Article Text

Abstract
Background Mechanically ventilated patients in the intensive care unit (ICU) are unable to communicate verbally. We sought to evaluate their needs via a communication board (CB) and a novel eye tracking device (ETD) that verbalizes selections made by gazing.
Methods This was a pilot prospective study conducted in a tertiary care surgical ICU. Continuously mechanically ventilated adult surgical ICU patients with a Richmond Agitation-Sedation Scale score of −1 to +1, without cognitive impairment, were eligible. We asked patients four yes-or-no questions to assess basic needs regarding presence of pain, need for endotracheal suction, satisfactory room temperature, and position comfort. Patients were then asked if there was anything else that they wanted to communicate. All responses were confirmed by head nodding.
Results The median accuracy of the CB (100% (IQR 100%–100%)) for basic needs communication (yes/no questions) was comparable with that of the ETD (100% (IQR 68.8%–100%); p=0.14) in the 12 enrolled patients. Notably, 83% of patients desired to communicate additional information, ranging from spiritual (eg, desire for prayer/chaplain), emotional (eg, frustration, desire for comfort), physical/environmental (eg, television), to physiological (eg, thirst/hunger) needs.
Discussion The majority of patients desired to communicate something other than basic needs. Unless specifically assessed via an assistive communication device (eg, CB or ETD), some of these other needs would have been difficult to discern.
Level of evidence IV therapeutic care/management.
- mechanical ventilation
- critical care
- eye tracking device
- communication
- assistive and alternative communication (AAC)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- mechanical ventilation
- critical care
- eye tracking device
- communication
- assistive and alternative communication (AAC)
Introduction
Over half of mechanically ventilated patients attempt to communicate, but many of these attempts are unsuccessful.1–3 Impaired communication during mechanical ventilation is frustrating for both patients and staff.4–6 Moreover, it has been linked to an increase in preventable adverse events.7
Few options exist to facilitate communication for continuously mechanically ventilated patients. Often, communication is limited to mouthing words, hand gesturing, and head nodding, which can be time-consuming and ineffective.8–10 Also, patient communication is typically limited to answering specific questions posed to them.
Current primary methods for assistive communication include communication boards (CB) and speech-generating touch screen devices; yet many patients lack the fine motor control necessary to navigate these devices independently.11 Further, a previous investigation found that only 27% of alert and oriented mechanically ventilated intensive care unit (ICU) patients could write legibly.12 The electrolarynx has recently been employed in case studies and series with some success, but its utility remains unclear.13 14 Speaking tracheostomy tubes and one-way speaking valves have also been employed for patients with tracheostomies, but typically require ventilator breaks for cuff deflation, and thus cannot be routinely employed.15
It has been postulated that an assistive technological aid such as an eye-tracking device (ETD) may be able to address this unmet need in mechanically ventilated patients without oral motor or fine motor abilities.11 ETDs detect eye movement and position, and then integrate data to create a gaze point for selection on a screen; this selection is then verbalized to the patient and caregiver by the ETD computer.16 ETDs have tremendous potential (customizable pages, writing by gaze detection, and surfing the world wide web by gaze detection alone) to facilitate freedom of communication beyond our pre-selected pages. ETDs are well established as a beneficial communication method for patients with neuromuscular disorders, in particular Amyotrophic Lateral Sclerosis (ALS).17 18 However, the use of ETDs as communication devices in the ICU has not been extensively examined. In this pilot study, we investigated the use of assistive communication devices by mechanically ventilated patients in a surgical ICU. We evaluated basic needs that would commonly be addressed in routine ICU care and alsosought to determine if there were any other issues or concerns that patients needed to relay to health care providers.
Setting and patients
This pilot prospective study was conducted in the 14-bed trauma/surgical ICU of an academic tertiary care medical center. The medical center is also an American College of Surgeons-verified level I trauma center. We evaluated admitted trauma/surgical ICU patients for enrollment during a consecutive 30-week period (July 2016–February 2017), from Monday through Friday. We evaluated the communication needs and abilities of a highly select patient population: patients receiving continuous mechanical ventilation via an endotracheal tube or tracheostomy at the time of screening, English-speaking, without cognitive impairment, and without traumatic brain injury that resulted in impaired motor or eye scores on the Glasgow Coma Scale. To ensure the absence of cognitive impairment, patients were assessed for their ability to follow commands by looking in three directions and responding yes or no to their correct name and an incorrect name. Patients had to be alert and calm (ie, Richmond Agitation-Sedation Scale score −1, 0, or +1). To avoid any interference in patient care, sedation, if any, could not be turned off for the study. The study was originally designed to be conducted on two consecutive days, with either the communication board (CB) or ETD used initially on the first day and the other device used first on the second day. However, given difficulty in recruiting patients to participate on two consecutive days, a modification was made whereby patients were evaluated on a single day. At the end of the continuous enrollment period, additional patients were recruited from a convenience sample during a non-continuous 3-month period, ending in January 2018.
Materials
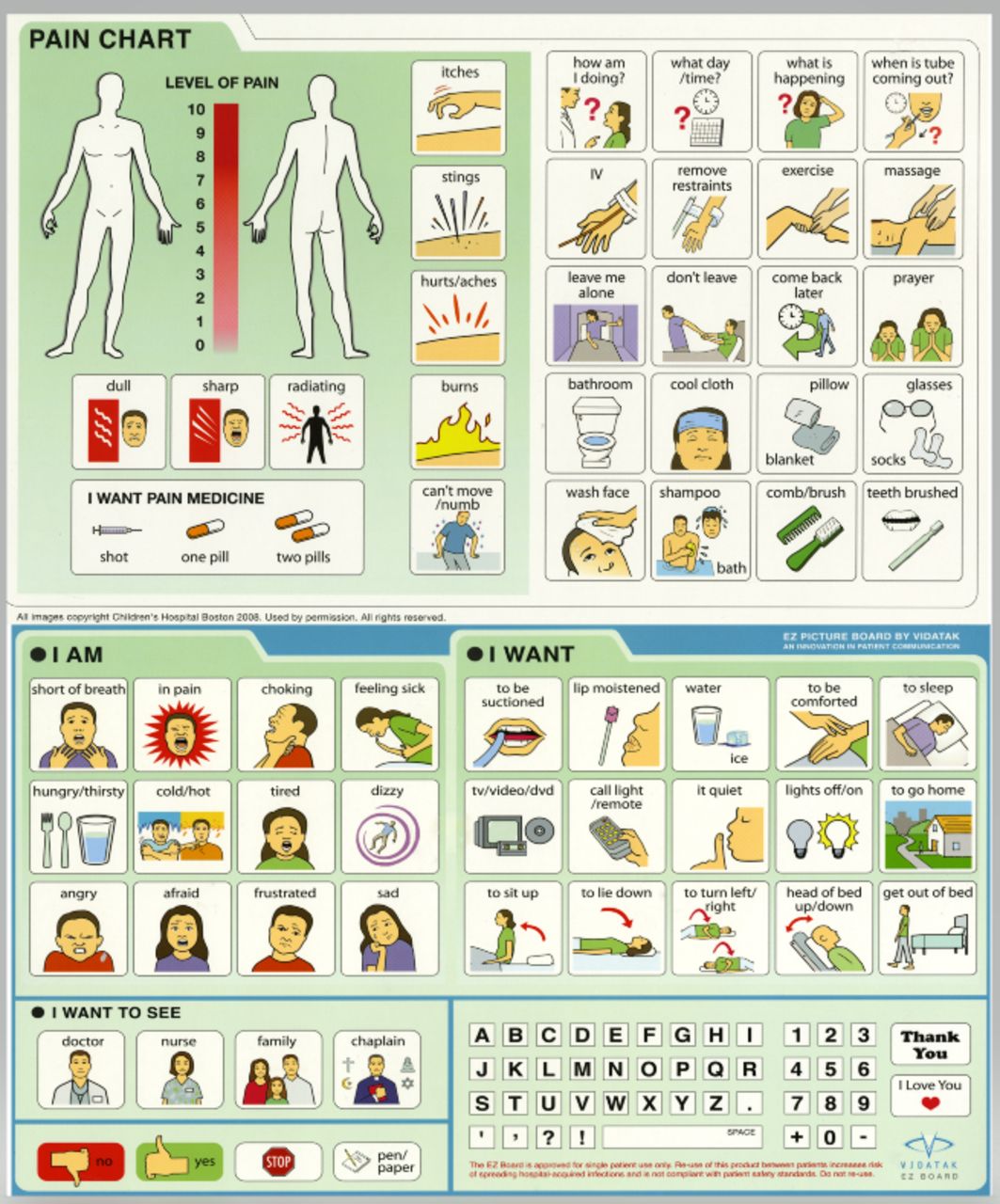
The Tobii Dynavox I-15 eye tracking device (Tobii Dynavox, Danderyd, Sweden; figure 1) and Vidatak EZ communication board (Acuity Medical, Annapolis, MD; figure 2) were employed for this study. The ETD is composed of a camera, a projector, and a preprogrammed algorithm, all of which are integrated into a free-standing monitor.16 The device was calibrated with each patient at each new usage session. Calibration was achieved by having the patient follow a cursor with their eyes to five points on the screen. Several page-sets available from the manufacturer were adapted by the study team to reflect the picture-word sets on the CB. Four main pages were created. The patient could select any item on the screen by maintaining their gaze on the selection for 400 milliseconds. Selections made by gazing were then verbalized by the ETD computer. Although the ETD we used also has a touch screen; this feature was not used during the study. Meanwhile, Vidatak EZ communication boards are composed of dual-sided laminated cardboard and feature pictures, words, and letters.

Tobii Dynavox I-15 eye tracking device.
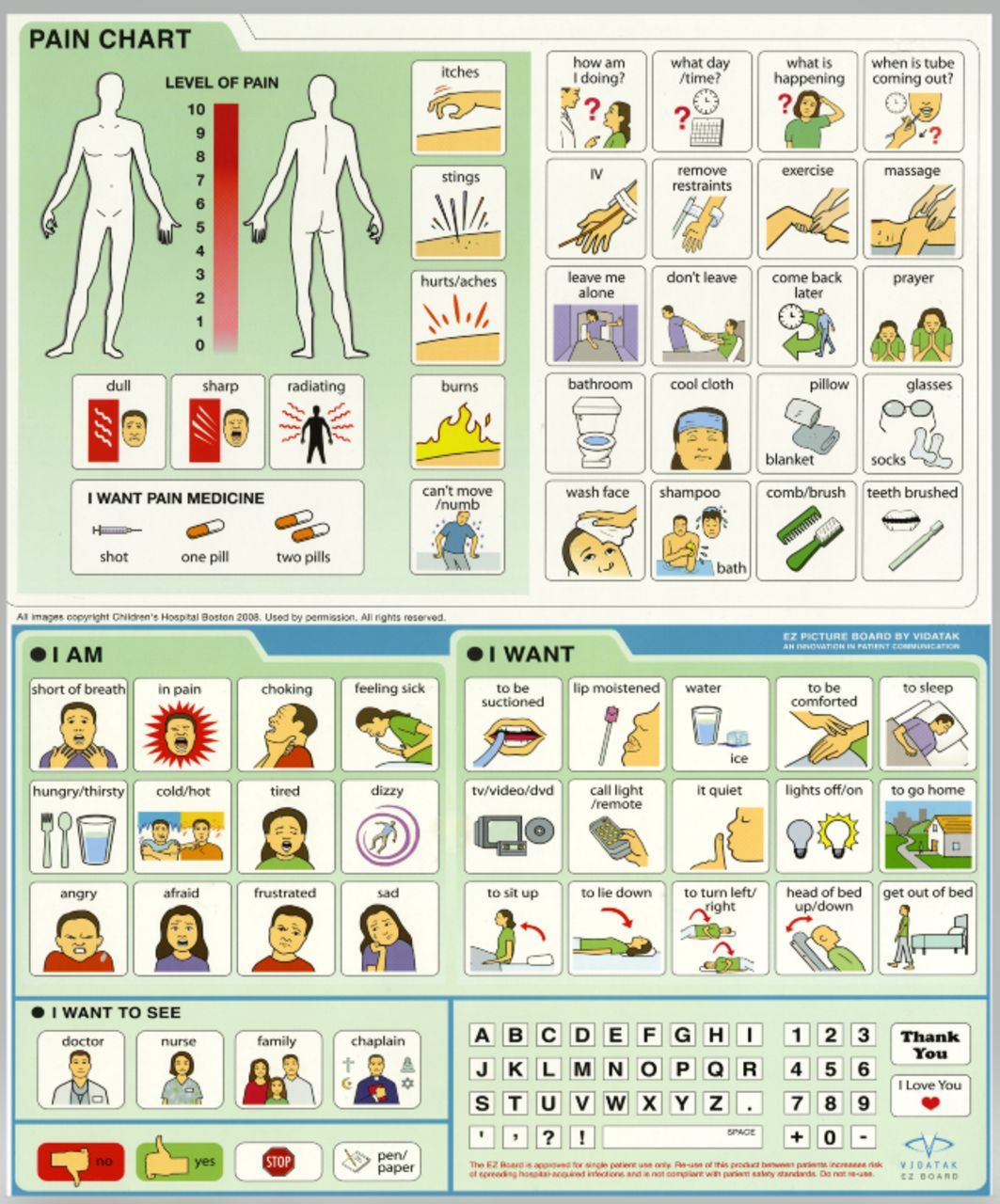
Vidatak EZ picture board.
Design
Once consented for the study, patients were introduced to the CB and ETD with a brief 1-minute introduction detailing how to access the ETD screens and the items on the CB. Orientation duration was brief by design to create a comparable user experience between the CB and ETD; the CB required minimal orientation due to its design, and thus orientation to the ETD was also kept brief.
Patients were verbally asked four basic needs yes-or-no questions: (1) ‘Are you in pain?’ (2) ‘Is your position comfortable?’ (3) ‘Do you feel that the room temperature is okay?’ and (4) ‘Do you need suctioning?’ Accuracy of the response was confirmed by the examiner repeating the patient’s response and asking ‘is this correct?’ The patient would then nod their head in response. For example, if a patient pointed to ‘yes’ on the CB when asked if they were in pain, the staff would state, ‘You indicated that you are in pain, is this correct?’ The patient would nod their head yes or no and the accuracy of their response was recorded. The patients were then asked if they had anything else that they would like to communicate and were given the opportunity to respond. Patients that were in odd-numbered rooms were evaluated with the ETD first, followed by the CB, whereas patients in even-numbered rooms were assessed with the CB followed by the ETD.
Study procedures were completed by first-year and second-year medical students. An occupational therapist or nurse was needed to observe each patient encounter as a requirement for enrollment during the 30-week period of continuous recruitment. Patients with limited ability to point to objects on the CB were assisted by staff pointing. Patient and observer preference between assistive (CB and ETD) and baseline forms of communication (head nodding or writing) was assessed. The patient’s/observer’s limited exposure and familiarity with the ETD precluded a meaningful assessment of patient and provider preference between the CB and ETD.
Data analysis
Basic descriptive (median, IQR) and inferential (Wilcoxon rank-sum) statistics were performed using SPSS V.23.0 to compare device accuracy. Because of the small sample size, further statistics were not performed.
Results
During the 30-week period of continuous recruitment, a total of 389 adult surgical ICU patients were screened, of whom 142 were receiving continuous mechanical ventilation at the time of screening (36.5%). Of this total population, 26 patients (18.3% of mechanically ventilated patients) met the inclusion criteria for this pilot study. Ten patients declined to participate. Three patients were excluded due to observer unavailability during this continuous enrollment period. Two patients were excluded because the ETD failed to detect their gaze due to ptosis or nasogastric tube interference. One additional patient’s session was interrupted by urgent transportation to surgery. Five additional patients were identified as meeting the inclusion criteria during the 3-month period of non-continuous enrollment, but three patients declined participation. An additional two patients were enrolled during this period (figure 3).

{kind=link}
{kind=link}
{kind=link}
Study enrollment. GCS, Glasgow Coma Scale; ICU, intensive care unit; RASS, Richmond Agitation-Sedation Scale; TBI, traumatic brain injury.
The demographics and clinical characteristics of the 12 patients who completed the study are listed in table 1. All patients communicated with head nodding; none had cervical spine injury. Prior to enrollment, four patients had access to a CB and five patients were able to write, although head nodding was still used as their primary form of communication. Eight patients made CB selections by pointing themselves. Four patients required image-by-image pointing by the research team to indicate responses. ETD selections were based on gaze alone, without image-by-image pointing by researcher or patient.
Demographics of enrolled patients (n=12)
Patients were asked four basic needs questions (ie, yes/no questions) regarding pain, satisfactory positioning, satisfactory room temperature, and need for endotracheal suctioning. For these four basic needs questions, participants responded with a median accuracy rate of 100% (IQR 100%–100%) using the CB and 100% (IQR 68.8%–100%) using the ETD (p=0.14). Specifically, 12 participants answered 46 of 48 (96%) yes-or-no questions correctly using the CB, compared with 36 of 48 (75%) using the ETD. Eleven patients demonstrated 100% accuracy in intended selections with the CB, whereas seven patients demonstrated 100% accuracy with the ETD.
After asking the basic needs questions, we asked patients if there was anything else they would like to communicate in the format of a free-response question. Most (10 of 12) patients expressed at least one additional desire/need via the CB and/or ETD, and several of these patients had multiple requests. These needs were separated into four categories (table 2): spiritual, emotional, physical/environmental, and physiological. Ten patients made 29 free-response statements using the CB. Patients using the CB most frequently requested to go home (three patients) and to have their lips moistened (three patients). The next most frequent requests, each of which was requested by two patients, were for chaplain/prayer, family, nurse, or doctor. A variety of emotions including anger, frustration, a desire to be left alone, and a desire to be comforted (one patient each) were also expressed using the CB. Additional comments are presented in table 2. In contrast to the CB, the ETD was employed by eight patients to make nine requests during the free-response section. Only one patient made the same request with the CB and ETD. Repositioning was requested most frequently (three patients), followed by medication and thirst (two patients each). Of note, pain was assessed separately as part of the basic needs questions and is not included in table 2, unless the patient indicated this specifically as part of their free-response with the CB and/or ETD.
Patients’ needs and concerns at the first session (n=10)
Prior to protocol change, five patients were eligible for a second session, but three were excluded (one was too sedate, one declined the second session, and one was extubated). Hence, a second session was completed in only two patients. The requests made by these two patients are presented here; they are not included in table 2. Both patients requested prayer/chaplain, repositioning, and reported pain and its severity during both sessions. One patient also requested the presence of family, their doctor, and their nurse during the second session (this was requested in the first session as well).
Most patients (n=10) preferred the use of an assistive communication device (CB or ETD) to their baseline form of communication (n=2). Of the two patients who preferred their baseline form of communication, one was capable of writing whereas the other could only nod their head. Ten patients’ sessions were observed by a nurse or occupational therapist. According to the observers, head nodding was the easiest tool for basic communication in seven patients, followed by an assistive communication device in three patients. An assistive communication device was considered the best option for complex communication in eight patients, followed by writing in two patients.
Discussion
Approximately 36.5% of patients in our ICU were receiving mechanical ventilation at the time of recruitment during the period of continuous enrollment. This number falls well within the typical range of mechanical ventilation in ICUs reported by Project IMPACT.19 Of the mechanically ventilated patients, 18.3% (26 of 142) met the enrollment criteria. This percentage of ICU patients considered candidates for assistive communication is significantly less than half of all mechanically ventilated patients in contrast to estimates from prior studies.2 A principal reason for this low number of enrollees is the strict study inclusion criteria. Indeed, tracheostomy patients transitioning off mechanical ventilation (ie, not being continuously mechanically ventilated) were excluded. Further, as sedation could not be stopped for the study, patients who were sedated at the time of assessment were not reassessed until the following day. Sedation may have varied throughout the day, precluding potentially eligible patients from participating.
One of the goals of this study was to identify if the ETD could be used to assess basic needs in the ICU. As such, the study was designed to mimic typical clinical conditions. In general, a variable number of patients have access to CBs while hospitalized, whereas no patients have access to ETDs. Rather, assessment of basic needs by hospital personnel typically involves the use of the patient’s baseline form of communication or the introduction of a new communication aid.
We attempted to determine if the ETD would benefit continuously mechanically ventilated ICU patients. Only two small studies have examined the use of ETDs as a communication aid in the ICU.20 21 To this end, we first assessed the ETD’s accuracy by asking four basic needs questions. The four questions selected for basic needs assessment were ones that were routinely asked by the nurses when evaluating a patient. The accuracy of the CB was not significantly different from the ETD.
We subsequently assessed patient needs using a free-response question and found that 83% of patients had a desire to communicate something other than basic needs. Notably, many patients had spiritual, emotional, physical/environmental, and physiological needs. For simplicity, patient statements were divided into these four broad categories, although some statements may fit into more than one category. These findings are congruent with a previous small study of 16 intubated patients via fixed-response survey questionnaires that found that patients expressed frustration, pain, and a desire for pastoral care.22 To this end, we found that several patients wanted a visit from their nurse, physician, family, friends, or a chaplain. Many of these free-response requests would have been difficult to ascertain without the use of an assistive communication device, as head nodding would not have sufficed. Of note, 83% of patients preferred the CB or ETD over their baseline communication method (head nodding/writing), further suggesting that relying on head nodding alone may be insufficient to adequately address the needs of mechanically ventilated patients.
The presence of a family member, a person to help calm the patient, or 1:1 nursing ratio has been shown to reduce delirium and decrease ICU length of stay and duration of mechanical ventilation.23 24 As healthcare professionals focusing on patient pathophysiology, these requests demonstrate the need for a more holistic/patient-centered approach to care. The findings of pain or request for medication are generally anticipated, whereas the spiritual and emotional needs are difficult to determine unless specifically examined. The importance of assessing the spiritual and emotional needs of patients in the ICU cannot be overemphasized.25
Limitations
Because we wanted to evaluate the use of a novel communication device without any alteration in the patient’s care, a relatively small sample population was able to be recruited for this study. Patients were initially enrolled for two usage sessions conducted over 2 days, which was later modified to one usage session over 1 day. This modification was made in response to an unexpectedly small percentage of patients who were eligible for 2 days of participation. Most patients who qualified for the initial usage session were extubated prior to the second session. Additional reasons included limited patient and staff availability, and decreased patient/family interest in repeat testing. Although the study demonstrated ETD feasibility, the brief exposure time and the novel, unfamiliar technology employed by the ETD precluded determination of an optimal assistive communication device. Permitting greater device access would have increased patient/observer device familiarity and arguably interest in a future longer duration study.
Conclusions
The overwhelming majority of mechanically ventilated ICU patients wanted to communicate something other than basic physical and physiological needs. It would have been difficult to discern these concerns, especially the spiritual and emotional needs of our patients without an assistive communication device. This pilot study highlights the utility of ETD and CB in mechanically ventilated patients, but its small sample size precludes determination of an optimal method. Rather, the method used to communicate with patients should be varied by patient condition and ICU resources. For many patients, a CB may be appropriate. For other patients, especially those unable to point because of a cervical spine injury or those interested in engaging with novel technology, an ETD may offer additional communication possibilities.
Acknowledgments
The authors would like to acknowledge Emily Huang for data analysis, Tobii Dynavox for loaning the device and developing the requested pages, and Tobii Dynavox and Vidatak for permitting publication of photos of their devices.
References
Footnotes
Presented at This article was presented in part at the 12th Annual Academic Surgical Congress in Las Vegas, Nevada, in February 2017.
Contributors Study design: JG, EID, DF, KG, CM, MD, RJ, JV, JR. Study implementation (patient recruitment and testing): EID, JG, DP, LT, AF, KG, CM, MD, DF. Data analysis: JG, EID, RJ, DF, JV. Article preparation: JG, EID, RJ. Critical revision: CM, KG, DF, JV, JR, RJ, EID, AF, LT.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Tobii Dynavox (Stockholm, Sweden) loaned the eye tracking device for this study. Tobii Dynavox and Vidatak (Acuity Medical, Annapolis, MD) approved the use of included photos. Tobii Dynavox recused itself from study design, data, analysis, and drafting of the article.
Competing interests None declared.
Patient consent Not required.
Ethics approval The Stony Brook University Human Subjects Committee (IRB) approved this pilot prospective study.
Provenance and peer review Not commissioned; externally peer reviewed.