Article Text

Abstract
Background Previous studies have demonstrated a significant relationship between weather or seasons and total trauma admissions. We hypothesized that specific mechanisms such as penetrating trauma, motor vehicle crashes, and motorcycle crashes (MCCs) occur more commonly during the summer, while more falls and suicide attempts during winter.
Methods A retrospective review of trauma admissions to a single Level I trauma center in Springfield, Massachusetts from 01/2010 through 12/2015 was performed. Basic demographics including age, Injury Severity Score (ISS), and length of stay were collected. Linear regression analysis was used to test the association between monthly admission rates and season, year, injury class, and mechanism of injury, and whether seasonal variation trends were different according to injury class or mechanism.
Results A total of 8886 admissions had a mean age of 44.6 and mean ISS of 11.9. Regression analysis showed significant seasonal variation in blunt compared with penetrating trauma (p<0.001), MCC (p<0.001), and falls (p=0.002). In addition, seasonal variation differed according to injury class or mechanism. There were significantly lower rates of MCCs in winter compared with all other seasons and conversely higher rates of total falls in winter compared with other seasons.
Discussion A significant seasonal variation in blunt trauma, MCC, and falls was observed. This has potential ramifications for resource allocation, including trauma prevention programs geared toward mechanisms of injury with significant seasonal variation.
Level of evidence Retrospective Review, Level IV.
- seasonal variation of trauma
- blunt trauma
- motorcycle crashes
- falls
- seasonal variation of mechanism of trauma
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- seasonal variation of trauma
- blunt trauma
- motorcycle crashes
- falls
- seasonal variation of mechanism of trauma
Introduction
Trauma is the leading cause of death in persons under the age of 46 and third leading cause of death in all ages.1 According to the CDC, in 2010 combined fatal and nonfatal unintentional injury resulted in total medical costs greater than $73 billion, with an estimated $419 billion when accounting for loss of work.2 Community-based prevention programs have been shown to prevent injury-related morbidity and mortality and reduce healthcare costs.3 The American Association for the Surgery of Trauma suggests a 10-step process for developing an injury prevention program. The first step consists of gathering and analyzing data, while the second step is to target an injury and the population affected.4 In order to do this effectively and efficiently, it would be ideal to target the most ‘at risk’ population near the most ‘at risk’ time.
Previous studies have demonstrated an association of increased overall trauma admissions with weather and temperature.5–7 Ho et al showed significant variation of penetrating trauma with changes in temperature.8 Bhattacharyya et al found individual weather changes such as maximum temperature and precipitation as independent predictors of trauma admissions.9
Studies have also reported that there is a high incidence of specific mechanisms of injury such as motor vehicle crashes (MVCs), falls, gunshot, stab, assault, and motorcycle crashes (MCCs).10 11 Similarly, these are the most common mechanisms at our institution. However, there are no studies that have evaluated seasonal variation with specific mechanisms of injury.
The purpose of this study was to determine whether there is any seasonal variation in trauma admissions and whether this variation differs for specific mechanisms of injury that are either common (ie, MVCs, MCCs, falls, or penetrating trauma) and/or have historical data suggesting seasonal or temperate variation (suicide and elderly falls).12 13 We hypothesized that penetrating trauma, MVCs, and MCCs occur more commonly during the summer, while more falls and suicides attempts occur during winter.
Methods
After obtaining institutional review board exemption, all trauma patients admitted to a Level I trauma center in Springfield, Massachusetts between January 1, 2010 and December 31, 2015 were retrospectively reviewed. Basic demographic variables were collected to provide context of the type of patients seen which include: date of injury, age, gender, Injury Severity Score (ISS), hospital length of stay, and mechanism of injury, and injury class (blunt or penetrating). Penetrating injuries were defined as injuries resulting from gunshot, stab wounds, impalements defined by Abbreviated Injury Scale, while blunt trauma were all other mechanisms of injuries excluding burns and penetrating trauma. Data were subdivided based on months of the year as well as seasons: Winter (December to February), Spring (March to May), Summer (June to August), and Fall (September to November).
Linear regression was used to analyze seasonal trends in mean monthly admissions across all patients by season, year and injury class (blunt or penetrating), or season, year, and mechanism of injury for selected mechanisms: motor vehicle collisions, motorcycle collisions, suicide attempts, falls, and falls in age greater than 65 years old. To examine interactions between seasonal trends and mechanism of injury, predicted mean monthly admission rates by season within each mechanism were computed based on the linear regression. Pairwise comparisons were used to identify seasons with excessive rates over the reference group (in the absence of any a priori hypothesis for comparisons, we chose the season with the lowest rate as the reference group). The p value used for significance was set at 0.005 to adjust for multiple comparisons. Finally, a subset of poly-traumatic and more severely injured admissions (ISS>15) was separately analyzed.
Results
During the enrollment period, 8886 patients with trauma were admitted to our Level I trauma center. Of these patients, 5923 (66.7%) were male and 2963 (33.3%) were female. The mean age was 44.6 and the mean ISS was 11. Penetrating trauma accounted for 9.7% of trauma admissions, while 90.3% sustained injuries due to blunt trauma. MVCs were the most common mechanism, accounting for 17.4% of all traumas, followed by falls. These two mechanisms in addition to motorcycle collisions, suicide attempts, and falls in age greater than 65 years old accounted for 50% of all trauma (4444 of 8886 cases) (see table 1).
Trauma demographics
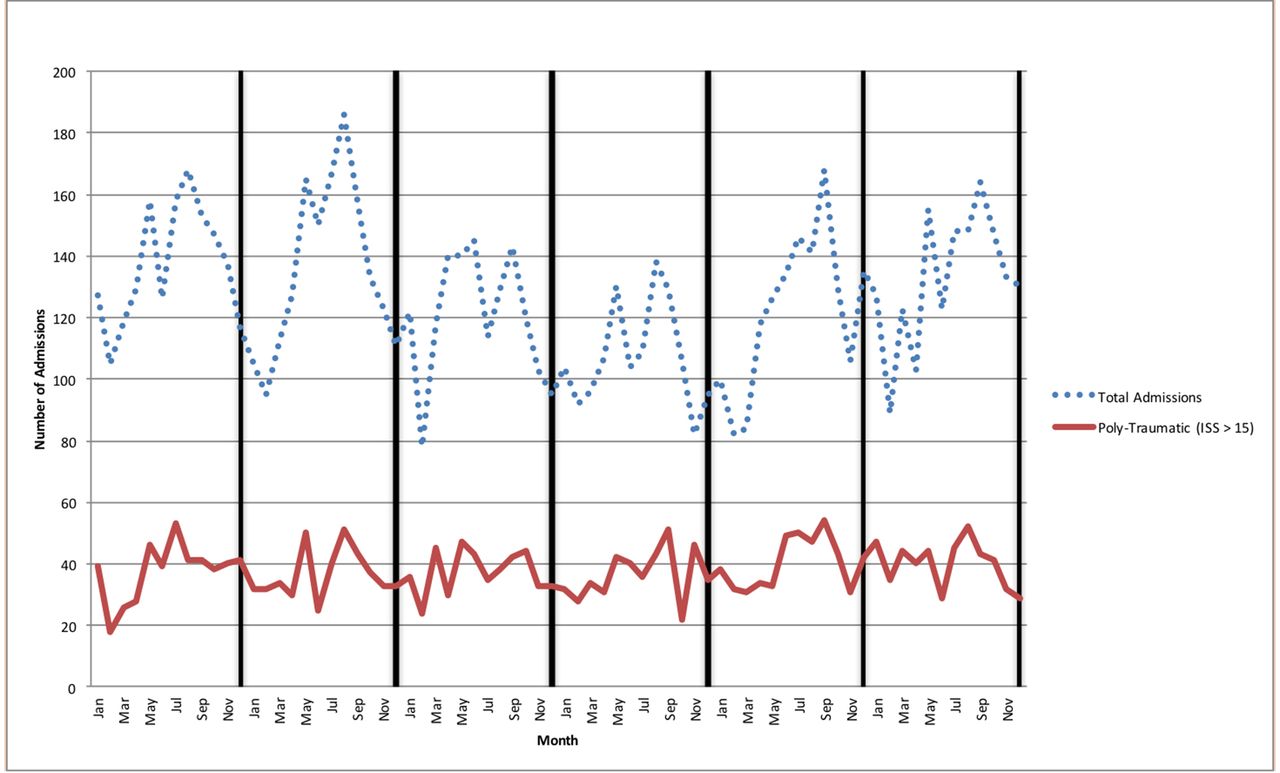
Figure 1 shows crude monthly admissions for the entire study period separately for blunt and penetrating admissions. Lowest rates occurred during the winter months in all years for both types of admission.
A linear regression analysis on number of admissions per month, with season, injury class, and year included as covariates was performed (table 2). These accounted for 94% of the variance in admissions by month (adjusted R2=0.94). The reference group for each covariate in the model represents the group with the lowest admission rates (eg, spring for season). Coefficients represent the difference in admission rates between all other groups and the reference group, after adjusting for other covariates in the model. Table 3 shows mean monthly admissions predicted from the regression. There were significant trends in admissions by season—winter had the lowest admission rates (after controlling by year) and summer the highest. When considering monthly admissions by year, 2010 had the highest rate and 2013 the lowest, but there was no linear trend in admissions by year. There was also no significant interaction between season and year, meaning that trends by season were constant across years.
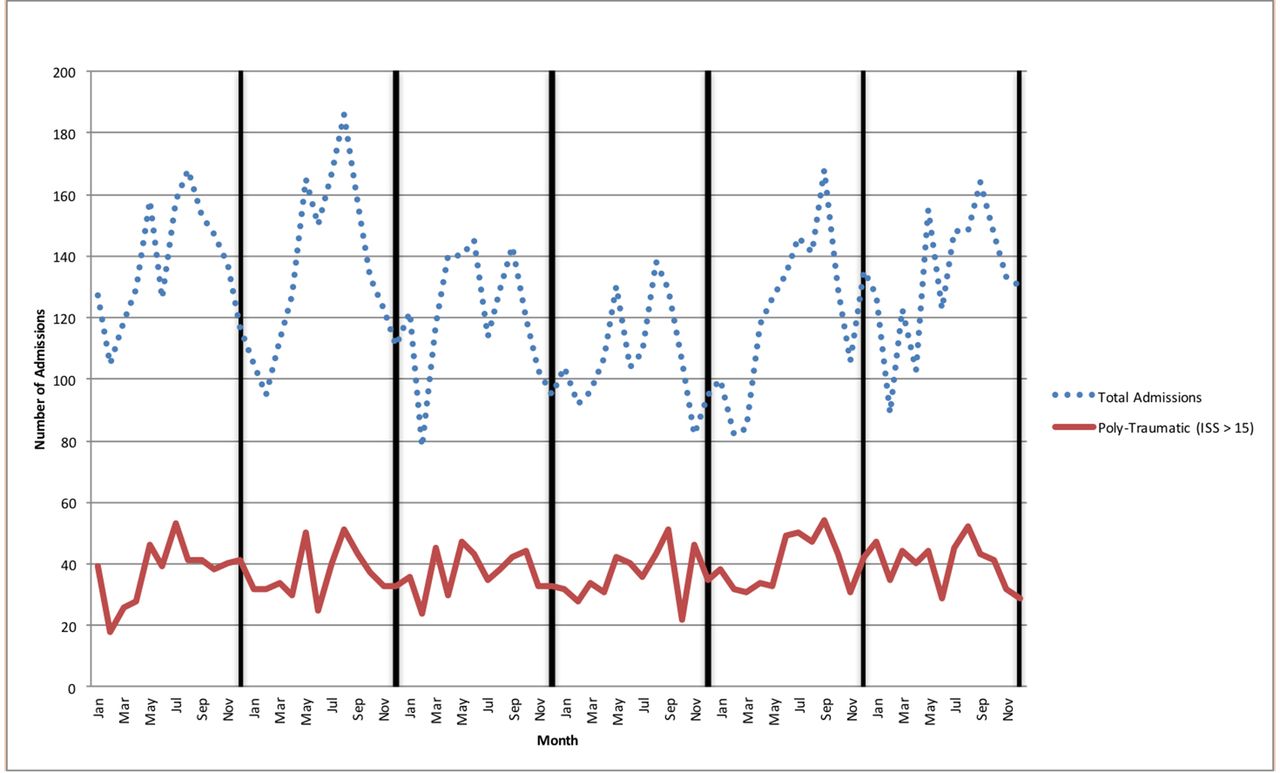
Trauma admissions by month and year. ISS, Injury Severity Score.
Regression on monthly admissions by season, injury class, and year
Predicted mean monthly admissions
With respect to injury class, there were significantly higher monthly admission rates for blunt admissions across all seasons, after adjusting for year. There was a significant interaction of season and blunt injuries, with the greatest excess of blunt admissions in summer (p<0.001) and fall (p=0.001) compared with winter.
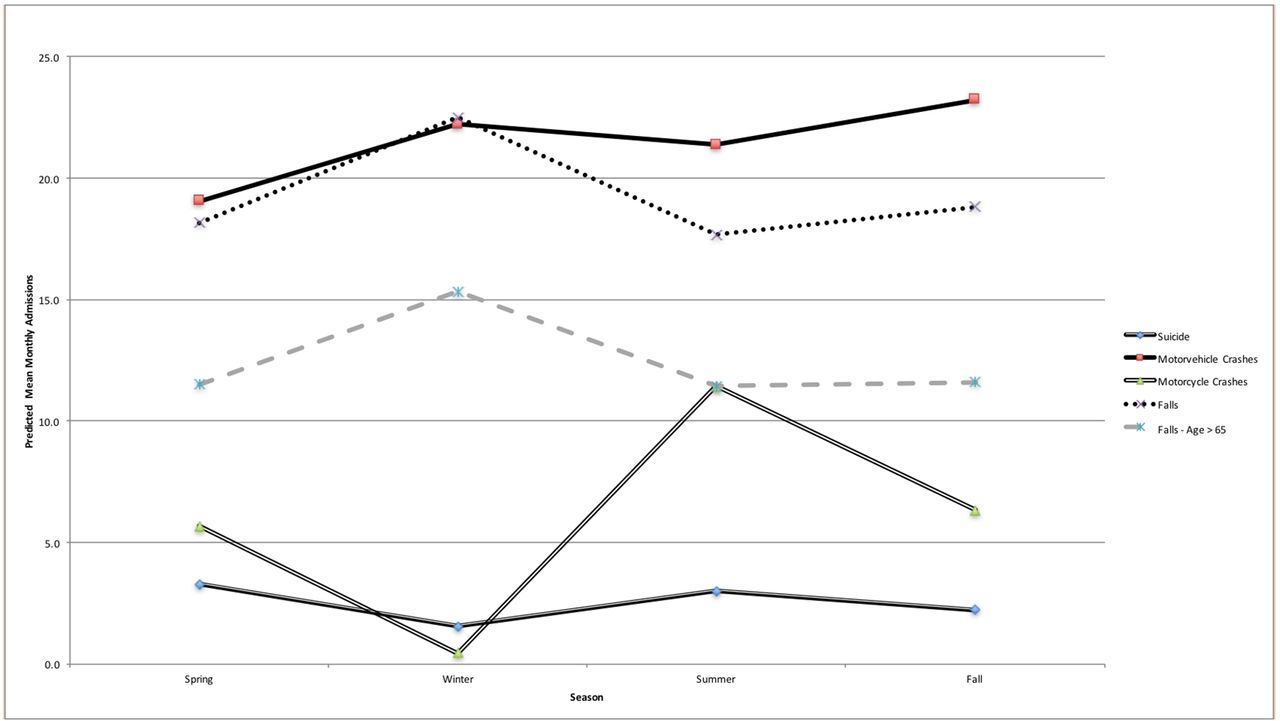
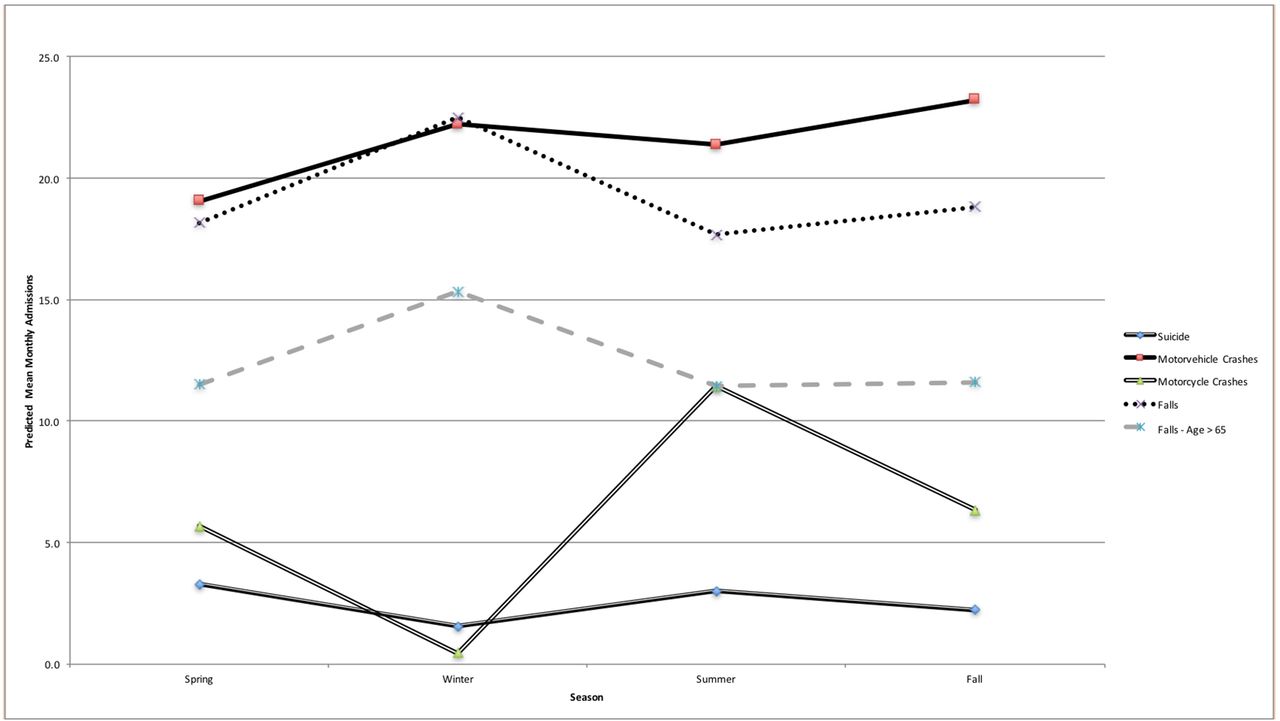
A separate linear regression was performed on the subset of patients with the five major mechanisms (n=4444). Predicted mean monthly admission rates by season and mechanism, adjusting for year, are shown in table 4 and figure 2. Suicides had the lowest predicted mean monthly admission rates in all seasons and MVCs the highest. The p values in the table represent the significance of pairwise comparisons within mechanism for each season compared with the season with the lowest admission rate (reference group). There was significant seasonal variation for falls and MCCs. For MCCs there were significantly higher rates for all seasons compared with winter, with an excess of predicted monthly admissions in spring of 5.2 and fall of 5.9, but the biggest excess occurred in summer (11.0). There were also significantly more falls in winter compared with summer (an excess of 4.8 per month). When analyzing separately for patients with ISS greater than 15, the effect of season or year was no different than for all patients.
{kind=link}
{kind=link}
Predicted mean monthly admissions by season and mechanism.
Predicted mean monthly admissions
Discussion
Traumatic injury is often thought to be predominantly unintentional and intentional thereby not occurring in any predictable pattern. However, previous studies have demonstrated an association between the number of trauma admissions and temperature, precipitation, hours of sunshine, day of the week, and time of day.7–9 14 The ability to predict the volume of total trauma admissions could enable better allocation of nondurable resources and personnel. However, in order to adjust staffing models a significant amount of lead-time may be required. According to the American Meteorological Society, ‘The current skill in forecasting daily weather conditions beyond 8 days is relatively low’.15 Furthermore, multiple factors including time of day, day of the week, temperature, rain or sunshine are at play, attempting to develop an equation to unify these into a clinically relevant resource needs assessment would be extremely difficult.
The intent of this study was to first determine if seasonal variation of specific trauma mechanisms exist in Western Massachusetts. In our location, an urban city with a population over 150 000, the winter temperature has a temperature range of 15°F–34°F (−9°C to 1°C), compared with the range of 33°F–56°F (0.5°C–13°C) and 55°F–78°F (13°C–26°C) in spring and summer.16 17 Our study found an increase in blunt trauma during summer and fall. While there are many postulated factors such as a sudden rise in temperature fostering more outdoor activity, there is likely a complex milieu of factors including social, economic, and weather factors that encompass a season and account for this variation. Although determining exact weather and temperature factors may be interesting, it may be too unpredictable to develop a targeted trauma prevention program. Instead, focusing on prevention leading up to and during seasons of increase incidence may lead to a reduction in traumatic injury mechanisms. Of course understanding patient demographics, socioeconomic factors, and environmental factors (eg, a particular road with increased rate of MVCs) is crucial to create any successful trauma prevention program.
Contrary to our hypothesis, there were higher rates of MVCs in fall and winter than in the spring. While most would predict that during summer months, the weather would allow more outdoor activity and increase motor vehicles on the road, which would lead to increase MVCs. Our data trended toward significance demonstrating a higher rate of MVCs in fall and winter. Although we did not evaluate specific weather trends in Western Massachusetts, it is known to have harsh weather conditions including heavy precipitation and snowfall in fall and winter months. Eisenberg et al demonstrated significant links between snowfall and fatal crashes.18 Similarly Saha et al described a high rate of adverse weather-related fatalities during months with high rain and wet conditions.19 Although there are multiple risk factors for MVCs including alcohol and drug use, road conditions, not using a seat belt, and so on, finding a higher rate of MVCs during specific seasons may be useful when devising a trauma prevention program regarding MVCs.
Nearly half of the MCCs occurred during summer. While most New Englanders would have predicted very few MCC during winter weather months due to the cold temperatures and the associated snow and ice, these data reinforce the need for a focused MCC prevention program leading up to and during spring and summer.
Falls were significantly more frequent during winter and close to significance in those greater than 65 years of age during winter in this study. A WHO report on falls prevention had a similar finding and cited potential reasons for this as slower reaction time triggered by hypothermia and/or slippery conditions related to ice.20 Given that falls during winter comprised nearly 30% of all trauma admissions, it would seem important to target prevention resources during this time.
While there are several limitations to this study (including its retrospective nature), one notable limitation is that this study was conducted at a single center located in a region with a highly variable climate. Although evaluating specific climates during seasons is beyond the scope of this project, Western Massachusetts is noted to be reliably cold with snow and ice in winter months and conversely hot and more humid in summer months. Studies in different climates would be required before any assertion of generalizability could be made. However, we believe the concept of identifying mechanisms of injury with seasonal variation may be important for all trauma centers. Potential benefits include a better understanding of institutional epidemiology and the ability to allocate preventative and treatment resources. Based on our institutions’ findings, future trauma prevention programs geared toward the prevention of blunt trauma, falls, and MCCs will be adapted to seasonal variation. For example, targeting MCCs in the spring and peaking in the summer with the hope of demonstrating a significant reduction of these injuries. Future directions include educating the public regarding these seasonal trends and focusing hospital resources to improve outcomes related to these traumatic injuries.
Conclusion
At a single Level I trauma center in Western Massachusetts, we found a significant seasonal variability in blunt trauma, MCCs, and falls. These findings are likely related to multiple factors including weather and socioeconomic factors. Future studies on seasonal trauma prevention programs geared toward mechanisms of trauma with significant seasonal variation appears warranted.
Acknowledgments
The authors would like to thank Ann Marie Mongeon for her assistance in data collection.
References
Footnotes
Contributors JN initiated the project, collected and analyzed data, drafted and revised the paper. He is the guarantor. SP assisted in data collection, drafted and revised the paper. AD helped develop the project and revised the paper. JG analyzed the data and helped write the statistical analysis section. RIG helped develop the project and revised the paper.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.