Article Text

Statistics from Altmetric.com
A 63-year-old patient arrived at our trauma center with profuse arterial bleeding from zone 2 on the right side of his neck. He was alert with a heart rate of 130 beats per minute and a blood pressure of 150/100 mm Hg. There was initial confusion regarding what had precipitated the bleeding. The patient clearly had undergone prior head and neck operation and radiation, marked by a chronic ulcerated wound with extensive fibrosis around the bleeding site and a laryngectomy stoma. The latter was quickly intubated and the patient resuscitated with blood products. Manual compression was applied to the bleeding site.
We later learned that a scab had recently formed at the site and the patient had displaced it while shaving, eliciting the hemorrhage from a partially exposed right common carotid artery. Unbeknown to our team, the patient’s medical history was significant for squamous cell carcinoma of the larynx treated more than 15 years ago.
Given the complexity of his cervical wound, the decision was made to proceed to the angiography suite, where an endovascular stent was successfully deployed to exclude the arterial defect and hemostasis. This allowed the wound to be fully visualized, revealing that the stent was exposed within the artery (figure 1).

Exposed stent in the right common carotid artery (arrow) within a chronic ulcerated fibrotic wound on the right side of the patient’s neck. An endotracheal tube inserted through the tracheal stoma for airway protection (star).
The patient recovered in the intensive care unit (ICU), and he was neurologically intact on antiplatelet medication. A few days later, a latissimus dorsi free flap was performed over the exposed segment of the stented right carotid. Unfortunately, the flap failed and the artery along with the stent were exposed again. Two weeks later the patient developed another massive arterial bleed from the exposed artery on the ward. The patient was reintubated through the tracheal stoma and manual compression applied to the bleeding site.
What would you do?
Proceed to the operating room
Proceed to the angiography suite to restent the carotid artery
Ligation of both ends of the carotid artery at the bedside
What we did and why?
Correct answer: A
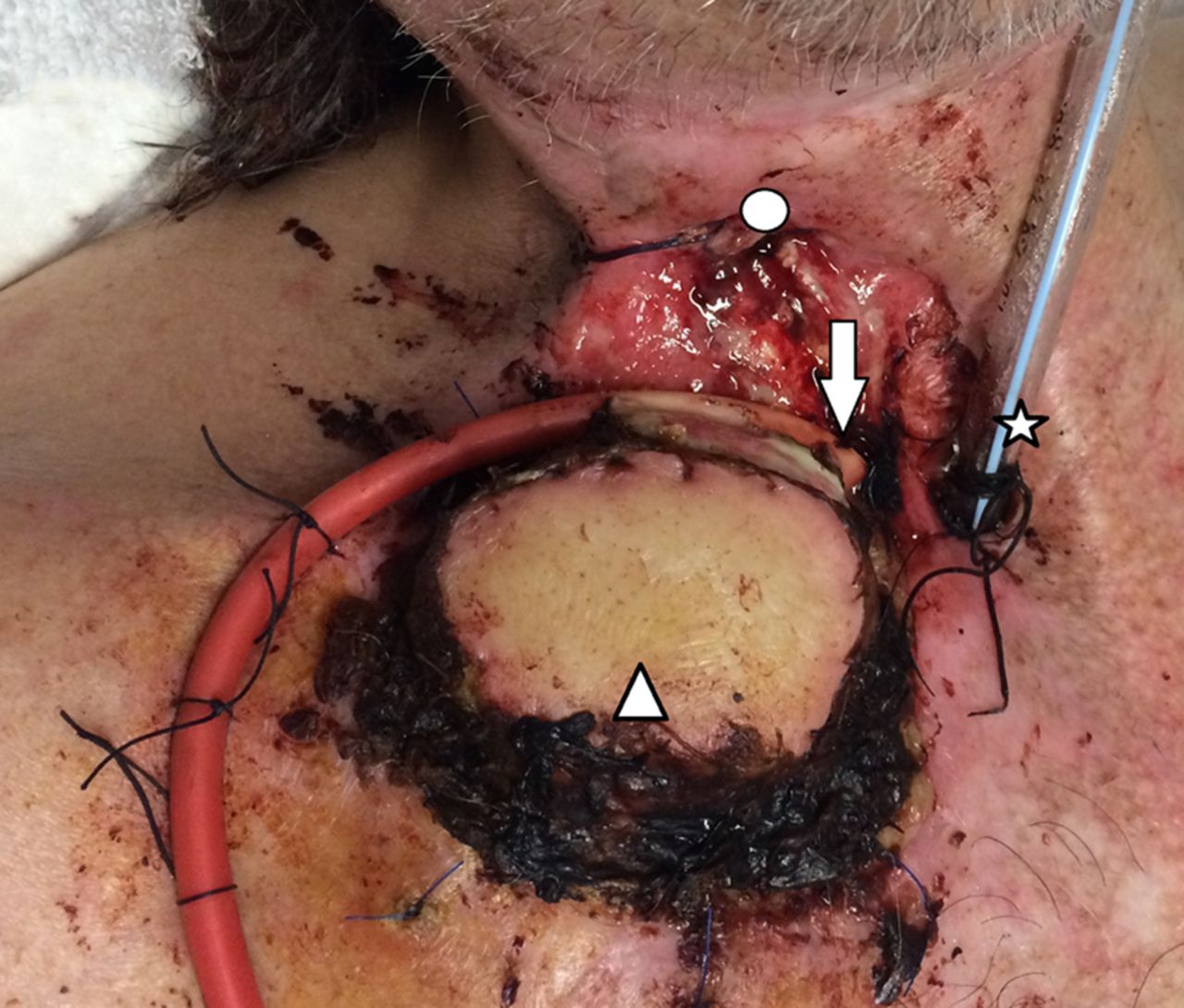
In the operating room (OR) the team was able to adequately assess the extent of right carotid artery disruption. Essentially, the stent had completely dislodged from the carotid, leaving the artery in discontinuity at the base of the ulcer. Due to the friability and fibrosis of the tissues, and retraction of the proximal artery deep into the neck, the decision was made to introduce a 14F Foley catheter into the proximal end of the artery as a damage control strategy. The Foley was easily inserted and the balloon was inflated, anchoring it at the level of the innominate artery after slight traction. The external portion of the Foley was clamped with two Crile clamps. The distal end of the artery was suture ligated with 2–0 silk for total hemostasis (figure 2).
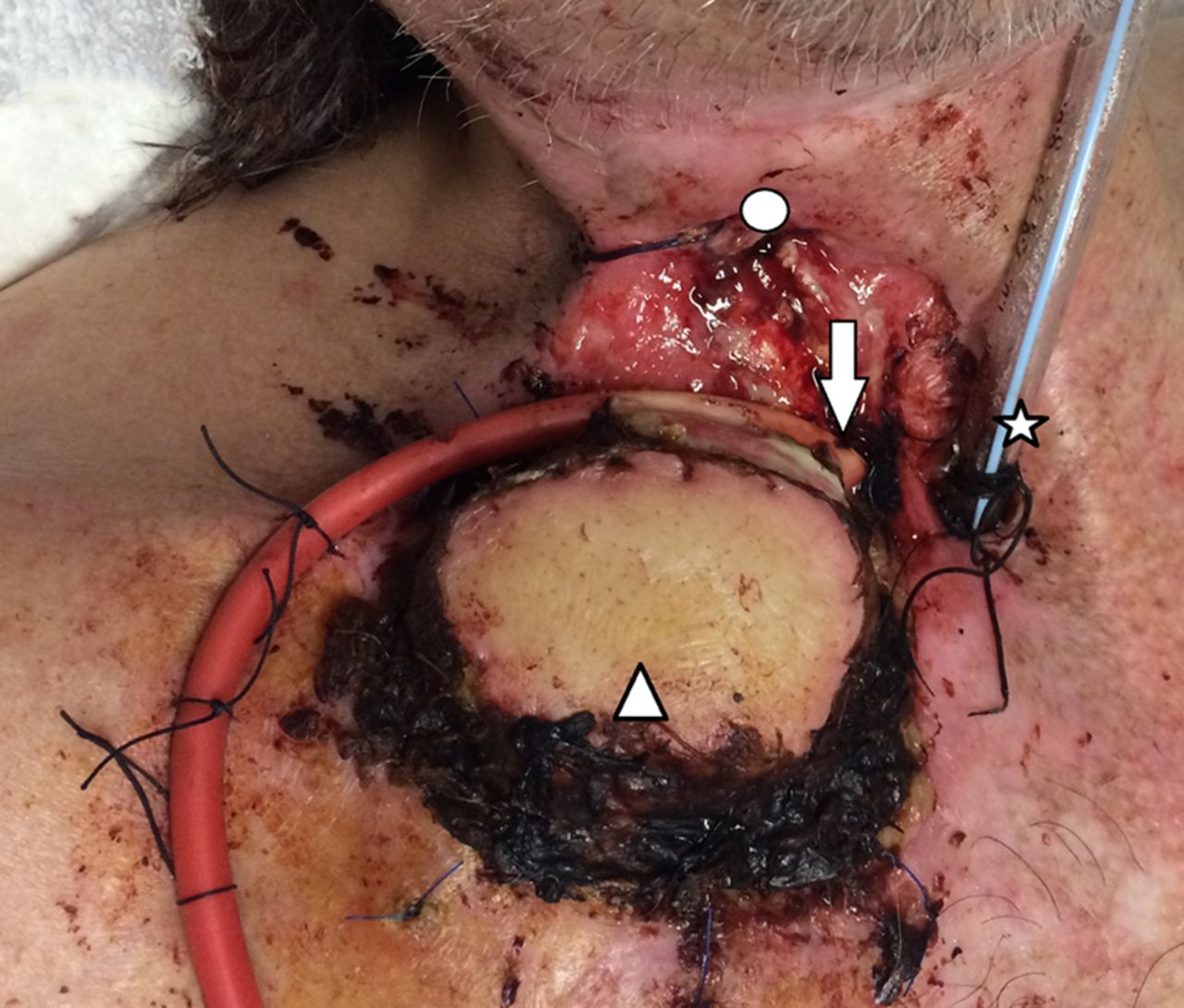
Foley catheter inserted in the proximal end of the disrupted right carotid artery (arrow). Suture ligation of the distal end of the right carotid artery (circle). Necrotic latissimus dorsi flap (triangle). An endotracheal tube inserted through the tracheal stoma for airway protection (star).
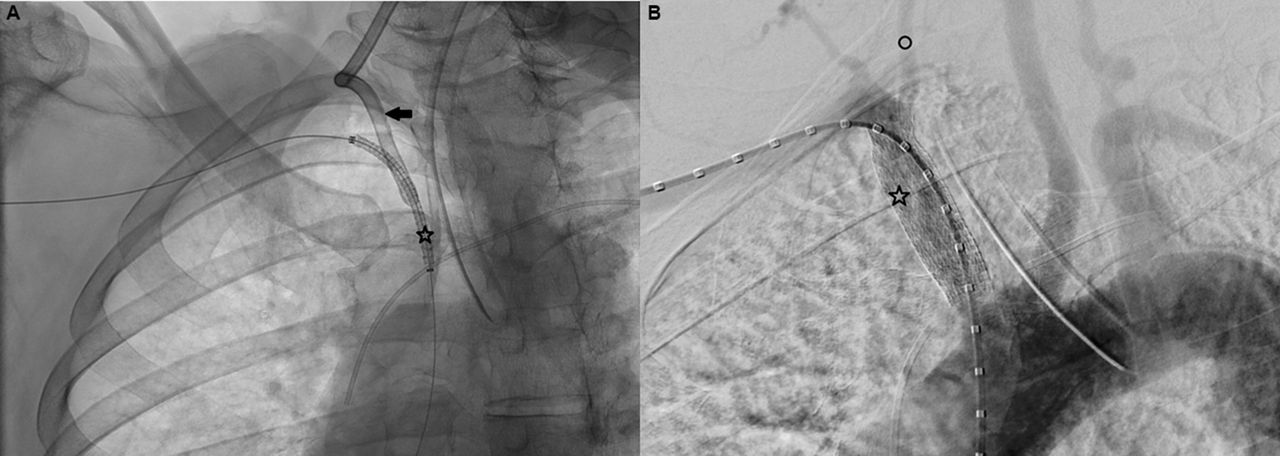
The patient recovered in the ICU for approximately 36 hours and was subsequently taken to the OR for definitive management. A rendezvous approach involving interventional radiology and general operation was chosen to simultaneously remove the Foley catheter and deploy a covered stent. Specifically, via access through the right brachial artery, a 13×50 mm covered stent (Viabahn Gore, WL Gore & Associates, Flagstaff, AZ) was advanced under fluoroscopy and positioned just proximal to the Foley in the right innominate artery. At that point, the balloon was deflated and the Foley catheter pulled back into the right common carotid artery while the stent was simultaneously advanced to a satisfactory position for deployment in the right innominate artery, across the origin of the right common carotid (figure 3). An angiogram revealed successful exclusion of the right common carotid and a patent right vertebral artery. The latissimus dorsi flap was excised at the end of the procedure. The patient presented slight weakness on his right arm and leg postoperatively. Follow-up CT scan showed bilateral subacute posterior cerebral artery infarcts. Two months later, the patient had significant neurologic improvement and was discharged home. Investigation showed that he remained cancer-free. The neck wound was covered with a split thickness skin graft.

{kind=link}
{kind=link}
{kind=link}
(A) Depicts the stent in the innominate artery (star) adjacent to the Foley catheter in the right common carotid artery (arrow) as it was being removed prior to the deployment of the stent. The balloon was deflated. (B) Shows poststent deployment (star) and complete occlusion of the right common carotid artery. The right vertebral artery remains patent (circle).
Hemorrhage from a ruptured carotid artery, as a delayed complication related to primary head and neck cancer and salvage head and neck operation, is called carotid blowout syndrome (CBS). This complication occurs in 3% to 4% of all head and neck cancers and bears a mortality rate of approximately 40%. The overall neurologic morbidity associated with CBS is 60%. Previous reports showed that this syndrome has three different presentations: type I or threatened CBS involves an exposed intact vessel following head and neck cancer treatment; type II or impending CBS pertains to transitory hemorrhages that resolve spontaneously or with packing; and type III is an acute CBS with massive bleeding.
A recent meta-analysis of 25 studies involving 559 patients showed that coil embolization and stent graft were used in 90% of the patients in CBS types I and II. Hemorrhage control was initially achieved in every patient with a perioperative stroke rate of only 1%. Rebleeding rates were 17% in patients treated with coils and 34% for stent grafts. Interestingly, 51% of the patients included in that meta-analysis were reported to have had acute bleeding on initial presentation, possibly type III CBS. Unfortunately, the actual severity of those cases at presentation was unclear. This is relevant fact in the management of CBS given that patient outcome is predicted by the severity of the initial presentation according to previous studies.
Our patient was notably challenging considering the massive rebleed of type III CBS. Surgical treatment would be technically difficult given the fibrosis of previously irradiated tissues. An endovascular approach alone was ill-advised considering the massive hemorrhage from the common carotid artery in the presence of hemodynamic instability. Therefore, a damage control strategy to temporize the bleeding followed by less invasive endovascular treatment was a suitable option for this case.
Footnotes
Contributors All authors contributed to this work.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.