Article Text

Abstract
Background An important critique with respect to the utilization of intermediate care units (IMCU) is that they potentially admit patients who would otherwise be cared for on the regular ward. This would lead to an undesired waste of critical care resources. This article aims to (1) describe the caseload at the IMCU and (2) to assess the triage system at the IMCU to determine potentially unnecessary admissions.
Methods This cohort study included all admissions at the mixed-surgical IMCU from 2001 to 2015. The Therapeutic Intervention Scoring System-28 (TISS-28) was prospectively collected for all admissions to describe the caseload at the IMCU and to identify medical criteria for admission. These were combined with logistical criteria to assess the IMCU triage system.
Results A total of 8816 admissions were included in the study. The average TISS-28 was 20.19 (95% CI 18.05 to 22.33), corresponding with 3.57 (95% CI 3.19 to 3.94) hours of direct patient-related work per patient per nursing shift. Over time, this increased by an average of 0.27 points/year (p<0.001). Of all admissions, 6539 (74.2%) were medically considered to be justly admitted, and 7093 (80.4%) were logistically considered to be justly admitted. With these criteria combined, a total of 8324 (94.4%) were correctly admitted.
Discussion Most admissions to the IMCU are medically and/or logistically necessary, as the majority of admitted patients demand a higher level of nursing care than available on the general ward. Continuous triage is thereby essential. These findings support further utilization of the IMCU in our current healthcare system and has important implications for IMCU-related management decisions.
Level of evidence Level VI.
- intermediate care unit
- high dependency unit
- critical care delivery
- nursing workload
- triage system
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
An important criticism of the utilization of intermediate care units (IMCU) is that they potentially admit patients who would otherwise be cared for on the regular ward, thereby wasting critical care resources.1 Therefore, this potential inefficiency should be an important quality parameter when assessing or comparing IMCUs.2 This is of particular importance given the widespread and increasing use of IMCUs.3
At the intensive care unit (ICU) level, multiple studies have been performed to identify patients who do not need ICU care.4–7 To differentiate between patients who truly do and do not need ICU care, different parameters have been used: the predicted risk of in-hospital death based on physiologic variables, age, diagnosis, comorbid conditions and ICU admission score; the duration of stay combined with the received ICU-specific procedures; and the Therapeutic Intervention Scoring System (TISS-76).4 5 7 8
At the IMCU, the TISS is also being used, most often in its simplified form: the TISS-28.9 In previous studies, this has been used to determine the optimum staffing ratio and to compare differences in management format in a before-and-after design, in which the performance before and after a change in management format is assessed.10 11
In the current study, we use the TISS-28 to describe the caseload (nursing workload) at the mixed-surgical stand-alone IMCU. Subsequently, we assessed the triage system at the IMCU to provide insight into the extent of (un)necessary use of the IMCU.
Methods
Study design and setting
This observational cohort study was conducted at the surgical IMCU of the University Medical Centre in Utrecht, a tertiary university referral hospital in the Netherlands. This stand-alone, mixed-surgical IMCU admits patients from all surgical disciplines, providing hemodynamic monitoring and cardiovascular and respiratory support including inotropic use and supplementary oxygen. It has a nurse-to-patient ratio of 1:1.5. Triage for admission was performed by the responsible medical team of the IMCU in collaboration with the admitting specialist. All admissions to this IMCU between January 1, 2001 and December 31, 2015 were included in the study. According to the Institutional Review Board, the study was not subject to the Medical Research Involving Human Subjects Act, and therefore informed consent was waived (protocol number 17-326/C).
Nursing workload
To assess the nursing workload, the TISS-28 at admission was used. The evening IMCU nurse registered the TISS-28 daily for all patients. If no TISS-28 was registered for a patient on the day of admission, the next available TISS-28 was used. Every point scored corresponds to 10.6 minutes of nursing work per nursing shift.9 Also, to assess the maximum nursing workload at the IMCU, the maximum TISS of all admissions and of admissions with a duration of more than 24 hours was reported. Subsequently, the range of the 25% highest TISS at admission and its mean were reported. The hypothetical maximum TISS of 78 could not be reached, as mechanical ventilation and renal replacement therapy are not provided at the IMCU.
The development of the TISS-28 during the 15 study-years at the IMCU was also analyzed. Particular attention was directed towards the following three different management formats used within this period: the open format, with admitting specialists in charge (period I); the closed format, led by a team of anesthesiologists, surgeons and internal medicine physicians (period II); and the joint format, with the admitting specialist in charge under direct supervision of trauma surgeons with additional critical care certifications (period III). These management formats are described in more detail in a previous report. 12
Nursing activities performed
Nursing activities were described using the individual TISS-28 items, which reflect the nursing skills needed at the IMCU.
Assessment of triage system: medical criteria
Subsequently, the TISS-28 was combined with specific reasons for admission to determine whether an admission at the IMCU was medically essential. Medically essential admissions were defined as patients admitted to the IMCU who could likely not have been safely admitted to the general hospital ward.
Three criteria for medically essential admissions were (1) a TISS-28 of ≥18, (2) specific nursing tasks unable to be performed in the general ward, and (3) a specific reason necessitating admission to the IMCU. A TISS of ≥18 corresponds with more than 3 hours of direct patient-related nursing care per nursing shift. With a nurse-to-patient ratio of 1:5 during day shifts in our general hospital ward, this was considered the maximum safe and desired workload of a patient in the ward. An example of a specific nursing activity that could not have been performed in the general ward is administration of vasopressors. With respect to the third criterion, specific reasons for admission to the IMCU included cardiac monitoring or respiratory insufficiency, among others. Cardiac monitoring was required when patients were at risk for cardiac abnormalities, for example, patients with suspected cardiac contusion or hyperkalemia. Respiratory insufficiency was indicated if standard oxygen therapy at the hospital ward (nasal cannula) was insufficient. Table 1 provides an overview of these criteria.
Classification of medically essential admissions at the intermediate care unit
This table shows the criteria used to define whether an admission was medically essential or not. If one or more of the criteria are present, the admission is classified as medically essential.
Assessment of triage system: logistical criteria
In addition to using medical criteria to assess the triage system, logistical criteria were used. The classification of logistically correct admissions was based on the location of admission, admission duration (either <24 hours or ≥24 hours), and discharge location. Utilizations were defined as (A) correct, (B) incorrect due to undertriage, that is, patients were transferred to the ICU <24 hours after admission, or (C) incorrect due to overtriage, that is, IMCU patients originally admitted from the ICU or the recovery unit who were then transferred <24 hours to the hospital ward.
The rationale behind these criteria was that short admissions (<24 hours) were logistically undesired since they delayed necessary ICU care if transferred to the ICU within 24 hours, or increased unnecessary transfer of patients if transferred to the floor within 24 hours (if not admitted for a short monitoring period, which is likely the case in patients who are deteriorating in the hospital ward or the emergency room). A detailed flow chart is shown in online supplementary file 1.
Supplemental material
Assessment of triage system: combined criteria
The aforementioned medical and logistical criteria were combined to determine whether an admission was classified as (1) both logistically correct and medically essential, (2) logistically correct but medically non-essential, (3) logistically incorrect but medically essential or (4) logistically incorrect and medically non- essential.
Statistical analyses
Admissions due to bed overflow, specific invasive interventions and deaths within 24 hours were excluded from the analyses. The bed overflow patients were admitted from other disciplines due to full occupancy of their IMCU. Specific invasive interventions included procedures like placement of a chest tube or central venous line, for which a short period of monitoring was required. Deaths within 24 hours were, in part, admitted for palliative care. Hence, these admissions were believed not to reflect the overall nature of IMCU admissions.
Descriptive statistics presented are the mean and 95% CI for the continuous variable nursing workload (normally distributed). Categorical variables are described as numbers with proportions. The nursing workload and the medically essential admission rate were compared per location of admission with, respectively, the analysis of variance test and Χ2 test of independence. For the comparison of these outcomes per admission duration shorter or longer than 24 hours, the t-test and Χ2 test of independence were used, respectively.
To assess the difference in nursing workload and medically essential admissions with respect to management formats, interrupted time series analyses were performed to adjust for pre-existing time trends. This is a strong approach to evaluate the longitudinal effects of interventions, especially when an experimental trial is not feasible or ethical.13–15 The autocorrelation of these models was checked by examining the residual plots and the (partial) autocorrelation functions. To determine the effectiveness of the triage, we constructed a two-by-two table for the frequencies and proportions of medical and logistical criteria.
In 112 admissions (1.17%), the admission indication was missing from the electronic health records. These cases were excluded from the analyses. In 617 (6.5%) cases, the TISS-28 score was missing. To adjust for potential bias and imprecision caused by these missing data,16 17 multiple imputation (30 data sets, 30 iterations) was performed for the separate TISS items, after which the total TISS score was calculated. Categorical values over the imputed data sets were averaged and rounded. Continuous values were pooled using Rubin’s rules.
A significance level of 0.05 was used. All statistical analyses were performed using R software for statistical computing V.3.3.218 with the additional packages ‘mice’,19 ‘bootstrap’20 and ‘ggplot2’.21
Results
An overview of the baseline characteristics of admissions is provided in table 2. After exclusion of bed overflow (n=387), specific invasive interventions (n=306) and deaths within 24 hours (n=43), a total of 8816 admissions were included in analyses. The patients who died were either admitted to the IMCU for end-of-life care (ie, palliative care, n=22), admitted with the joint agreement not to transfer to the ICU (n=7), or admitted without any treatment limitations (n=14).
Baseline characteristics of study population
This table shows the baseline characteristics of the studied population at the IMCU of the University Medical Centre Utrecht, from 2001 until 2015.
Nursing workload
The average TISS-28 was 20.2 (95% CI 18.0 to 22.3), corresponding with 3.6 (95% CI 3.2 to 3.9) hours of direct patient-related work per patient per nursing shift. The maximum TISS-28 was 44, which was also the maximum TISS for those admitted longer than 24 hours. The highest 25% TISS at admission ranged from 24 to 44 with a mean of 27.6 (95% CI 22.1 to 33.1).
The mean TISS per admission location was 21.9 (95% CI 11.1 to 32.8) from the ICU, 21.1 (95% CI 10.2 to 31.9) from the recovery unit, 19.3 (95% CI 7.7 to 30.9) from the hospital ward, and 16.2 (95% CI 5.4 to 27.1) from the emergency room (p<0.001). Admission within 24 hours had an average TISS of 18.8 (95% CI 6.9 to 30.7), compared with a TISS of 20.8 (95% CI 9.4 to 32.2) in admissions longer than 24 hours (p<0.001).
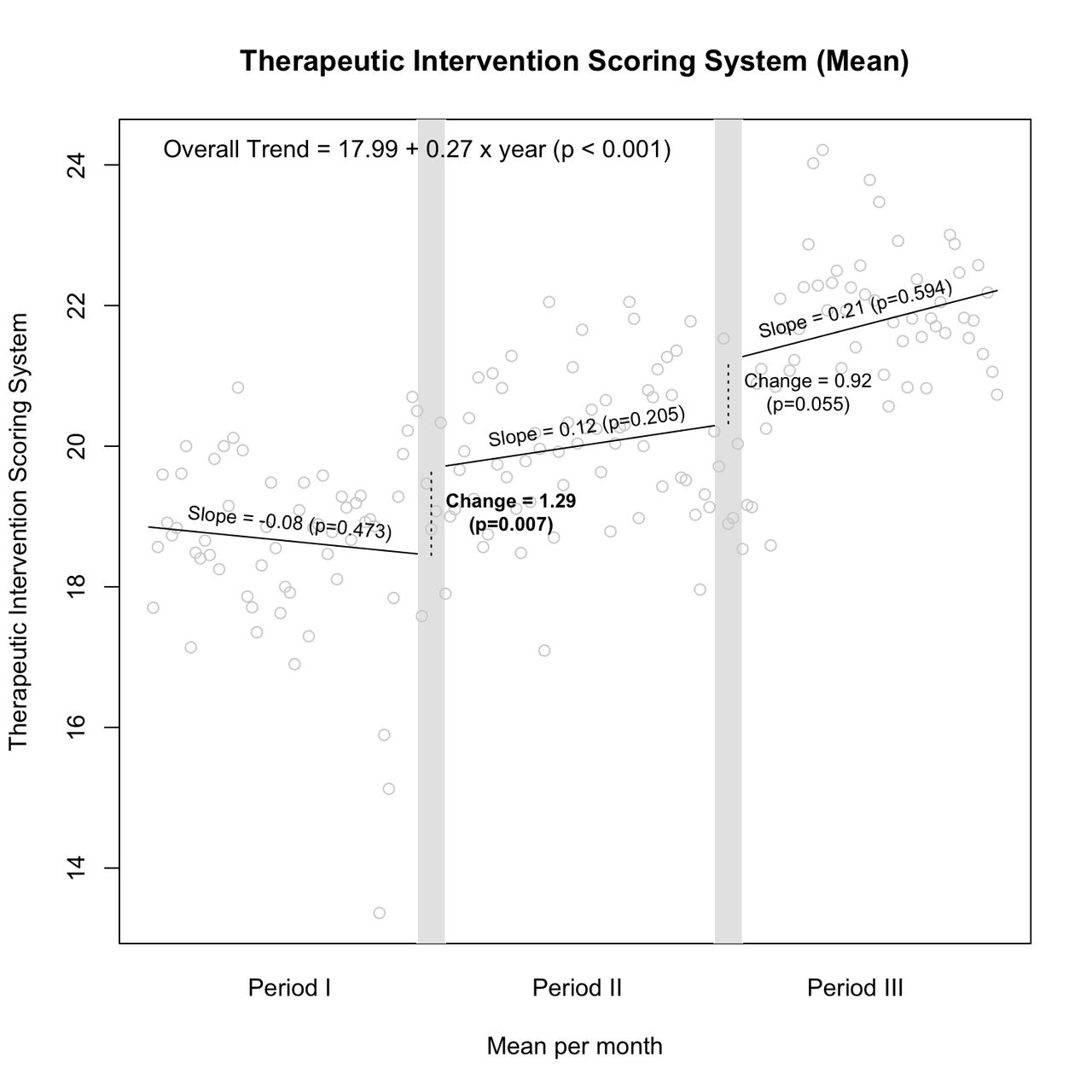
Over time, the mean TISS-28 increased by 0.3 points per year (p<0.001) (figure 1). The introduction of both the closed format (period II) and the joint format (period III) was associated with a stepwise increase in the TISS-28 of 1.3 (p=0.007) and 0.9 (p=0.055), respectively.
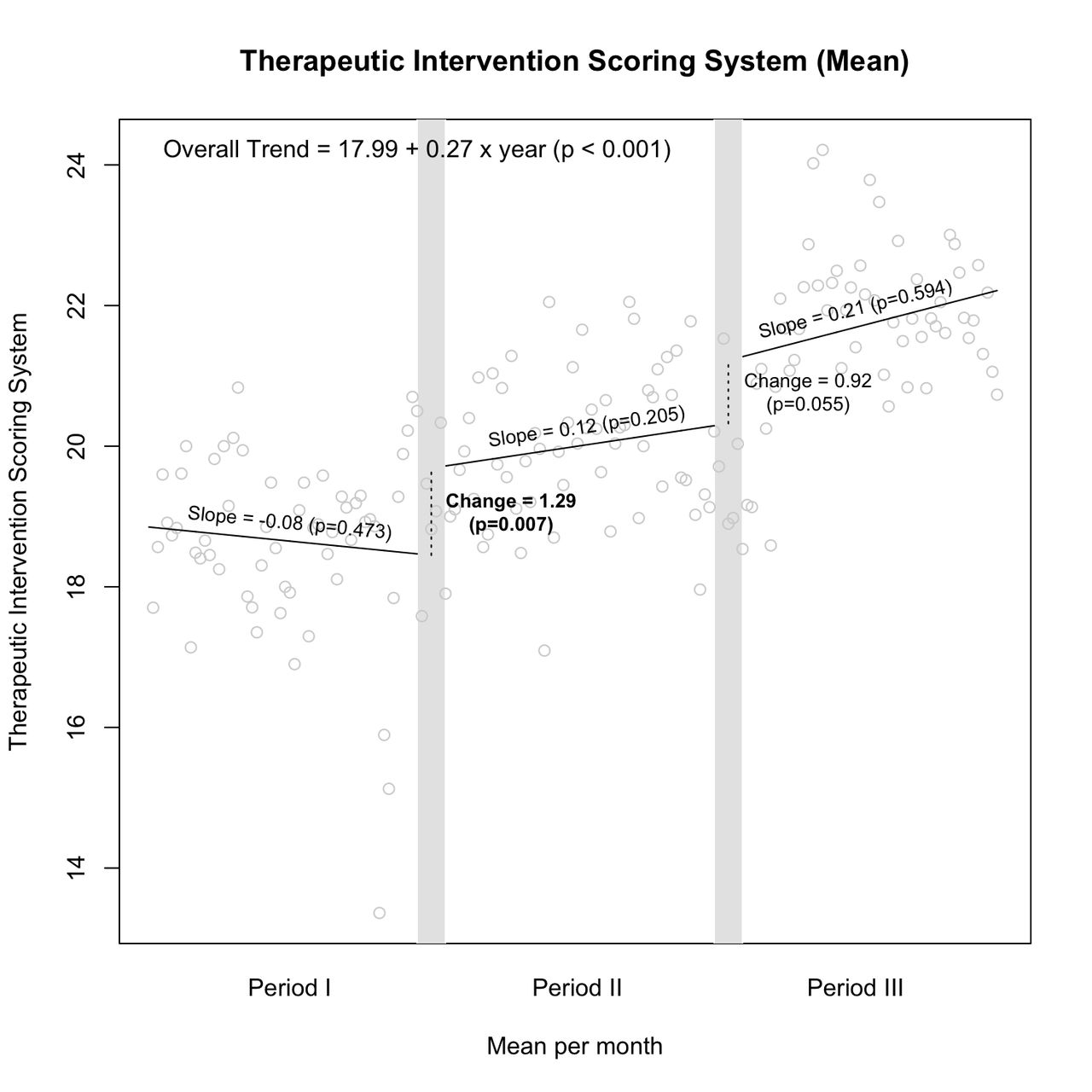
Therapeutic intervention scoring system per management format. Interrupted time series analysis. This figure shows the performed interrupted time series (ITS) analyses of the Therapeutic Intervention Scoring System (TISS) as a measure for the nursing workload.
Nursing activities
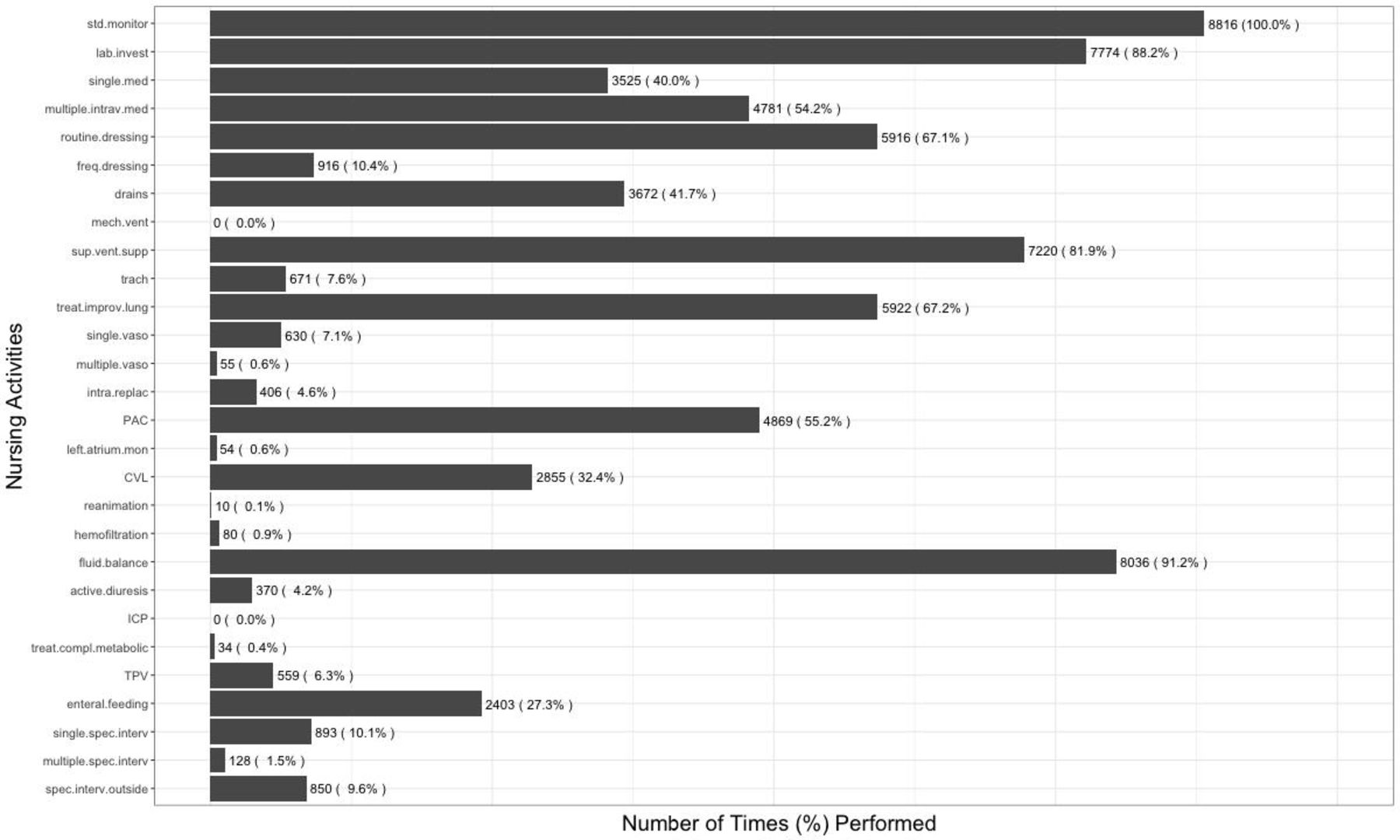
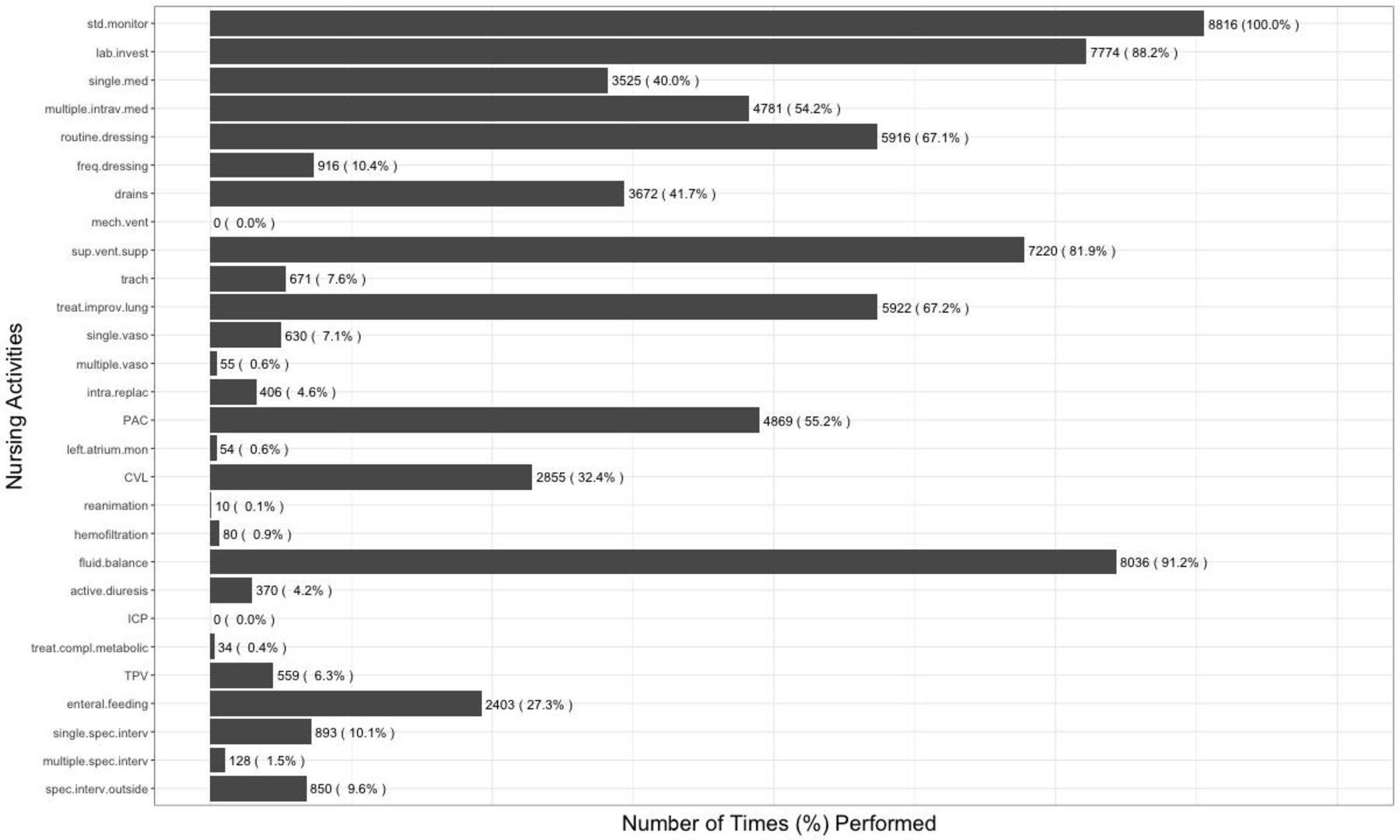
The nursing activities as reported in the TISS-28 and their relative frequencies are depicted in figure 2. All patients at the IMCU received standard monitoring (100.0%), and almost all patients underwent fluid balance control (91.2%), laboratory investigations (88.2%), supplementary ventilatory support (81.9%), treatment for improving lung function (67.2%), routine dressing changes (67.1%), peripheral arterial catheter placement (55.2%), multiple intravenous medications (54.2%), drain care (41.7%) and central venous line placement (32.4%). None received mechanical ventilation or intracranial pressure measurement, as these were limitations of the described IMCU.
{kind=link}
{kind=link}
Nursing activities at the intermediate care unit. This figure shows the performed nursing activities (as part of the Therapeutic Intervention Scoring System-28 list) at the intermediate care unit. active.diuresis, active diuresis; CVL, central venous line; drains, care of drains; enteral.feeding, enteral feeding through gastric tube or other gastro-intestinatl route; freq.dressing, frequent dressing changes; fluid.balance, quantitative urine output; ICP, intracranial pressure measurement; intra.replac, intravenous replacement of large fluid losses; lab.invest, laboratory investigations; left.atrium.mon, left atrium monitoring; mech.vent, mechanical ventilation; multiple.intrav.med, multiple intravenous medications; multiple.vaso, multiple vasoactive medications; multiple.spec.interv, multiple specific interventions in the IMCU; PAC, peripheral arterial catheter; reanimation, cardiopulmonary resuscitation after arrest in last 24 hours; routine.dressing, routine dressing changes; single.med, single medication use; single.spec.interv, single specific intervention in the IMCU; single.vaso, single vasoactive medication; spec.interv.outside, specific intervention outside the IMCU; std.monitor, standard monitoring; sup.vent.supp, supplementary ventilatory support; TPV, intravenous hyperalimentation; trach, care of artificial airways (tracheostomy); treat.compl.metabolic, treatment of complicated metabolic acidosis/alkalosis; treat.improv.lung, treatment for improving lung function.
Assessment of triage system: medical criteria
A total of 6539 (74.2%) admissions were medically essential. Overall, the amount of medically essential admissions increased by 0.9%/year (p<0.001). According to location of admission, there were 2689 (79.7%) medically essential admissions from the ICU, 1565 (75.3%) from the recovery unit, 1479 (81.8%) from the hospital ward, and 806 (51.8%) from the emergency room (p<0.001). Of all short admissions (<24 hours), 1728 (63.7%) were medically essential compared with 4811 (78.8%) admissions longer than 24 hours (p<0.001).
Assessment of triage system: logistical criteria
According to the logistical criteria for the assessment of the triage system at the IMCU, 7093 (80.5%) of all admissions were logistically correct. Of the remaining (logistically incorrect) admissions, 1389 (15.8%) were overtriaged admissions (from the ICU or recovery) and 334 (3.8%) were undertriaged admissions. Of the overtriaged admissions, 544 (6.2%) were admitted from the ICU, and 845 (9.6%) were admitted from the recovery unit.
Assessment of triage system: combined criteria
Table 3 shows the application of the combination of logistical and medical criteria to assess the triage system at the IMCU. A total of 492 (5.6%) admissions were patients admitted without logistical reasons or without receiving medically essential interventions at the IMCU. A total of 8324 (94.4%) admissions were correct based on our combined medical and logistical criteria.
Triage system at the intermediate care unit—application of combined logistical and medical criteria
Discussion
Based on a combination of medical and logistical criteria, almost all admissions are correctly triaged (94.4%). Furthermore, this study shows that admissions to the IMCU require a high nursing workload (TISS 20.2, or 3.6 hours of nursing work per patient per shift).
In comparison to this study, earlier research of the nursing workload at IMCUs reported a TISS of 23 (IQR 19 to 26) in a mixed-specialty IMCU, whereas another study in an internal medicine IMCU reported a TISS-28 of 5.8 (SD 2.8, open format) to 6.6 (SD 2.8, closed format).10 11 Both were situated in academic hospitals. The mean TISS for ICUs ranges from 26.2 to 32.3.11 This roughly indicates that the IMCU described in this study admits patients with two-thirds of the nursing workload of ICUs. At our institution, this is also reflected in the nurse-to-patient ratio, which is 1:1.5 at our IMCU and 1:1 at our ICU.
The nursing workload (TISS) at our institution was different based on management format, with a stepwise increase of 1.3 (p=0.007) from open to closed and 0.9 (p=0.055) from closed to joint format. This supports earlier research in which a higher TISS-28 was observed in a closed format compared with open format.10 It also suggests that the novel joint format admits a higher TISS-28 than both the closed and open formats. This supplements earlier research within the same IMCU, which showed that the joint format has an equal efficiency and safety (with a more complex caseload) compared with other formats.12
The criteria to classify admissions as medically essential (TISS ≥18, specific nursing activities, and admission indications) are arbitrary and have not been reported on previously. However, we believe they indicate whether patients could have been admitted to the hospital ward, although this also depends on the nurse-to-patient ratio and limitations of care that can be provided in the hospital ward. These proposed criteria can be used to assess the triage system at the IMCU and can explore the extent of unnecessary utilization of IMCUs.1 Since they reflect the necessity of IMCU admission, it is likely that the actual number of medically essential admissions is higher due to factors such as psychiatric diseases or manifestations (eg, delirium or suicidal behavior) requiring more extensive care.
We stress that logistical criteria should complement the medical criteria, since the intermediate position and capabilities of the IMCU also facilitate admissions for logistical reasons, such as the short monitoring of trauma patients and deteriorating patients from the hospital ward. Logistical criteria are possibly subject to more hospital management-based choices of where to provide which care rather than a direct consequence of triage decisions.
In conclusion, since admissions at the IMCU are infrequently incorrect, our findings show that criticism of the admittance of ward patients at the IMCU is unwarranted. This can have important management consequences in the ongoing debate of opening or maintaining the IMCU. Furthermore, physicians should consider the medical and logistical necessity of admissions to their IMCU to optimize its potential.
The strength of this study is that it is the first to define and apply both medical and logistical criteria to assess the triage system over a long period at the IMCU. It provides the tools to do so and creates platforms to discuss the assessment of this triage and the outcome parameters at the IMCU. Furthermore, our study size and time series analyses warrant powerful statistical analyses. Most importantly, it is the first study to show that unnecessary admissions at the IMCU rarely occur.
The limitation of this study is that not all logistical considerations at or outside of the IMCU are considered. The intermediate nature of the IMCU in combination with the scarcity of hospital resources makes IMCU admissions and discharges susceptible to the availability of beds at the IMCU and at other locations within the hospital. Therefore, an inadequate IMCU admission does not always reflect a shortcoming in the triage protocol. If these factors had been available for our analyses, it most likely would have increased the correct number of triages to the IMCU. Also, our predefined criteria are novel and therefore have not been validated on earlier research. Another limitation is that differences in the organization of IMCUs could limit direct application or comparison of our results to other IMCUs, although the stand-alone IMCU is nowadays a commonly used format.22
Conclusions
Most admissions to the IMCU are medically and/or logistically necessary, as the majority of admitted patients demand a higher level of nursing care than available on the general ward. Continuous triage is thereby essential. These findings support further utilization of the IMCU in our current healthcare system and have important implications for IMCU-related management decisions.
Acknowledgments
We thank Rogier Cantor for his efforts in extracting the required data.
References
Footnotes
Contributors JDJP made substantial contributions to design, data collection and data analysis and has actively participated in its interpretation. LMP made substantial contributions to the data analysis and interpretation and critically revised the article. JDJP and LMP were the main authors involved in drafting and finalizing the article. LPHL was involved in the design and critically revised the article. RMH made substantial contributions to conception and design and critically revised the article. FH contributed to the design and actively participated in data collection, analysis and its interpretation. He was involved in drafting the article and revising it critically. LPHL, RMH and FH have given final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.