Article Text

Statistics from Altmetric.com
History
While a 20-year-old woman was being chased by an assailant, she tripped on railroad tracks, fell, and felt immediate pain in her left knee. As the pain led to loud screaming, the assailant fled. The emergency medical service brought the patient to a level 1 trauma center.
Examination
The patient was awake and alert with normal vital signs. She was unable to move her left knee, which appeared to be dislocated. Although she had sensation in the left foot and limited movement of the left ankle and toes, there were no palpable distal pulses or Doppler signals.
Question
The most appropriate first step in the management of this patient is:
Left below-knee four-compartment fasciotomy.
CT arteriography.
Administration of unfractionated heparin.
Operative exploration.
Management
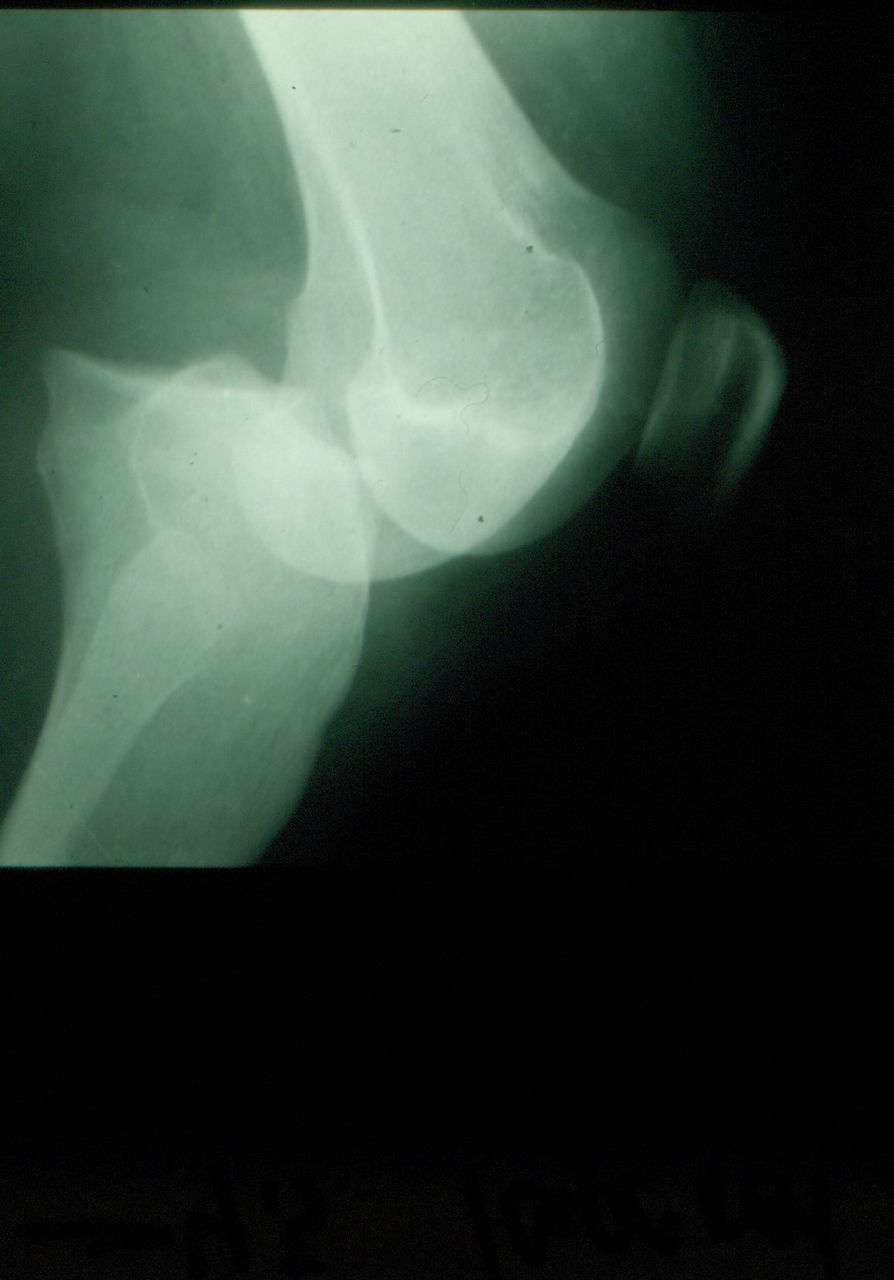
In consultation with the trauma attending surgeon, the trauma fellow administered intravenously 5000 units of unfractionated heparin in light of the probable complete occlusion of the popliteal artery and the lack of an open wound or other major associated injuries. Orthopedic surgery agreed that the patient had a posterior dislocation of the left knee with probable injury to the mid-left popliteal artery (figure 1). The dislocation was successfully reduced under intravenous sedation. No pulsations were noted in the left pedal arteries after the reduction.
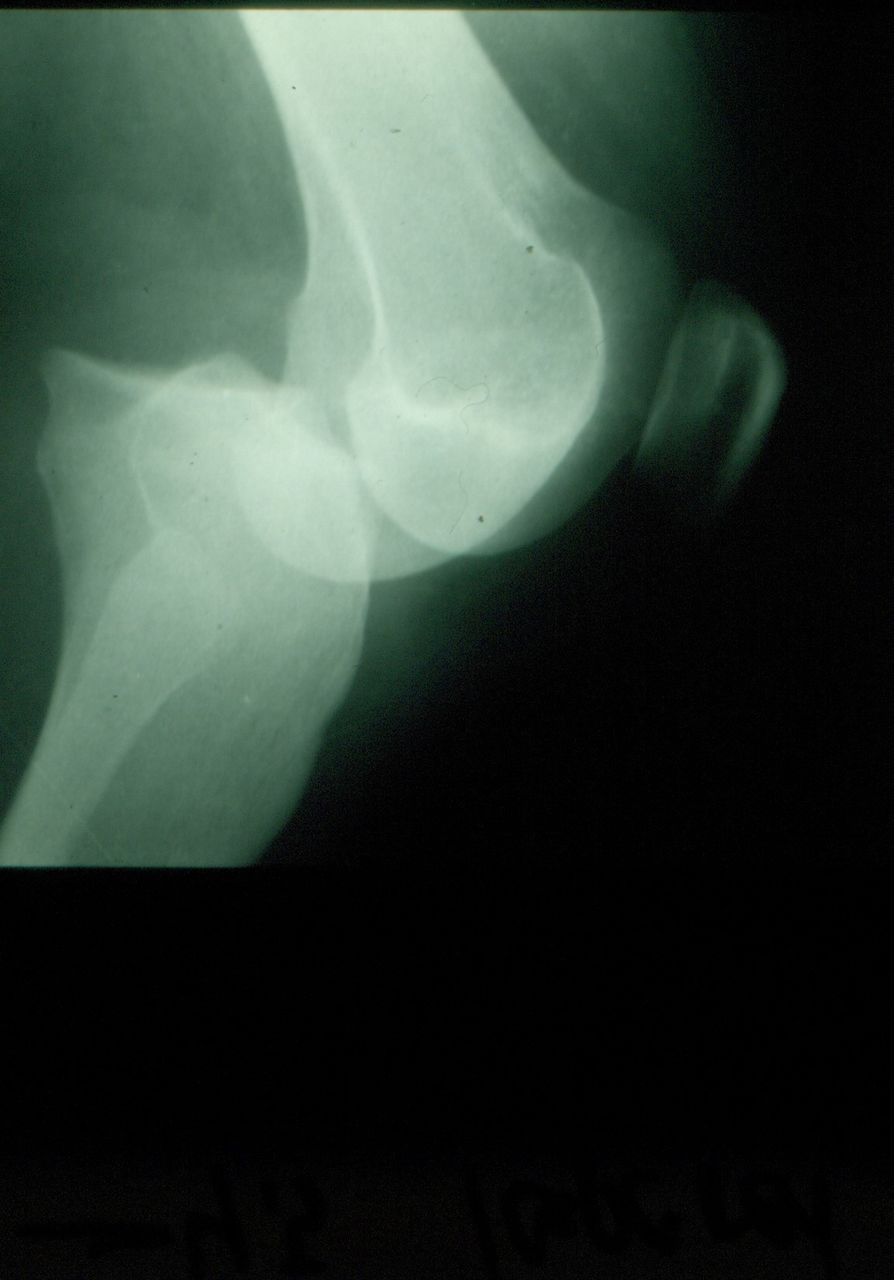
Posterior dislocation of the left knee joint.
Question
The most appropriate next step in the management of this patient is:
Left below-knee four-compartment fasciotomy.
CT arteriography.
Administration of aspirin (ASA) 181 mg.
Contact the endovascular surgeon.
Management
A one-shot left femoral arteriogram (patient cared for before availability of CT arteriography) documented a thrombosis in the left mid-popliteal artery (figure 2).
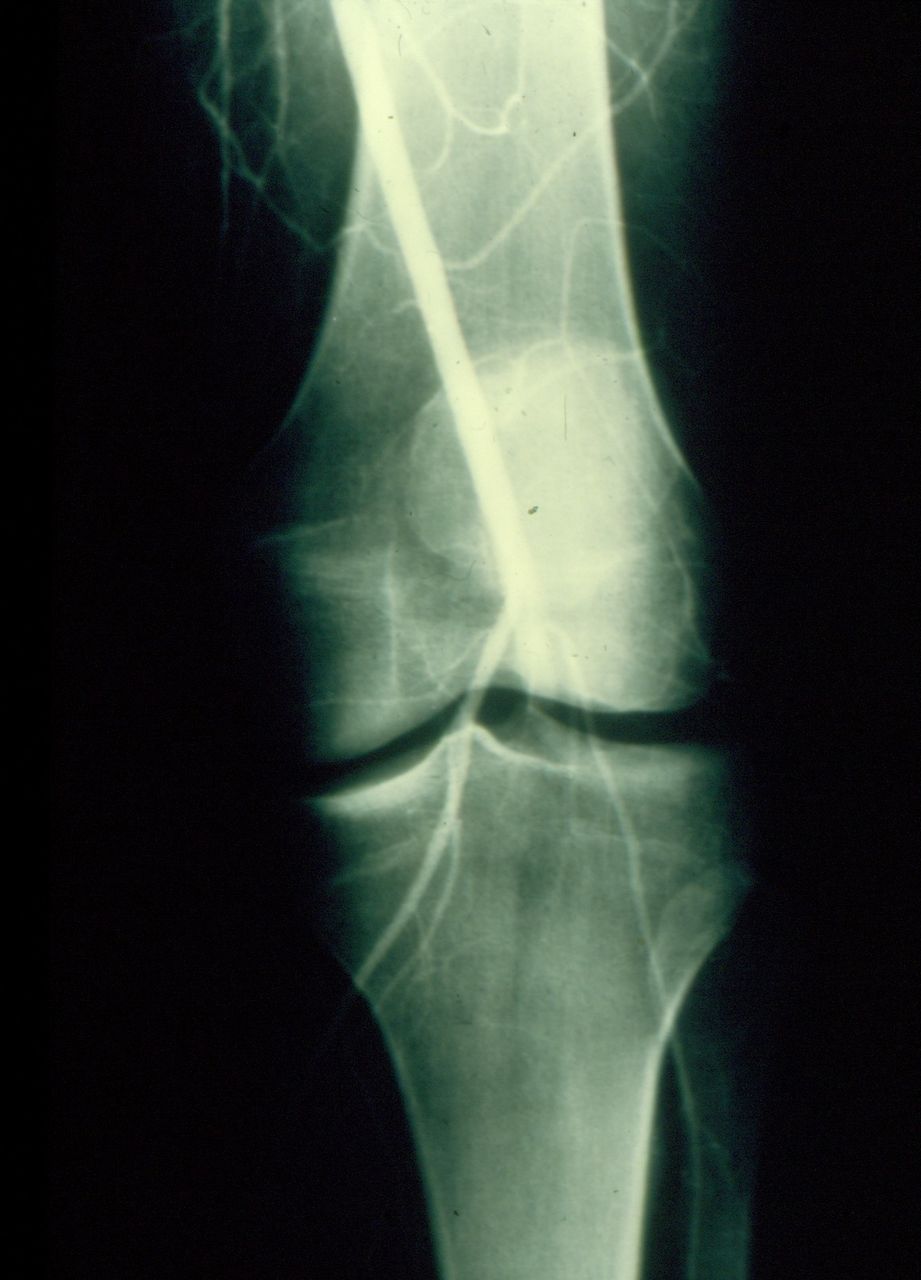
Blunt thrombosis of the left popliteal artery behind the knee joint.
The patient was typed and crossed for two units of packed red blood cells, received 1 g of cephalosporin antibiotic intravenously, and was moved to the operating room. With the patient in supine position, the left lower extremity was externally rotated, with the knee flexed to 30°. The skin was prepared and draped from the umbilicus to the bilateral toenails, and the left foot was placed in a sterile transparent plastic bag. A 15 cm longitudinal medial popliteal incision was made, starting along the anterior border of the sartorius muscle in the medial distal left thigh, extending posteriorly to the posterior knee joint, and completed approximately 1 cm behind the posterior border of the proximal tibia. Care was taken to avoid the greater saphenous vein in the distal one-third of the incision. The proximal popliteal vessels were exposed by retracting the sartorius and gracilis muscles posteriorly and the vastus medialis anteriorly. As noted in Wind and Valentine,1 the surgeon had to divide the attachment between the adductor magnus tendon from the semimembranosus muscle to visualize the popliteal vessels exiting the adductor hiatus. There was obvious thrombosis of the mid-popliteal artery (figure 3), and the proximal artery and adjacent popliteal vein were encircled with vessel loops. It became obvious that the extent of thrombosis mandated further exposure of the artery behind the knee joint. The tendons of the pes anserinus (sartorius, gracilis, and semitendinosus muscles) were then divided 1.5 cm from their distal bony attachments. Before each tendon was divided, the proximal and distal ends were marked with a colored suture, using different colors for each tendon. After the non-injured distal popliteal artery and adjacent popliteal vein were encircled with vessel loops, the extent of arterial thrombosis was 6 cm in length. A longitudinal arteriotomy 4 cm in length was made in the medial aspect of the area of thrombosis. Fogarty balloon catheters #4 and #5 were passed proximally via partial loosening of the vessel loop, and no clot was removed from the superficial femoral artery. After removal of the #5 Fogarty balloon catheter, 20 mL of a solution of 50 units of unfractionated heparin/mL of saline was injected proximally, and the proximal popliteal artery was reclamped. In a similar fashion, #3 and then #4 Fogarty balloon catheters were passed into the distal popliteal artery and beyond. Recognizing that the distal passage of the catheter goes into the peroneal artery nearly 90% of the time, the calf was gently massaged after the catheter was removed to encourage evacuation of any thrombus in the anterior and posterior tibial arteries. Once again, 20 mL of heparinized saline was injected distally and the distal vascular clamp was reapplied. An intimal disruption 2 cm in length was visualized and recognized as the source of the thrombosis (figure 4). A 4 cm segment of the artery containing the intimal disruption was resected. An end-to-end arterial anastomosis could not be performed because of excessive tension and a desire to save the geniculate collaterals around the knee. Using a reversed autogenous saphenous vein graft excised from the right proximal thigh, the proximal artery-to-graft anastomosis was completed using two continuous 6–0 polypropylene sutures to prevent a purse-string effect on the suture line. The last few polypropylene stitches on the distal anastomosis were left loose, and the proximal vascular clamp was removed for flushing. This clamp was reapplied, and the distal vascular clamp was removed for flushing and to evacuate all air from under the suture line. The two continuous polypropylene sutures were pulled tight, one knot was tied down to seal the anastomosis, and the proximal vascular clamp was removed. There were no major suture line leaks, and five more knots were placed.

Discoloration of area of thrombosis of the left popliteal artery.
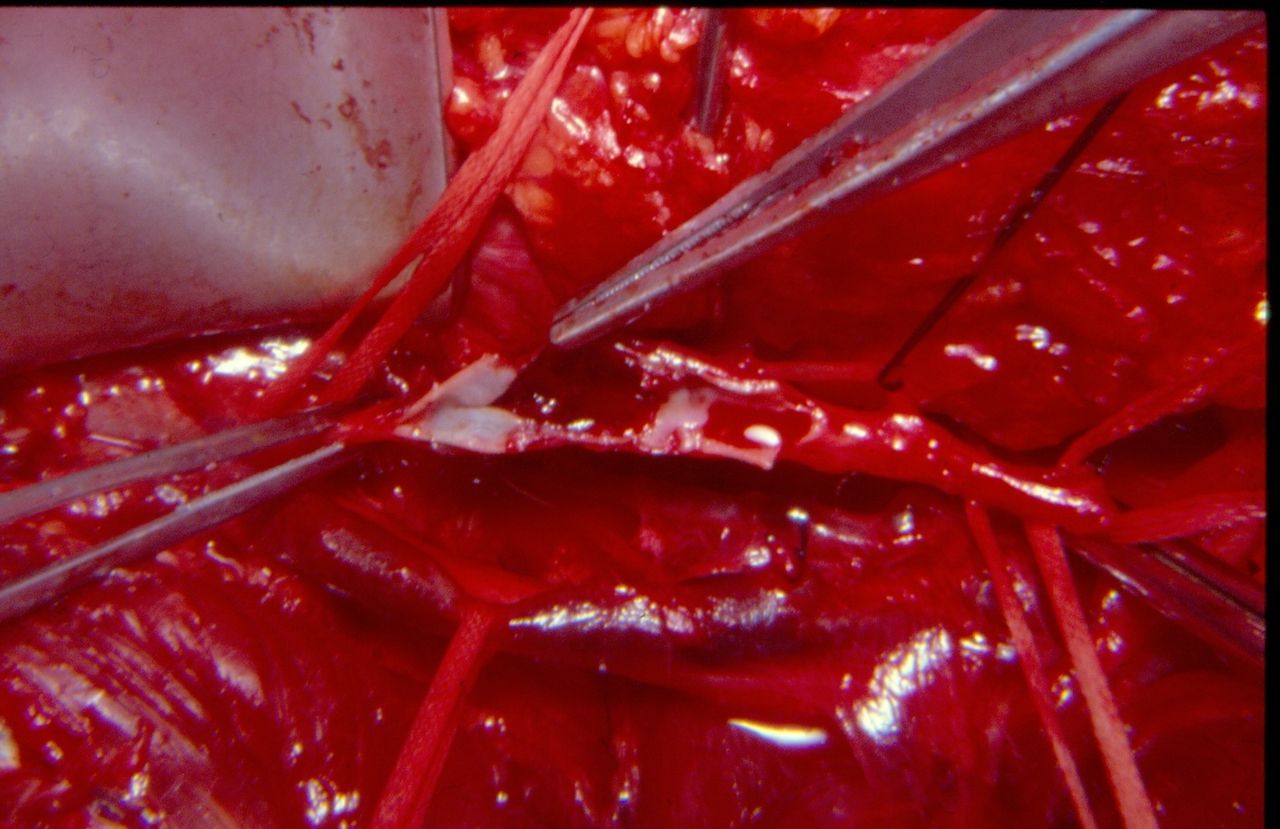
Opened left popliteal artery demonstrates intimal tear as source of thrombosis.
Even though arterial pulsations were readily palpable just distal to the interposition graft, pedal pulsations were not as robust. A 20-gauge plastic over metal arterial cannula was then inserted into the very proximal popliteal artery approximately 3 cm above the proximal anastomosis. A completion arteriogram (figure 5) documented multiple vascular clamp marks (large hollow arrows), patent anastomoses, and flow into the anterior tibial artery and tibioperoneal trunk (small hollow arrows). At this point pedal pulses were readily palpable. The tendons of the sartorius, gracilis, and semitendinosus muscles were reapproximated with permanent horizontal mattress sutures, and the medial popliteal incision was closed in layers. A left knee immobilizer was then placed on the patient.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Post-repair arteriogram documents multiple vascular clamp marks (large hollow arrows), patent anastomoses (black arrows), and flow into the anterior tibial artery and tibioperoneal trunk (small hollow arrows).
The patient was placed on oral aspirin 81 mg orally every 12 hours in the evening after the operation. At the time of discharge 3 days later, the patient was instructed to start a gentle daily walking program with the knee immobilizer in place for 1 month. In addition, she was referred for physical therapy on the left knee joint to start in 1 month, and advised to cease smoking and continue the oral baby aspirin dosage as described above for 3 months.
Discussion
Historically, blunt thrombosis of the popliteal artery resulted in an amputation rate of over 30% in some series.2 This was often due to (1) extensive associated injuries to soft tissue, bone, popliteal vein, and tibial nerve from high kinetic energy motor vehicle–pedestrian or motorcycle crashes; (2) delays in recognition and treatment; and (3) delays in the recognition and treatment of compartment syndromes below the knee.3 There is, however, a subset of patients with blunt injuries to the popliteal artery resulting from an isolated posterior dislocation of the knee joint. Older articles have noted an incidence of injury to the popliteal artery in approximately 15% of these patients, although many of these were injuries to the intima and media (abnormal imaging) rather than complete thrombosis.4 For a period of time in the 1980s and early 1990s, this high incidence of injuries prompted mandatory arteriograms of the popliteal artery in all patients with a history of a posterior dislocation of the knee. This philosophy gradually changed based on studies at the Los Angeles County Hospital–University of Southern California Medical Center and at the University of Florida Health Science Center, Jacksonville .4–6 In a 2002 report by Miranda et al from Jacksonville, the authors concluded that significant injuries (require operative repair) could be reliably (94.3% positive predictive value) predicted on a physical examination without arteriography.5 In combination with an Ankle-Brachial Index <0.9 in the injured lower extremity, it would be unlikely that a thrombosis or major blunt injury to the popliteal artery would have delayed recognition in the modern era.
The important points emphasized in this case report include the following:
Posterior dislocation of the knee joint results in the need for operation on the popliteal artery in less than 10% of patients.
Preoperative anticoagulation is appropriate in the patient with thrombosis of the popliteal artery and the absence of any contraindications (ie, significant associated injuries to the extremity, or associated injury to the brain, solid organ or pelvis).
A dislocation of the knee will usually result in injury to the popliteal artery directly posterior to the knee joint, but a CT arteriogram is mandatory to recognize an abnormal location or distal in situ thrombosis or embolization.
The medial approach to the popliteal artery is a comfortable one for most general trauma surgeons, but the posterior approach is favored by some surgeons.
Exposure through the medial approach may require temporary division of the three tendons of the pes anserinus.
Fine principles of vascular repair are mandatory on this “end” artery. These include use of small vascular clamps or bulldog clamps, passage of Fogarty balloon catheters, continued intraoperative heparinization, appropriate flushing sequence before re-establishing arterial flow, and a completion intraoperative arteriogram.
Although the use of postoperative ASA after insertion of an interposition graft would not be considered routine by many experienced vascular surgeons, its success in maintaining patency of coronary bypass grafts would suggest that it would be useful for grafts in small arteries of the extremities.
Footnotes
Contributors DVF completed the article and submitted it for publication as requested.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.