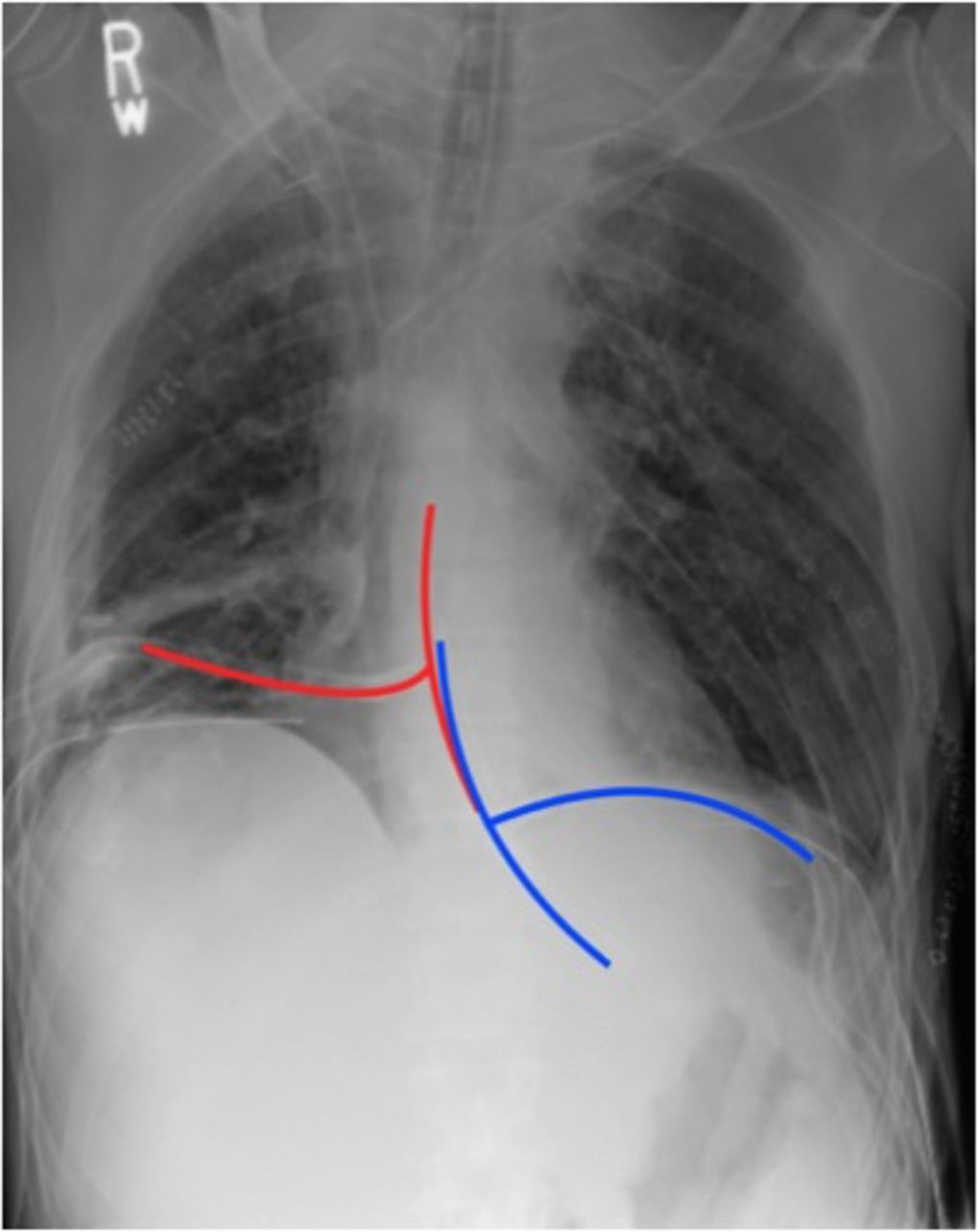
Postoperative chest X-ray demonstrating the right T-tube (red) and left T-tube (blue), and widely drained bilateral pleura spaces.
Our case demonstrates an atypical and uncommon presentation of two distal EP/fistulas of uncertain etiology and chronicity. The patient presented with significant weight loss (>20lbs, BMI 17 kg/m2) with evidence of malnutrition and recent EGD with several biopsies. Pathology from these biopsies did not reveal an explanation for the development of the EP/fistulas and it is unclear if the biopsy procedures themselves contributed to the esophageal injuries. Treatment algorithms for EP classically vary depending on chronicity with management of acute perforations favoring primary repair and chronic perforations managed through wide drainage of the pleural cavity. Treatment often includes a multimodal and multidisciplinary approach including surgeons, advanced endoscopists and intensivists. Esophageal stenting has become more widely utilized and is often an initial modality in the modern era for both acute and chronic perforations, providing a minimally invasive means of management with the intent of improved morbidity compared to surgical management. However, as demonstrated by our case, there is still a role for surgical management of EP, whether for salvage of failed stent therapy or as initial management. Despite the array of treatment options, morbidity and mortality from EP remains high and these patients often require prolonged organ support in an intensive care setting. An EP can present a significant clinical challenge, and an even larger challenge when more than one perforation exists.
Footnotes
Contributors DP and DS are the sole contributors of this submission.
Funding The authors have not declared a specific grant for this research from anyfunding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.