Article Text

Abstract
Background The management format of the mixed-surgical intermediate care unit (IMCU) affects its performance. A format of combined supervision of surgeons with additional critical care certifications and admitting specialists, named the “joint format”, may herein be a promising new model of specialized critical care. This study aims to assess the performance of the joint management format.
Methods This observational cohort study compared three IMCU management formats at the stand-alone, mixed-surgical IMCU of a tertiary referral hospital using interrupted time series analyses. All admissions from 2001 until 2015 were included. Predetermined criteria for performance (utilization, efficiency, and safety) were applied to three different management format periods: open (2001–2006), closed (2006–2011), and joint (2011–2015) formats.
Results A total of 8894 admissions were analyzed. In terms of case load (utilization), there was an overall increase in the number of surgical patients (0.25%/year) (p<0.001), age (0.38/year) (p<0.001), and readmissions from the ward (0.16%/year) (p<0.001) and from the intensive care unit (ICU) (0.17%/year) (p=0.014). In terms of efficiency, the admission duration decreased (1.58 hours/year) (p<0.001). Transfer to the ICU within 24 hours, readmission within 24 hours from the ward, and unplanned mortality (eg, safety) did not change over time.
Discussion At a time of increasingly complex case load, the joint format at the mixed-surgical IMCU is an efficient and safe management format in which the admitting specialist continues to provide specialized care. Specialty-specific supervision at IMCUs is a safe option which should be considered in healthcare policy decisions.
Level of evidence Level IV.
- critical care organization
- high dependency unit
- intermediate care unit
- management format
- surgical critical care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- critical care organization
- high dependency unit
- intermediate care unit
- management format
- surgical critical care
Introduction
The intermediate care unit (IMCU) can fulfill an important role in our hospitals. Logistically situated between the hospital ward and the intensive care unit (ICU), the IMCU provides hemodynamic and respiratory support for deteriorating patients from the hospital ward, admits patients in need of extensive (postoperative) monitoring, and serves as a buffer unit to facilitate earlier discharge from the ICU.1
The IMCU can be configured differently in different hospitals due to local hospital profile and needs.2 Through knowledge of the actual effects of (differences in) configurations of the IMCU, the best hospital-specific design can be chosen.3 One crucial aspect of the IMCU configuration is the management format.
The choice of management format has been a subject of debate in the ICU literature,4–7 but for the IMCU only few studies have been performed.8–10 However, these studies focused on the effects of IMCU management formats on the utilization of the ICU,9 did not compare different management formats,10 or compared formats along with a physical relocation of the unit.8
The IMCU management format has important potential effects on the utilization and efficiency of the IMCU. Further, specialty-specific—surgical—involvement in the critical care process may be beneficial for the patient and thus improve patient outcomes.6
Management format can be distinguished into high-intensity staffing (mandatory intensivist consultation) or low-intensity staffing format,4 or into being either closed, with an intensivist or generalist in charge, or open, with the admitting specialist in charge. In this article, we use the latter distinction and we propose a new concept of the so-called joint staffing format, which was recently implemented in our hospital. In this management format, supervision of dedicated surgeons with additional critical care certifications is provided in collaboration with specialty-specific knowledge of admitting specialists.
The aim of this study was to assess the effects of the open, closed, and joint format of the IMCU on its performance in terms of utilization, efficiency, and safety.
Methods
Study design and setting
This was an observational cohort study comparing three different IMCU formats using interrupted time series (ITS) analyses. The study setting was the stand-alone, surgical IMCU of the University Medical Center Utrecht, a tertiary referral academic hospital in the Netherlands which also functions as a level 1 trauma center. All admissions to this IMCU between January 1, 2001 and December 31, 2015 were included. All data were prospectively collected.
Study variable
The variable of interest was the management format at the IMCU. Over the studied period, the IMCU medical team consisted of surgical trainees—available 24/7—which were supervised according to three different management formats in different time periods:
Period I (January 2001–February 2006). The IMCU of the University Medical Center in Utrecht has started off (in 1998) as a stand-alone, four-bedded unit adjacent to the surgical hospital ward. Its management format was open, with the admitting surgeon directly in charge. In this period, the hospital had a dedicated surgical ICU with surgical intensivists in charge, assisting at the IMCU if required.
Period II (February 2006–May 2011). In 2006, as all ICUs in the Netherlands changed to closed format ICUs led by intensivists, the IMCU transformed accordingly. In this period, the IMCU increased in size to a five-bedded unit and had a closed format. Throughout this period, the management format changed between anesthesiological intensivists, surgical intensivists, and internal medicine intensivists.
Period III (May 2011–December 2015). Due to an expected increase in caseload complexity, the management format in the IMCU transformed again. The IMCU further increased in size to six beds, with one (seventh) additional bed dedicated to specific interventions in ward patients, such as the insertion of a chest tube or central venous catheter. In this period, responsibility for the patient was taken up jointly, with dedicated supervision of trauma surgeons with additional critical care certifications for hemodynamic and respiratory stabilization, while the admitting—surgical—specialist remained in charge of their patients. We will refer to this form of patient management as “joint format”.
Study outcomes
We categorized the study outcomes into utilization, efficiency, and safety of the IMCU. These three aspects are thought to be important in assessing the performance of the IMCU. Utilization indicates how the IMCU is used, in terms of case load and complexity. Efficiency indicates the minimization of overtriage at the IMCU. Safety indicates patient safety at the IMCU. The following parameters were used to study these aspects:
Utilization. Information was collected on the number of admissions, admission durations, and admission and discharge location. As other measures for the utilization of the IMCU, the number (%) of readmissions and time until readmission were analyzed. As an approximation of the admitted caseload complexity, the nursing workload (Therapeutic Intervention Scoring System-28) of admissions was analyzed.11 A readmission was defined as a secondary admission within 2 weeks during the same hospital admission. Both these parameters were analyzed separately for readmissions from the ICU and from the hospital ward.
Efficiency. To assess overtriage at the IMCU, the location of admission, admission duration, and discharge location were used. Admissions were classified as overtriage if a patient from the ICU or recovery was redirected to the hospital ward within 24 hours, since this was potentially an unnecessary extra patient transfer. Admissions from the ward or emergency room who were redirected within 24 hours to the hospital ward were not considered overtriage; these were, respectively, deteriorating and newly presented patients in need of a short period of monitoring.
Patients who were admitted for a specific intervention (eg, placement of a chest tube) and those who died within 24 hours of admission were excluded from these analyses, since their appropriateness of IMCU stay could not be determined.
Safety. The percentage of incorrect admissions due to undertriage of needed level of care (defined as a transfer to the ICU within 24 hours after admission), the amount (%) of readmissions from the hospital ward within 24 hours, and the unplanned mortality at the IMCU were used.
Early ICU transfer was considered a possible delay of necessary ICU care and therefore a safety parameter.12 Readmissions from the hospital ward within 24 hours were also considered to be a potential hazard for patient safety, since this potentially indicates a too early discharge of admitted patients. For the unplanned mortality, a distinction was made between patients with and without restrictions on treatment, whereas the area of interest was patients without restrictions on treatment.
Statistical analyses
In the statistical analyses, data of the quarter (3 months) before and at transition from one period to another were not used, such that the transition phase was excluded from analyses. Hence, for the transition from open to closed format (from period I to II) the months October 2005 up to and including March 2006 were excluded, and for the transition from closed to joint format (from period II to III) the months January 2011 up to and including June 2011 were excluded from the analyses.
In the descriptive analyses, for continuous variables the 95% bootstrapped and accelerated CIs were reported. For categorical variables, the percentage of occurrence was reported. In the univariate analysis, differences between the three periods were assessed using analysis of variance tests for continuous outcomes and χ2 tests for independence.
To adjust for possible linear time trends, ITS analyses were performed using segmented regression analysis. This has been shown to be a strong approach to evaluate longitudinal effects of interventions when an experimental trial is not feasible or ethical.13–15 The ITS approach in this study was used to determine whether observed differences in periods could be explained by underlying time trends or could be ascribed to the changing of management formats (the intervention). For this, analyses of quarterly bins were performed. The autocorrelation of the linear models was checked by examining the residual plots and the (partial)autocorrelation functions. To analyze whether ceiling or floor effects were present, the outcomes as percentages were also logit-transformed, using empirical log transformation,16 to investigate whether different results were obtained.
Since acute pancreatitis and esophagectomy (due to cancer) patients are subgroups which are known to frequently develop complications with subsequent IMCU care,17 18 trends in the admittance of these specific patient subgroups at the IMCU were also analyzed.
Missing values rarely occurred in the data. In only 104 patients, information on the specialty admitting the patient was missing. As this was due to insufficient information in the electronic files, we expect this to be missing completely at random; hence, complete case analyses were performed.
Throughout the analyses a level of significance of 0.05 was used. All analyses were performed using R V.3.3.2 software for statistical computing,19 with the additional packages “ggplot2”20 and “bootstrap”.21 The ITS analyses were based on an example R Script.15
Results
An overview of the admission characteristics and utilization, efficiency, and safety parameters in the three study periods is provided in table 1. A total of 8894 admissions were included in the analyses.
Utilization, efficiency, and safety of the intermediate care unit for the three periods
Age, number of surgical patients, and nursing workload were significantly higher in period III (p<0.001), whereas admission duration was lower (p<0.001) and readmission rates from both the hospital ward (p=0.012) and the ICU were higher (p<0.001).
The rate of overtriaged admissions from the recovery unit was higher in period III (p<0.001). No difference was observed in overtriaged admissions from the ICU (p=0.740). The rate of readmissions within 24 hours from the hospital ward was higher in period III compared with the other periods (p=0.029). Also, unplanned mortality of patients without a non-ICU policy was absent in period III (p=0.002).
Time trends: ITS analyses
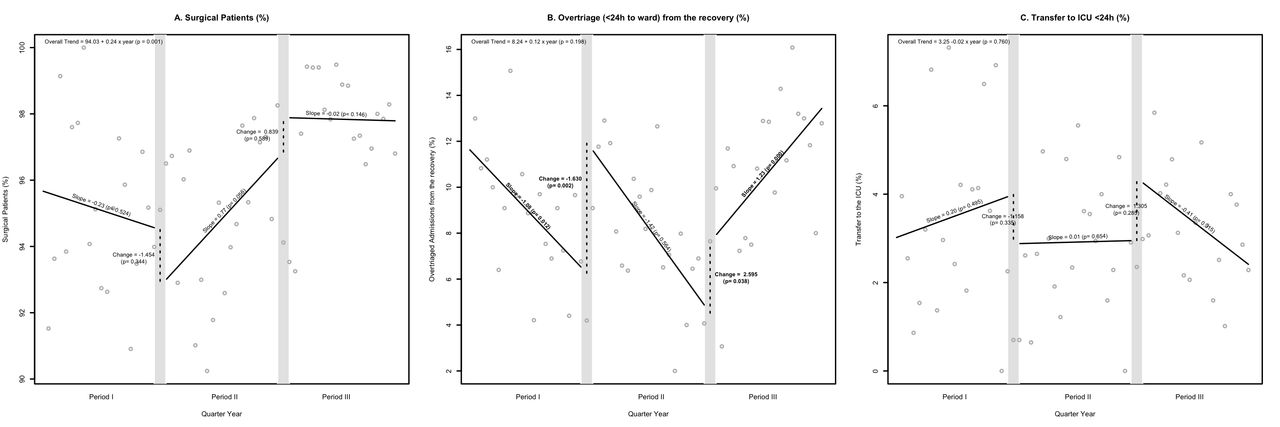
Of each of the measured outcome levels—utilization, efficiency, and safety—one graph of the observed time trends with corresponding p values is shown in figure 1A–C (all ITS graphs are shown in online supplementary file 1).
Supplemental material
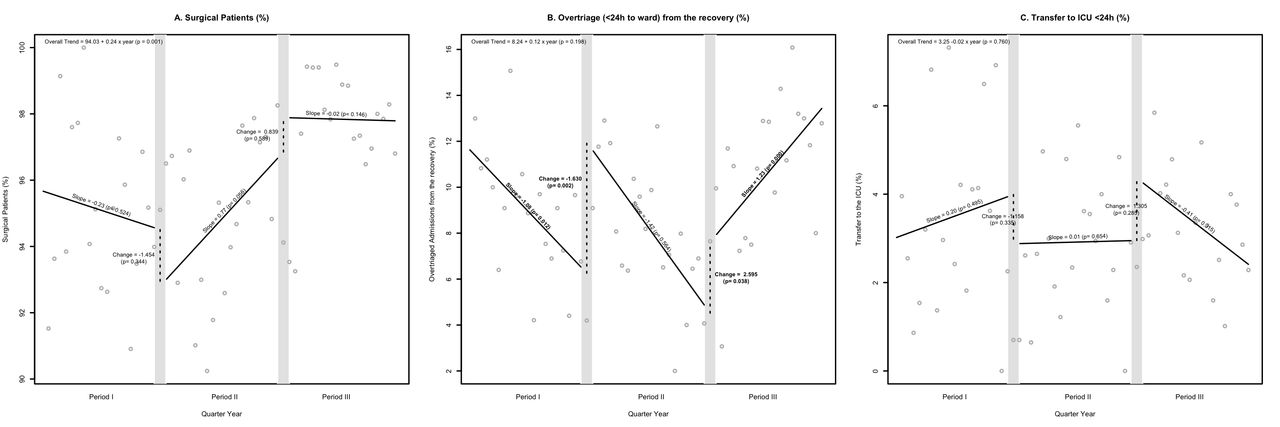
Different management formats and utilization, efficiency, and safety at the intermediate care unit: an ITS analysis. This figure shows the performed ITS analyses on three examples: mean age (A, utilization), number of incorrect admissions from the recovery ward (B, efficiency), and discharge to ICU rate (C, safety). The gray dots represent the average observed values per quarter year, and the gray bars represent the transition period between one format and the other (these values are excluded from the analyses). The overall trend is shown in the upper left corner. The segmented linear regression lines show the slope per period and the change in level after an introduction of another format. Of the slopes, the p values at period I shows the significance of this slope itself, whereas the p values at the slopes of periods II and III show whether this slope has changed significantly from the period before. The p values of the change in level show whether this direct change was statistically significant. ICU, intensive care unit; ITS, interrupted time series.
The ITS graphs show that there was overall an increasing trend in surgical patients (0.25%/year) (p=0.001) (figure 1A) and age (0.38/year) (p<0.001), and a decrease in average admission duration (−1.49 hours/year) (p<0.001). Overall, the readmissions from the hospital ward (0.16%/year) (p<0.001) and the ICU (0.17%/year) (p=0.014) increased.
Overall, transfer to the ICU rate (0.02% decrease/year) (p=0.629) (figure 1C) and readmissions within 24 hours from the hospital ward (0.05% increase/year) (p=0.114) increased, and unplanned mortality (0.02% decrease/year) (p=0.184) did not significantly change.
Subsequently, the effect of the different management formats on the outcomes was analyzed. First, the joint format was compared with the closed format. From this, it follows that the joint format increased the readmissions from the ICU with 4.19% (p=0.004). This effect was absent in readmissions from the ICU within 24 and 48 hours at the ICU. The joint format also increased the average number of overtriaged admissions from the recovery with 2.60% (p=0.038) (figure 1B) and with a further 1.23%/year (p<0.001). In comparison of the joint with the open format, no significant changes were found except for a higher overtriage from recovery of 7.59% (p=0.016) and decreased slope of −0.58%/year (p<0.001). Also, a different slope of overtriages from the ICU of −0.43% per year (p=0.045) was observed.
The residual plots and (partial) autocorrelation function plots showed very little evidence of autocorrelation. Logit transformation of the percentage outcomes showed similar results, except for the increase in readmissions from the ICU (from period II to III), which was no longer statistically significant.
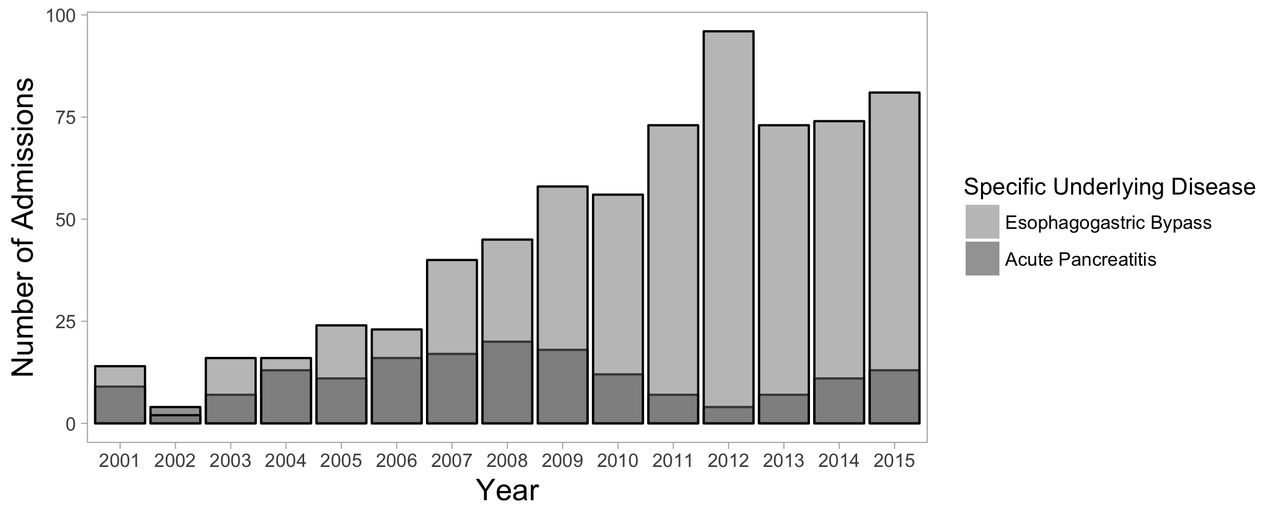
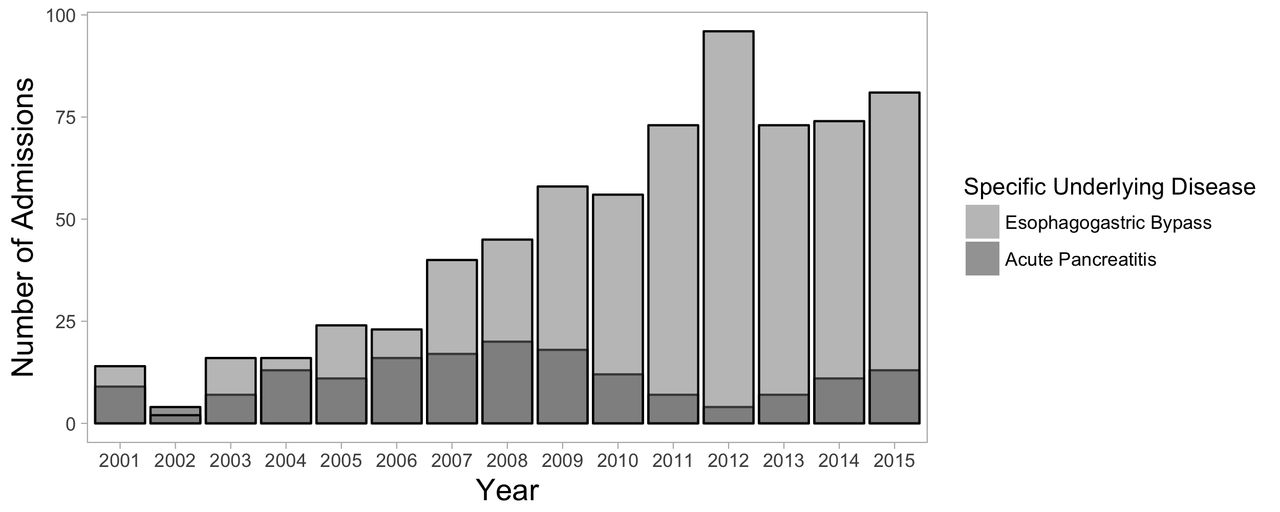
The case load at the IMCU in terms of patients with acute pancreatitis has increased from 2001 (n=9, 1.55%) to 2008 (n=20, 3.10%), after which it decreased to 13 (1.67%) in 2015. The case load in terms of esophagectomy patients has increased from 14 (2.41%) admissions in 2001 to 81 (10.39%) in 2015 (figure 2).
{kind=link}
{kind=link}
Admissions with acute pancreatitis and esophagogastric bypass at the intermediate care unit. This figure shows the number of admissions with acute pancreatitis and with esophagogastric bypass.
Discussion
This study is the first to propose and assess the effects of the joint staffing format compared with the commonly used closed and open formats. The performance of this management format was evaluated in terms of utilization, efficiency, and safety. ITS analyses were performed to distinguish between underlying general time trends and probable effects of the management formats.
Observed overall time trends at the IMCU in the studied period were an increasing percentage of surgical patients, increasing age, increasing nursing workload, and decreasing admission duration. Readmissions (>24 hours after IMCU discharge) from both the hospital ward and the ICU increased. Increasing age, nursing workload, and readmissions are likely to reflect an increased caseload severity at the IMCU. Readmissions are frequently a consequence of increased caseload severity, as more critically ill (surgical) patients are more prone to develop complications. Complications would then lead to a secondary transfer from the ward to the IMCU, or from the IMCU to the ICU and back. Also, as this study covers a period of 15 years, an increased caseload complexity (which is the overall trend) is to be expected.22 23 The increasing prevalence of (high-complex) esophagectomy patients at the IMCU further supports this finding.
The decreasing admission duration can probably be explained by (1) specific clinical pathways at our institution, such as patients undergoing hyperthermic intraperitoneal chemotherapy and enhanced recovery after surgery protocols after colectomies for colon carcinomas24; (2) increased level of training of the IMCU nurses; (3) a more strict adherence to the IMCU requirements in a situation with ongoing shortage of hospital resources; and (4) an increased pressure on available IMCU (and ICU) beds due to this ongoing shortage of resources.
Efficiency, in terms of overtriage from the ICU or recovery, did not significantly change over time. Most importantly, although an increased caseload severity was observed over time, transfer-to-the ICU rate, readmissions within 24 hours from the hospital ward and unplanned mortality did not significantly change. Hence, the safety of admissions at the IMCU was maintained even though the case load increased.
As for the (immediate) effects of the different management formats on utilization, efficiency, and safety, the following changes were observed. First, there were significantly more readmissions from the ICU in the joint format; this effect, however, was absent in readmissions from the ICU within 24 and 48 hours and was also absent in the logit-transformed analyses. Hence, this does probably not indicate an earlier, too safe, transfer to the ICU, but rather an increased admitted caseload severity at the joint format: the admitted patients more often require extended care at the IMCU and therefore necessary ICU transfer. Second, the joint format significantly increased the overtriage from the recovery unit. This is probably explained by a hospital policy of less recovery beds, which enhances the use of the IMCU as an extended postrecovery unit.
This study complements earlier research that has focused on the comparison between high-intensity and low-intensity staffing at the IMCU in that there are no significant differences in terms of mortality, although our comparison was between the open and closed formats (thus, not the intensity level).8 It thereby introduces the joint format and applies other outcome measures: logistical measures such as utilization and efficiency, and patient safety parameters such as ICU transfer and early readmission from the ward. These measures were thought to more adequately reflect the quality assessment in intermediate units. Furthermore, the low mortality rate hampered its use as a valid, comparable outcome measure.
At first, these results may seem to contradict the finding that the closed (or high-intensity) format at the ICU reduces the in-hospital mortality among ICU patients.4–7 However, in the surgical subpopulation of trauma patients, this mortality reduction was strongest with the surgical intensivist in charge.6 Potentially therefore, specialty-specific critical care is safe and desired (for trauma patients) for the ICU and for the (surgical) IMCU. Furthermore, if we were to classify the joint format (trauma surgeons with additional critical care certifications) as ‘high-intensity format’ due to mandatory ‘intensivist’ consultation, our results are in favor of the high-intensity format and thereby align with its observed beneficial results at ICUs.
The strength of this study is its large study size covering a long time period with an ITS analysis. Such an analysis offers the ability to distinguish between time effects and intervention effects.13–15 Furthermore, this study assesses the performance of the IMCU with logistically oriented quality parameters which are directly measured at the IMCU. Most importantly though, this study is the first to propose and critically assess the novel joint format, and with it the direct surgical involvement in the daily management format at the IMCU.
A limitation of this study is that it does not consider issues of occupancy rate, while—in a time of full capacity—a patient in need of IMCU care may trigger a chain of events that alter triage decisions in further admissions. Another potential limitation of our study is to which extent our findings are generalizable to other IMCUs. However, all IMCUs do share common characteristics and the here reported stand-alone, open format surgical IMCU is one of the most commonly used.2 Also, increasing caseload severity is a phenomenon that is seen worldwide.22 23 Therefore, we expect these results are likely applicable to other IMCUs as well.
Furthermore, we realize that over the course of time, other changes in the clinical care process may have taken place that influence patient outcomes, such as the introduction of laparoscopic procedures instead of open abdominal surgery, or the change from open to endovascular aneurysm repair. We have not explicitly modeled these in our analyses; however, with the ITS analysis, such changes in patient outcomes over time are modeled implicitly, and the analysis serves to investigate whether “additional” changes in patient outcomes have taken place with the change of management format.
Conclusions
The joint management format is a collaboration between admitting specialists and specialty-specific critical care specialists. We showed that in a period with increasing caseload severity, this joint format has proven an efficient and safe management format.
With the specialist continuing to provide specialized care, this may be a promising new model which can fulfill an important role in our current healthcare system. Surgical supervision at IMCUs is a safe option which should be considered in healthcare policy decisions.
References
Footnotes
Contributors JDJP made substantial contributions to design, data collection, data analysis and the interpretation of the results. JDJP was the main author involved in drafting and finalizing the article. LMP made substantial contributions to the data analysis and interpretation and critically revised the article. LPHL was involved in the design and critically revised the article. RMH made substantial contributions to conception and design and critically revised the article. FH contributed to the design and actively participated in data collection, analysis and its interpretation. He was involved in drafting the article and revising it critically. JDJP, LMP, LPHL, RMH and FH have all given final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval According to the Institutional Review Board of the University Medical Center Utrecht, the study was not subject to the Medical Research Involving Human Subjects Act and therefore the necessity of informed consent was waived (protocol number 17-326/C).
Provenance and peer review Not commissioned; externally peer reviewed.