Article Text

Abstract
Background This study aimed to compare treatment outcomes between patients with severe pelvic fractures treated at a representative trauma center that was established in Korea since 2015 and matched cases treated in the USA.
Methods Two cohorts were selected from a single institution trauma database in South Korea (Ajou Trauma Data Bank (ATDB)) and the National Trauma Data Bank (NTDB) in the USA. Adult blunt trauma patients with a pelvic Abbreviated Injury Scale >3 were included. Patients were matched based on covariates that affect mortality rate using a 1:1 propensity score matching (PSM) approach. We compared differences in outcomes between the two groups, performed survival analysis for the cohort after PSM and identified factors associated with mortality. Lastly, we analyzed factors related to outcomes in the ATDB dataset comparing a period prior to the implementation of the trauma center according to US standards, an interim period and a postimplementation period.
Results After PSM, a total of 320 patients (160 in each cohort) were identified for comparison. Inhospital mortality was significantly higher in the ATDB cohort using χ2 test, but it was not statistically significant when using Kaplan-Meier survival curves and Cox regression analysis. Moreover, the mortality rate was similar comparing the NTDB cohort to ATDB data reflecting the post-trauma center establishment period. Older age, lower systolic blood pressure (SBP) and Glasgow Coma Scale (GCS) at admission were factors associated with mortality.
Discussion Mortality rate after severe pelvic fractures was significantly associated with older age, lower SBP and GCS scores at admission. Efforts to establish a trauma center in South Korea led to improvement in outcomes, which are comparable to those in US centers.
Level of evidence Level IV.
- pelvic fracture
- trauma systems and outcomes
- Outcome and comparison
- global surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Pelvic trauma occurs in only 3% of all skeletal injuries.1–3 However, mortality rates after severe pelvic fractures are high due to rapid exsanguination, difficult hemostasis, and presence of associated injuries.1–13 Therefore, a multidisciplinary approach is critical to treat such injuries; in particular, resuscitation, bleeding control, and the management of bone and associated injuries should occur simultaneously and as early as possible after the injury. Severe pelvic fractures should always be subjected to an integrated multidisciplinary management strategy led by trauma surgeons, but also including orthopedic surgeons, interventional radiologists, anesthesiologists, critical care physicians, and urologists.13–15 However, in developing countries where trauma systems are not well established, a multidisciplinary approach is difficult to implement, and patient outcomes after severe pelvic fractures are likely inferior when compared with countries with established trauma systems.
South Korea is a developing country with a reported preventable trauma death rate approaching 30%.16 17 The South Korean government announced in 2012 the establishment of a trauma system by designating 17 regional trauma centers across the country. Currently, there have been no reports on outcomes after the creation of the nationwide trauma system.18 19 Moreover, no specific guidelines for the management of complex injuries such as severe pelvic fractures exist. Ajou University Medical Center (AUMC) created the Division of Trauma Surgery in 2010, which includes a dedicated group of trauma surgeons providing care to trauma patients following the American College of Surgeons’ Committee on Trauma (ACSCOT) guidelines. The Division of Trauma Surgery was created prior to the government’s plan to establish a nationwide trauma system.20 The institution has been receiving increased human resources and equipment as well as financial support from the South Korean government since 2013, and it has been able to fully manage all trauma patients transported to the facility since 2015. Therefore, AUMC is well known as one of the leading hospitals in the treatment of patients with severe pelvic fractures in South Korea. However, thus far, the trauma center’s performance and its outcomes have not undergone an in-depth assessment.
In this study, we analyzed the outcomes of two cohorts of patients with severe pelvic fractures comparing the Ajou Trauma Data Bank (ATDB) to the ACSCOT National Trauma Data Bank (NTDB). Survival analysis was performed to analyze risk factors associated with outcomes. Additionally, we analyzed the effect of the implementation and establishment of the trauma center at AUMC on outcomes.
Methods
Data
We designed two cohorts to analyze the outcomes of patients with severe pelvic trauma: patients included in the ATDB between 2010 and 2016 and those included in the NTDB between 2010 and 2014.
AUMC is a leading teaching hospital that has been running a trauma center that is equivalent to a level I trauma center in the USA since 2015; it covers a population of approximately 7 million residents in the southern area of the Gyeonggi province in South Korea. Annually, more than 2000 trauma patients and 500 major trauma patients with an Injury Severity Score (ISS) >15 are hospitalized at the hospital.
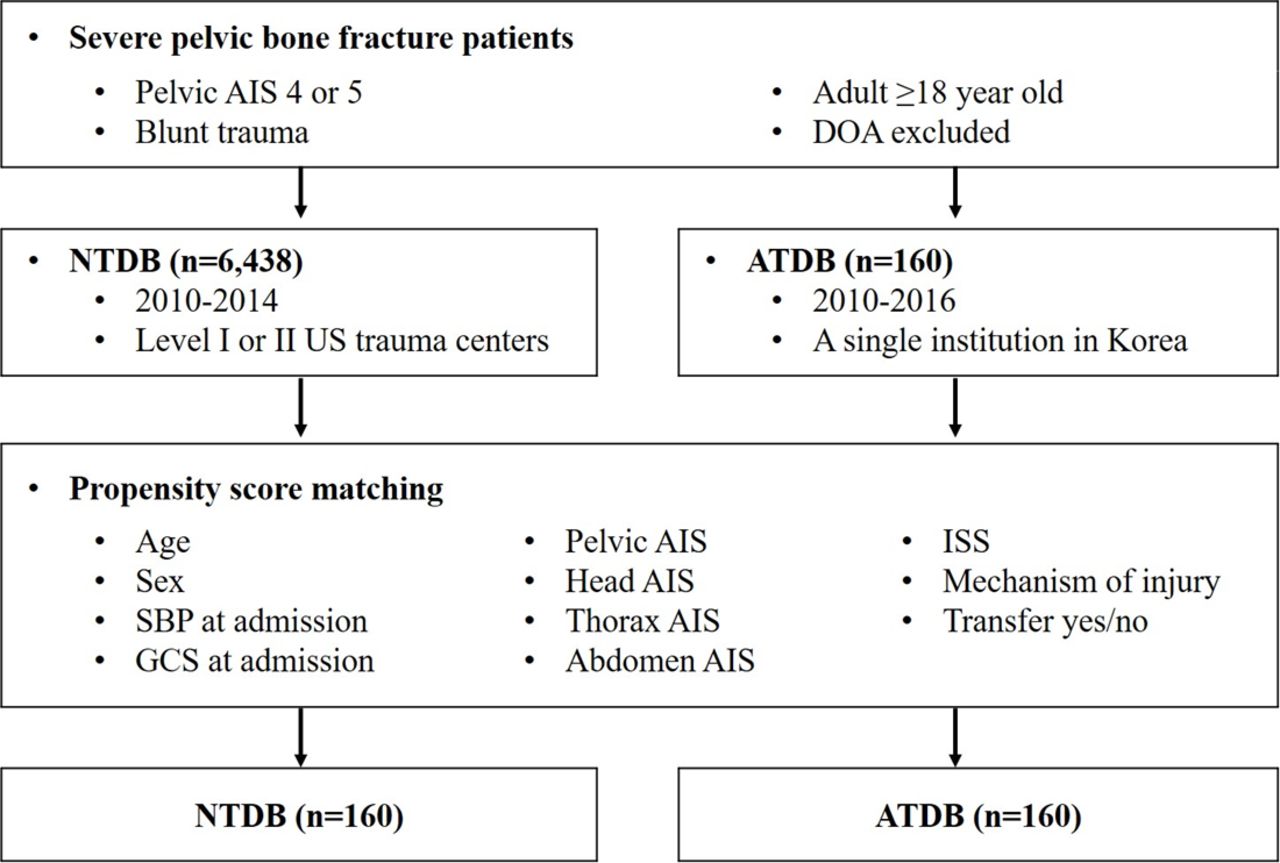
We evaluated 14 000 and 110 000 patients from the ATDB and NTDB, respectively, for inclusion in the study. After excluding cases deemed ‘dead on arrival’, we included patients aged ≥18 years, with a blunt mechanism of injury, and a pelvic Abbreviated Injury Scale (AIS) >3. A total of 6438 and 160 patients from the NTDB and ATDB were included in the final study, respectively, before matching (figure 1).

Flow chart of the study design. AIS, Abbreviated Injury Scale; ATDB, Ajou Trauma Data Bank; DOA, death on arrival; ISS, Injury Severity Score; GCS, Glasgow Coma Scale; NTDB, National Trauma Data Bank; SBP, systolic blood pressure.
Statistical analysis
We matched patients based on covariates that are known to affect outcomes after severe injury. Those included age, sex, systolic blood pressure (SBP) at admission, Glasgow Coma Scale (GCS) at admission, mechanism of injury, transfer status (yes/no), ISS and pelvic, head, thorax and abdomen AIS. Logistic regression was used to calculate the propensity scores of these covariates in patients of the ATDB (n=160) and NTDB (n=6438) cohorts. We then conducted a 1:1 propensity score matching (PSM) with the minimum distance method for the ATDB and NTDB cohorts (n=160 for each, with total of 320 research subject; figure 1). The standardized differences in the covariates between the two groups were calculated before and after matching to validate the PSM procedure.
We compared differences in hospital length of stay (LOS), intensive care unit (ICU) LOS, days on the ventilator and in-hospital mortality between the two datasets before and after matching using the Mann-Whitney U and χ2 tests. Thirty-day survival rates were compared using Kaplan-Meier plots. Furthermore, we analyzed survivors and non-survivors after PSM matching and identified factors associated with mortality.
After adjusting for confounding factors that could affect in-hospital mortality, a Cox regression model was used to analyze the effect of the treatment institution comparing both datasets (ATDB vs. NTDB) on outcomes. First, we conducted a univariate Cox regression analysis using 11 variables (excluding mechanism of injury and including the dataset variable). All 11 variables were included in the multivariate Cox regression analysis because they were all significantly associated with mortality in the univariate model (p<0.1) except for the dataset variable (p=0.194).
Lastly, we analyzed factors related to outcomes in the ATDB cohort comparing three periods of time related to the creation and establishment of the trauma center (pre-establishment, interim establishment and post-establishment). All continuous and categorical variables were compared using the Kruskal-Wallis or χ2 tests.
All statistical analyses were performed with SPSS, V.23, and p<0.05 was considered significant.
Results
The median age of patients in the ATDB (n=160; 58.1% men) and NTDB (n=6438; 64.6% men) cohorts were 48.5 years (IQR: 35–61) and 46 years (29–46), respectively. Before PSM, all potential confounding variables were significantly different between the ATDB and NTDB cohorts except for sex (p=0.093) and thorax AIS (p=0.665). After PSM, there were no significant differences between the two groups (table 1). When we calculated the standardized differences of the covariates, all except for age and thorax AIS decreased after PSM. Therefore, and because the values for age (0.0067) and thorax AIS (0.0009) were very small, we considered the PSM adequate.21
Comparison of severe pelvic fracture patients between ATDB and NTDB before and after propensity score matching
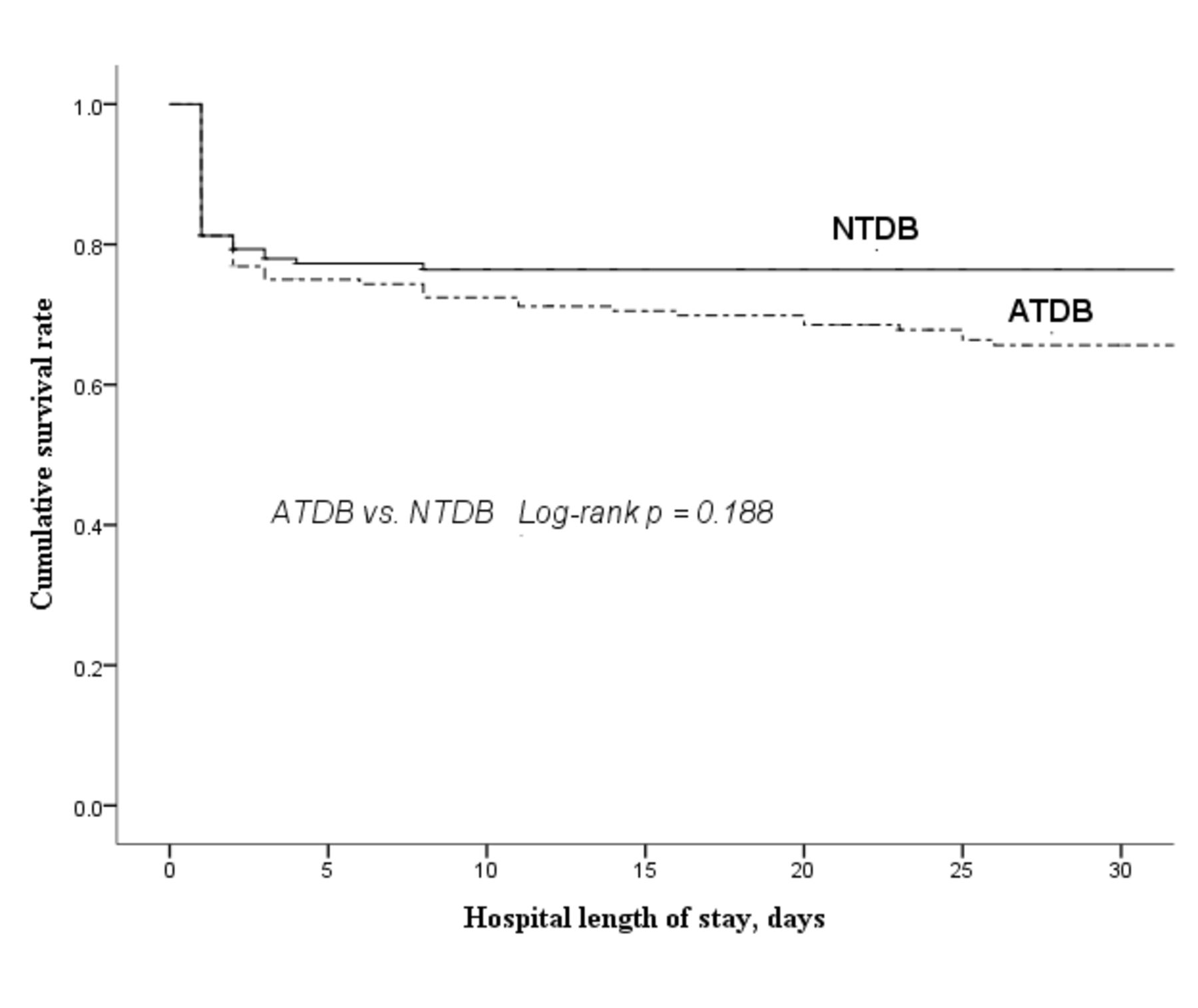
Patients in the ATDB cohort had a significantly higher mortality rate than that observed in the NTDB cohort; however, the difference decreased after matching (before PSM: 36.9% vs. 16.7%, respectively; p<0.001; after PSM: 36.95% vs. 23.1%, respectively; p=0.007). Before PSM, patients in the ATDB cohort had lower SBP and GCS at admission as well as a higher overall ISS (table 1). The Kaplan-Meier curve analysis showed that the 30-day cumulative survival rate was 1.2 times higher in the NTDB than in the ATDB cohort (76.9% vs. 63.1%, respectively); after matching, however, the difference was not statistically significant (log rank p=0.188; figure 2).

Kaplan-Meier curves of 30 day in-hospital mortality among patients with severe pelvic fracture from NTDB and ATDB. ATDB, Ajou Trauma Data Bank; NTDB, National Trauma Data Bank.
Comparing survivors with non-survivors, we found significant differences in all variables except for mechanism of injury (table 2). In the Cox regression analysis, patients’ age, SBP and GCS at admission were found to affect mortality with statistically significant adjusted HRs as follows: age: aHR=1.016, p=0.011, 95% CI 1.004 to 1.028; SBP at admission: aHR=0.986, p<0.001, 95% CI 0.981 to 0.992; and GCS at admission: aHR=0.887, p<0.001, 95% CI 0.838 to 0.938. Regarding the effect of the treatment institution (ATDB vs. NTDB), the aHR was borderline significant (p=0.054; table 3). As the log minus log curve for the two groups (ATDB and NTDB) showed a parallel pattern, we considered the Cox regression model as statistically appropriate for the analysis. According to the results of the Cox regression analysis, the interaction effect of the two groups had a p value of 0.077 and therefore could not be considered as changing the hazard function. This satisfied the proportional hazard assumption (data not shown).
Comparison between survivors and non-survivors after propensity score matching
Cox regression analysis of risk factors associated with mortality in patients with severe pelvic fractures
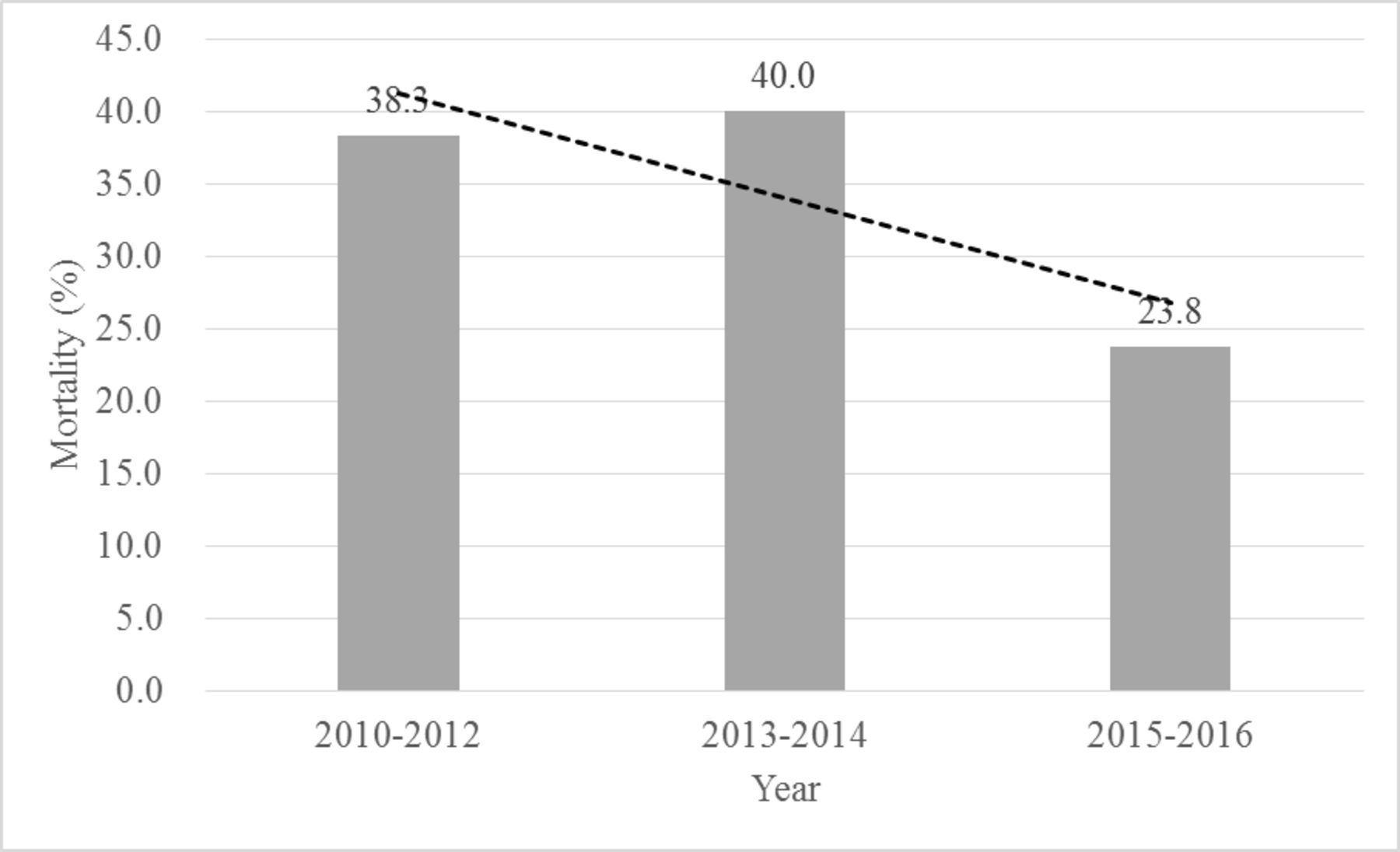
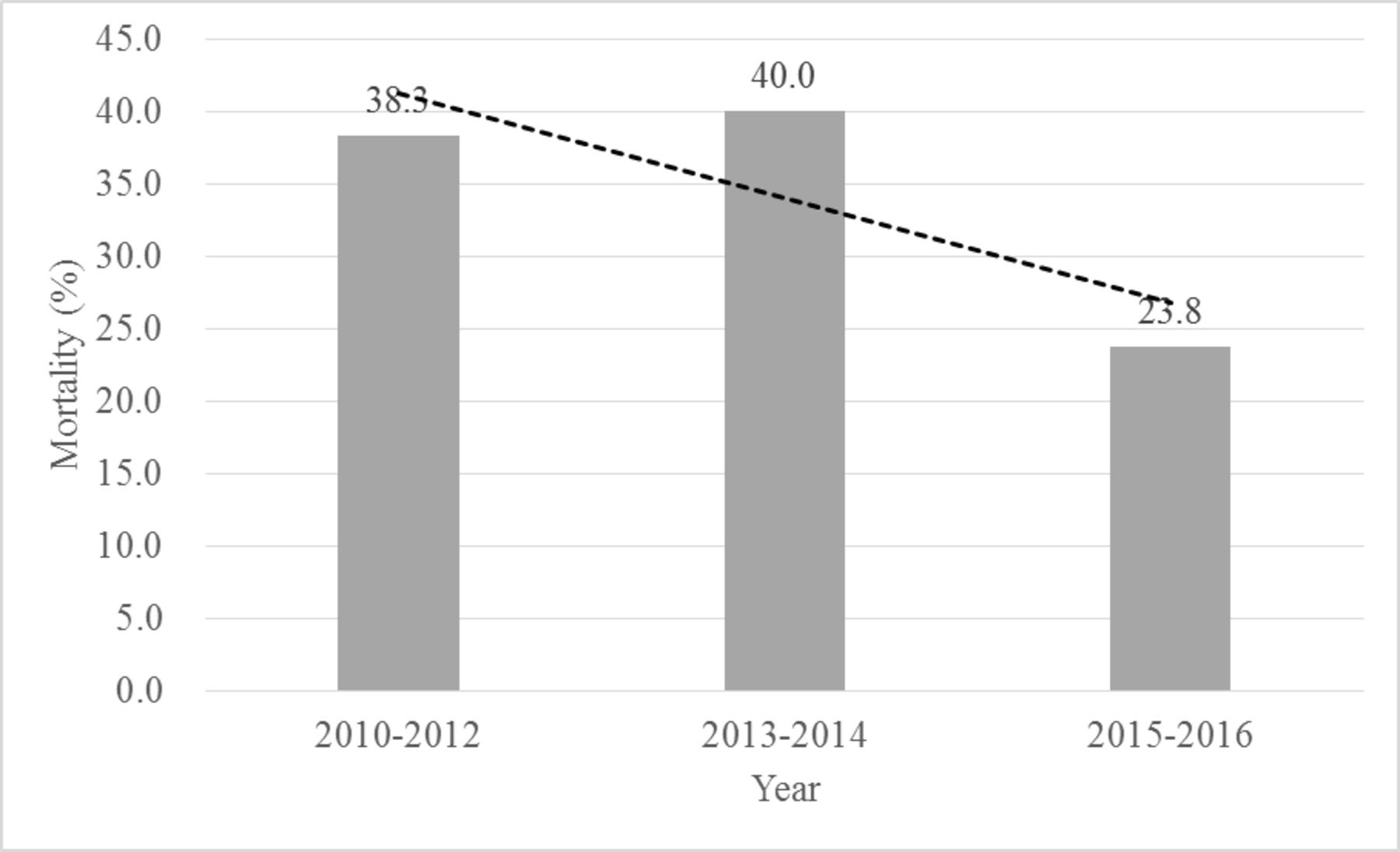
Outcome analysis in the ATDB cohort according to the establishment of the trauma center (pre-establishment, interim establishment and postestablishment), revealed decreased mortality rate post-trauma center establishment in 2015 and 2016 (figure 3). However, as the number of patients were too small (n=21), statistical significance could not be adequately assessed. ICU LOS (median, 3.5 days) and mortality (23.8%) were more similar between the post-trauma center establishment and NTDB cohorts (ICU LOS: median, 5 days; mortality, 23.1%) than between the pre-establishment and interim establishment of the trauma center and NTDB cohorts (table 4).
{kind=link}
{kind=link}
{kind=link}
Mortality rate change after severe pelvic fractures in a representative at Ajou trauma center according to the periods related to trauma center development and establishment.
Comparison of variables and outcomes between the pretrauma, interim trauma and post-trauma center establishment periods in the ATDB
Discussion
This study shows that there is difference in in-hospital mortality after severe pelvic fractures (AIS 4 or 5) at a single representative trauma center established in South Korea in 2015 when compared with matched patients treated at level 1 or 2 trauma centers in the USA. The difference, however, was not statistically significant when using the Kaplan-Meier survival curves and Cox regression analysis. Moreover, mortality and ICU LOS were similar in the post-trauma center establishment period in South Korea and in the NTDB dataset. It was also confirmed that older age, lower SBP and GCS at admission were associated with mortality in severe pelvic fractures. Although one must be careful in generalizing these findings, we were able to effectively compare two cohorts from two different population datasets, in two different countries and report significant risk factors associated with specific outcome measures in a specific anatomical injury using current statistical methodologies.
In this study, we compared two different cohorts using PSM. We were able to match 160 patients with severe pelvic fractures during 7 years from a representative trauma center in South Korea. For comparison purposes, we analyzed data from 6438 patients with severe pelvic fractures from the NTDB, which was established several decades earlier than the ATDB.22 23 However, even selecting only severe pelvic fracture cases (AIS of 4 and 5), there are still significant differences between the ATDB and NTDB cohorts in terms of pelvic and overall injury severity, associated injuries and mechanism of injury. Therefore, we employed PSM to control for those differences to be able to compare the two cohorts. We think that this study design is useful if appropriate statistical methods and adequate matching are used for the analysis in the field of traumatology, where prospective studies such as a randomized controlled trials are difficult to do.
Before PSM, a significantly higher in-hospital mortality rate was observed in the ATDB cohort compared with the NTDB cohort. However, patients in the ATDB cohort had more severe pelvic fractures than observed in the NTDB group. As the ATDB cohort included patients with higher pelvic AIS, lower SBP and GCS at admission and higher overall ISS when compared with the NTDB cohort, we used PSM to adjust for those confounding factors. Our data showed that difference in in-hospital mortality between the groups was reduced after matching. Comparing mortality rates between two cohorts derived from two different countries likely has its limitations.24 As we detected significant differences in hospital LOS between the two groups, such differences were taken into account when assessing differences in survival rates by the Kaplan-Meier and Cox regression methods. When we performed a Kaplan-Meier analysis for 30-day survival rates, no significant differences were observed between the two groups. The Cox regression analysis showed that the management of severe pelvic fractures at a representative trauma center in South Korea had a lower aHR for mortality than other factors such as age, SBP and GCS at admission. It should be noted, however, that the aHR for the treatment institution had borderline statistical significance (p=0.054). In summary, the simple comparison of in-hospital mortality rate by χ2 test in patients with severe pelvic injuries showed that the ATDB group had a higher mortality rate than the NTDB group, although this was not statistically significant in the Kaplan-Meier survival curve analysis or the Cox regression analysis model considering variables such as hospital LOS and ICU LOS. Additional analyses using the ATDB dataset relative to the period after the establishment of the trauma center (after 2015) revealed that the mortality rate, ICU LOS and days on the ventilator were more similar to those of the NTDB cohort although the number of cases was too small to determine any statistical difference.
Age, SBP and GCS at admission were significantly associated with mortality rate after severe pelvic fractures in comparisons between matched survivors and non-survivors in the Cox regression analysis. These results are in agreement with previous studies.4 25 These findings imply that patients with severe pelvic fractures who are older, presenting with hypotension and decreased level of consciousness are at higher risk of death and require more immediate interventions.
There are several limitations to this study. First, we used a retrospective study design and only included data from a single center in South Korea, therefore our findings cannot be generalized due to possible selection bias. Second, we relied on PSM to compare the two cohorts, and this methodology has some limitations.21 26–28 Lastly, the use of a registry-base dataset might may have introduced bias.29 In particular, there could be differences between datasets originating from two different countries.24 The ATDB applied the criteria used by the NTDB for registering the majority of the data. However, the NTDB dataset did not include information on transfusion volumes and types blood products, laboratory findings and specific data on efforts such as the type of surgical intervention or the use of interventional radiology techniques for bleeding control. Therefore, we could not conduct more in-depth analyses of outcome measures as they relate to treatment options.
In conclusion, patients with severe pelvic fractures (pelvic AIS 4 or 5) had a high mortality rate (>20%); mortality was significantly associated with older age, lower SBP and GCS scores at admission. Our results suggest that the establishment of a trauma center at AUMC has improved outcomes of patients with severe pelvic fractures.
References
Footnotes
Contributors KJ, SM, AS, KH and RC contributed to study design, data collection, data analysis and data interpretation. KJ, KH and RC were responsible for article writing. KJ, SM, JC-JL and RC were responsible for the critical revision of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; internally peer reviewed.