Article Text

Abstract
Perioperative morbidity and mortality related to anesthesia involves multiple factors. Patient characteristics and comorbidities play a role in many of these events, highlighting the importance of preoperative screening. While optimization of patient comorbidities is not always possible, having data regarding those comorbidities can prove life-saving. Equipment and medication considerations also enter into untoward outcomes such as anesthetic interventions outside of the traditional operating room where resources are sometimes lacking and haste creates errors. Ultimately, when surgeons and anesthesiologists cooperate in patient care, communicating concisely but thoroughly, patients are more likely to do well. The language of surgeons is that of diagnosis requiring a surgical intervention, while anesthesiologists are discussing patient comorbidities impacted by anesthetic medications, positive pressure ventilation, neuraxial techniques, ramifications of patient positioning, effects of opiates and so on. Because all of the considerations combine in determining outcomes, it is incumbent on both surgeons and anesthesiologists to understand those elements leading to severe morbid events as well as death. This review touches on many of the most important factors.
- anesthesia
- complications
- difficult airway
- obesity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Major issues surrounding perioperative morbidity and mortality in anesthesiology
Since the first use of ether, the risks and benefits of anesthesia have been analyzed repeatedly. Anesthesia evolved from nearly anyone being able to ‘drop ether’ to the subspecialty practice we undertake today, with non-anesthesiologists increasingly looking through a glass, darkly. Anesthetic equipment, medications, monitors and techniques change to keep pace with advances in surgery, aging patients, patients who are sicker and non-operating room (non-OR) procedures. Surgeons and anesthesiologists sometimes speak in entirely different terms when discussing cases. Part of that disconnect is that surgeons deal with a diagnosis requiring a surgical intervention, while anesthesiologists deliver anesthesia to facilitate a surgery while simultaneously keeping at-risk patient organs viable. In the 1940s, one in a thousand healthy subjects died from their anesthetic.1 The safety of anesthesia has evolved substantially with improved understanding of anesthetic-related deaths, the advent of better monitoring practices, improved airway management tools, sharing of safety knowledge and peer review. Today, anesthesia-related mortality is about 1.1 per million persons per year in the USA.2 Here we will elucidate both common and rare causes of anesthesia-related morbidity and mortality that significantly impact perioperative liability, especially in the setting of multiple comorbidities. Our goal in undertaking this review is that by elucidating underlying causes of complications related to anesthesia as well as their prevention, patients can have safer surgical experiences.
Closed Claims Database
Systematic study of anesthesia-related morbidity and mortality in the USA has always been hampered by lack of a unified database. In 1984, Drs Richard Solazzi and Richard Ward, anesthesiologists at the University of Washington, studied resolved lawsuits from the State of Washington. They examined cases of ‘bad’ outcomes hoping to decipher the causes and improve future outcomes. That project led to the creation of the Closed Claims Database in 1985. Collaboration with several major professional liability insurance companies like the St. Paul Fire and Marine Insurance Company of St. Paul, Minnesota, the project sought to codify the elements of specific ‘bad’ outcomes beyond the borders of Washington State. The initial data collection focused on cases that seemed unusual, such as death due to spinal anesthesia. That analysis changed the way bradycardia and hypotension after spinal were viewed and treated by anesthesiologists. Since then, over 9799 claims have been analyzed covering a variety of subjects in more than 60 newsletter articles and 33 peer-reviewed publications.3
Human error as a factor
In 1978, Cooper et al published their study highlighting human errors as more common than pure equipment failure in preventable incidents, which was the first time such errors were reported systematically in the anesthesia literature.3 They found that 82% of incidents were inadvertent mistakes such as ‘syringe swaps’, accidental changes in fresh gas flow or unfamiliarity with clinical situations or equipment. While inadequate communication, distraction and haste were also described, emphasis was placed on medication errors in the operating room (OR). Since that initial study, numerous others examined the mechanics of medication delivery such as use of color-coded syringe labels4 and bar coding of pharmaceuticals, patients and labels.5 Meanwhile both nursing and pharmacy studies looked at using two practitioners to read labels and orders, amid other systems measures.6 7 Only anesthesiologists and nurse anesthetists prescribe, dispense and administer medications without a second person verifying the process. In 1981, Anaesthesia published a retrospective analysis titled ‘A survey of anesthetic misadventures’ in which more than 8000 incident reports in a busy district hospital were analyzed, finding that most incidents arose out of failure to perform a normal check, both with medications and equipment.8 In that analysis, the rate of major and minor mishaps was 0.14% or 1 mishap in 694 observations. Another retrospective analysis published in 1990 covered more than 1 13 000 accident reports during a 10-year period.9 Again, failure to check, inattention, lack of vigilance and carelessness were identified as factors. Most of the anesthetics during that retrospective review (1978–1987) were non-cardiac (97 496), with 148 reported problematic outcomes. Although the most common problem was dental damage (26%), 19% of the reports concerned cardiac arrest, of which 16 were fatal. Drug errors in the Closed Claims Audit show that roughly 24% result in fatality. While newer anesthetic medications are safer than before, drug errors in anesthesia occur relatively frequently. Most medication errors are ultimately benign; however, a subset results in significant harm or escalation in care.10 11 Consequently, vigilance plays a role in preventing anesthetic mishaps in all cases.
Loss of airway/difficult intubation
The inability to intubate or mask ventilat is one of the most feared complications in anesthesiology. Early anesthetics involved spontaneously breathing patients inhaling anesthetic vapor. Because patients would occasionally completely obstruct or aspirate gastric contents and die, the utilization of endotracheal tubes began in earnest with the published work of Meltzer, Auer and Elsberg in 1909.12 It was not until 1913, however, that Janeway published his work using the laryngoscope to assist intubating the trachea.13 Since that time, a plethora of tools invented to aid intubation has improved the ability to intubate. Until now, no device carries a 100% guarantee of success.
In addition to airway management tools, anesthesiologists studied human airway characteristics in an attempt to judge the ease or difficulty in performing intubation or mask ventilation. One such study by Mallampati, published in 1985 reported that visualization of the entire uvula and faucial pillars correlated with the greatest ease of intubation, whereas the inability to see the soft palate created a very unfavorable condition for intubation.14 Although there is some statistical relationship to intubation success in the four modified Mallampati views, none is perfectly specific for estimating intubation success. Beyond Mallampati’s initial efforts, numerous studies followed, attempting to develop an airway assessment method or combination of methods that yield perfect specificity and sensitivity. However, no airway assessment tool or combination of tools is absolutely sensitive or specific.
Respiratory events account for 17% of Closed Claims outcomes with brain damage and death being the most serious. Twenty-seven per cent of those respiratory events are due to difficult intubation. Difficult intubation is far more likely to occur in suboptimal environments outside of the OR such as in the emergency department, the intensive care unit (ICU), patient wards and even outside of the hospital. Consequently, anesthesiologists must prepare for difficult intubation more often when outside of the OR. Inside the OR arena, 67% of difficult intubations are noted at induction of general anesthesia and may occur in individuals who were originally assessed as having a ‘normal airway’. Up to 15% occur during surgery if the patient becomes extubated unexpectedly or an exchange of endotracheal tube becomes necessary. Another 12% of cases occurred at planned extubation when events such as laryngospasm, bronchospasm or insufficient respiratory drive mandated reintubation of the patient. Death and brain damage associated with airway incidents during induction of general anesthesia have decreased since 1985, yet adverse events related to other phases of anesthesia (maintenance, emergence) have not changed.
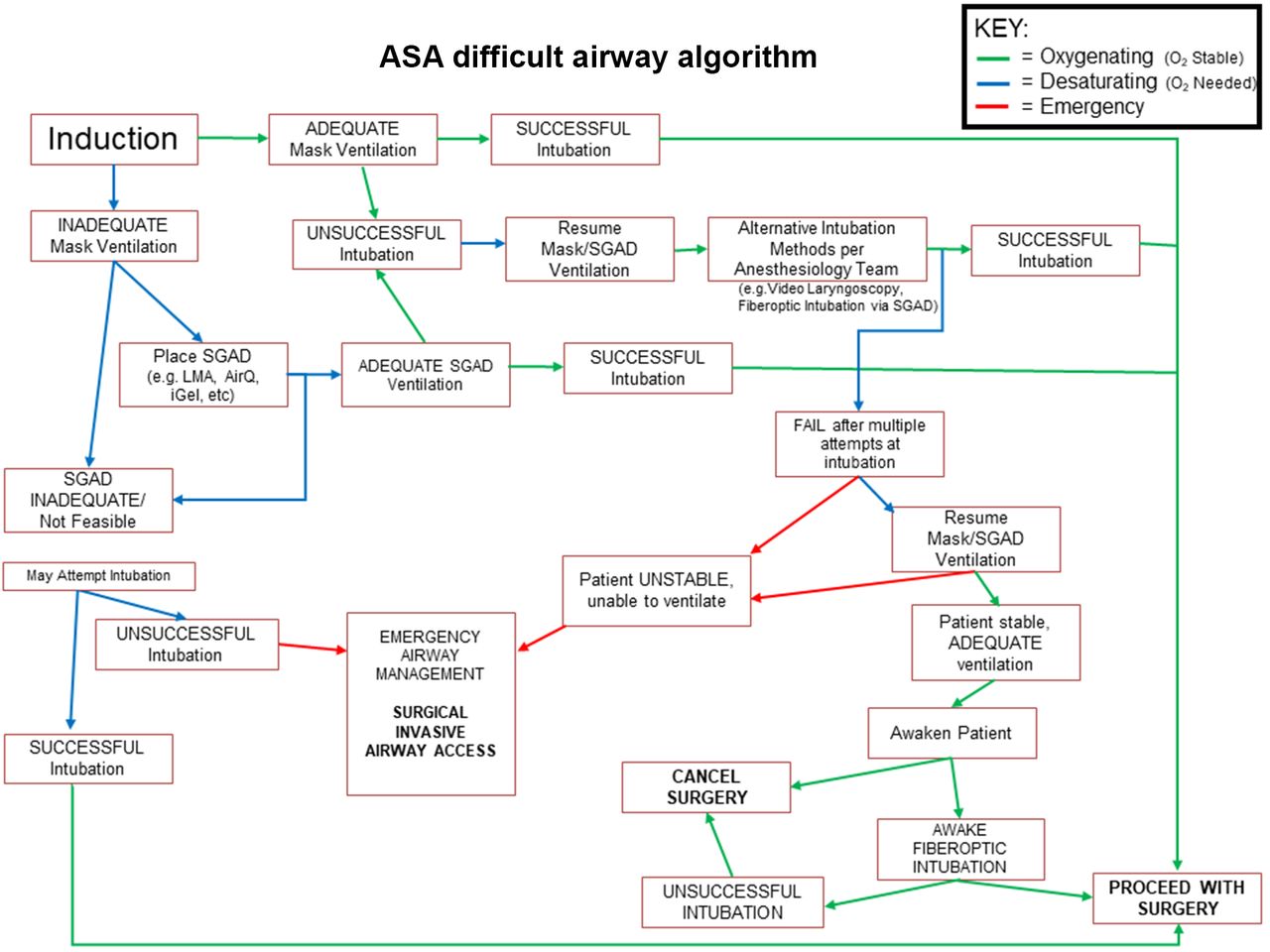
Of note, continued, persistent attempts at standard direct laryngoscopy more commonly result in airway loss with brain damage or even death. No more than three attempts at standard direct laryngoscopy should be used before other modalities should be undertaken. Consequently, the difficult airway algorithm15 should be implemented (refer to figure 1), allowing patients to resume spontaneous respirations and wake up when possible or advancing to other airway rescue devices if spontaneous respiration is not possible. Supraglottic airway devices such as the laryngeal mask airway marked an advance in rescuing difficult airways; however, they are not 100% effective. Likewise, video laryngoscopy (indirect laryngoscopy) has improved safety, but even in the largest studies, it has not revealed perfect efficacy. Other tools such as bougies, light wands, Combitubes, blind techniques and surgical airway also comprise part of the difficult airway algorithm.

Difficult airway algorithm. ASA, American Society of Anesthesiology; LMA, laryngeal mask airway; SGAD, supraglottic airway device.
Performing fiberoptic techniques can be difficult after failed intubation due to blood and secretions in the airway, obscuring important structures. Awake fiberoptic intubation as a primary modality is more frequently used in the anticipated difficult airway rather than after other methods have failed in a patient who has already been induced. Surgical airway should be considered early in the event of a ‘can’t ventilate can’t intubate’ scenario and requires ongoing communication between anesthesiologists and surgeons. However, if a patient can be ventilated, then preparing for a more ordered approach to the airway, including having appropriate surgeon involvement ready, may be undertaken. Of particular note, there are instances when intubation poses a significant mortality risk such as a nearly occlusive supraglottic mass. Consequently, a planned awake tracheostomy should be undertaken by the surgical and anesthesia teams to ensure the best possible outcome for the patient.
From a pharmacological standpoint, the introduction of sugammadex for reversal of neuromuscular blockade may become an adjunct to the difficult airway algorithm. Sugammadex actively binds rocuronium or vecuronium, eliminating the paralysis induced by those agents. Although it has been used in the clinical event of inability to intubate, its usefulness for ‘can’t intubate can’t ventilate’ has been called into question due to the time it takes to draw up, administer, circulate and have an effect. Considering that after 5 min of apnea the brain begins to deteriorate, the scenario of several intubation attempts followed by obtaining sugammadex, delivery and subsequent effect may not be able to salvage a patient.
Obstructive sleep apnea
Obstructive sleep apnea (OSA) is a modern diagnosis. In the study of Pickwickian persons, common threads arose leading to a formal syndrome. First appearing in the 1980s medical literature, it was often referred to as obesity hypoventilation syndrome.16 A New England Journal of Medicine report on sleep disordered breathing in middle-aged adults published in 1993 stirred the interest of a variety of physicians, including anesthesiologists.17 For anesthesiologists, the association of OSA with difficult airways was succinctly described in 1995 by Biro et al.18 Numerous studies followed regarding preoperative diagnosis using standardized questionnaires,19 the relative safety of allowing patients with OSA to undergo ambulatory surgery,20 predictive value of OSA in difficult intubation21 and what types of postoperative monitoring are most valuable.22
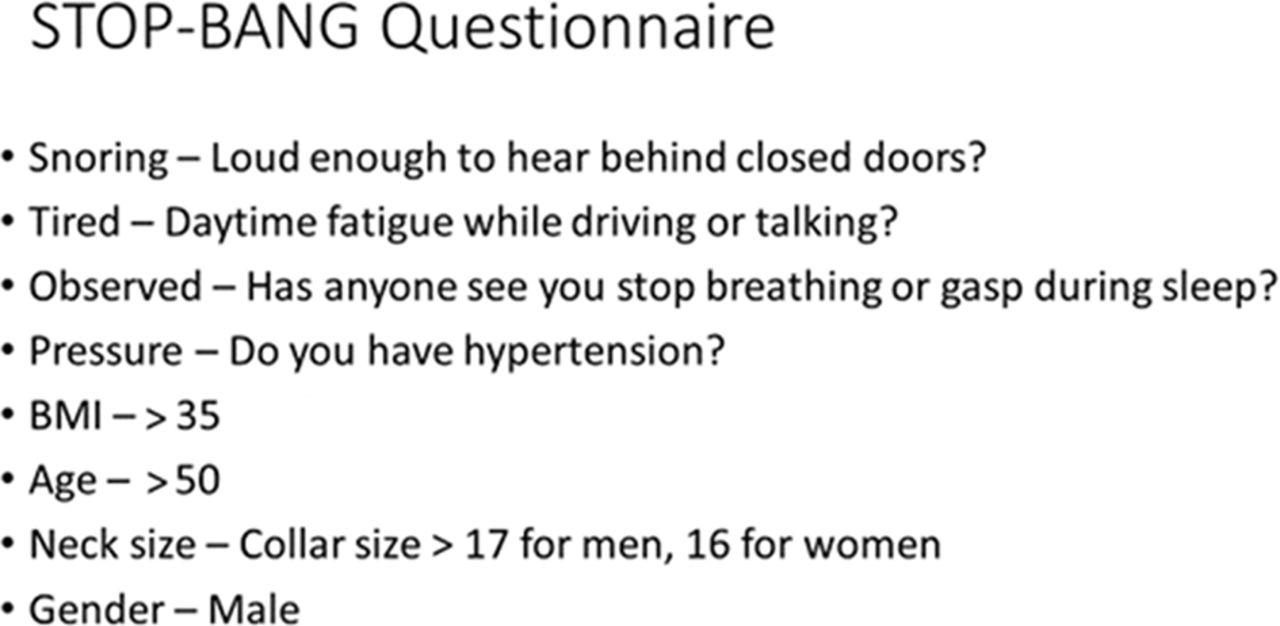
OSA is described as the partial or complete obstruction of the upper airway with resulting arterial oxygen desaturation, increased carbon dioxide (CO2) accumulation and importantly, excess sympathetic stimulation. Patients experience brief, repetitive cortical arousals that disrupt normal sleep with resultant excessive daytime sleepiness. Cohabiters of those with sleep apnea typically report habitual snoring in the patient with OSA as well as episodes of self-limited apnea. Therefore, additional questioning of significant others, roommates or family may be helpful (refer to figure 2).
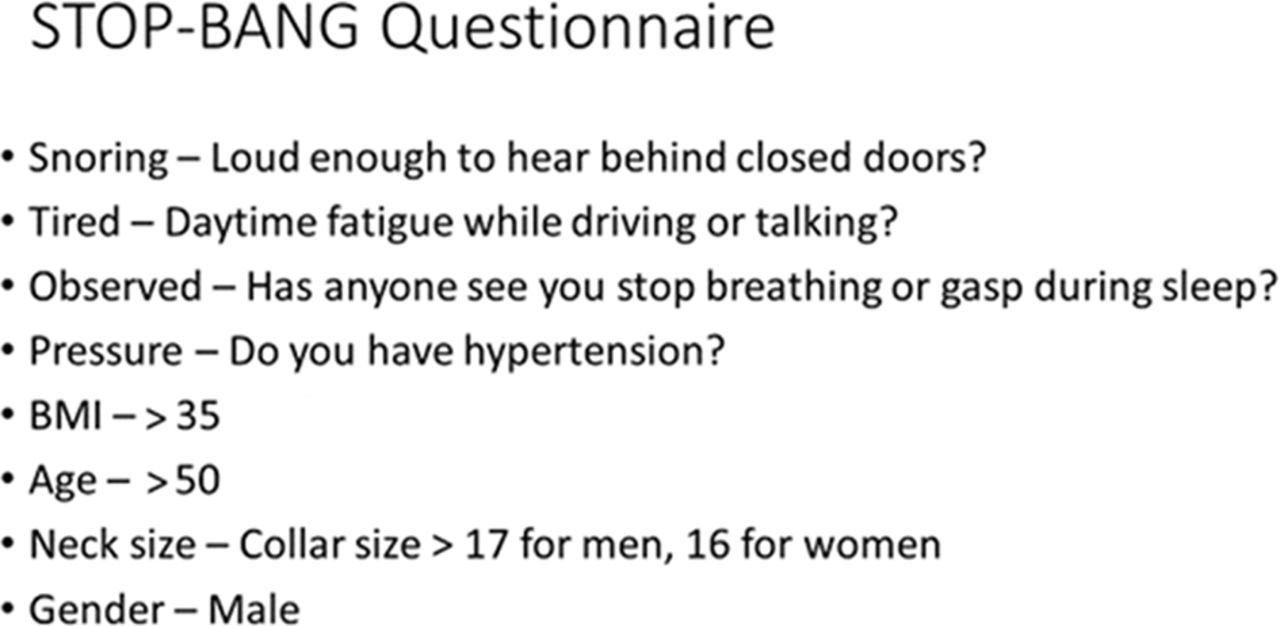
STOP-BANG Questionnaire. BMI, body mass index.56
Excess sympathetic stimulation due to OSA contributes to global, significant adverse health outcomes in patients with OSA. Disease states associated with OSA are hypertension, metabolic syndrome, diabetes, pulmonary hypertension (PHTN), ischemic heart disease, congestive heart failure (CHF), arrhythmias, depression and an increased risk of accidental trauma.23 When one considers the comorbidities most associated with anesthesia-related deaths, OSA carries significant risks for patients undergoing surgery. The number and severity of comorbidities add to the statistical odds of a patient suffering a morbid or lethal anesthetic event.24 25 Consequently, OSA is associated with difficult intubation and other morbid and lethal events in the perioperative period. OSA affects more men than women. Approximately 9% of women and 26% of men in the 30-year-old to 49-year-old age range, and 27% of women and 46% of men in the 50-year-old to 70-year-old age range have OSA. Roughly 90% of patients with moderate-to-severe OSA lack a formal diagnosis. OSA worsens in the postoperative period, particularly with respect to opiates.23 26 Prevention of adverse respiratory events in patients at risk of OSA includes using positive airway pressure therapy (BiLevel Positive Airway Pressure/Continuous Positive Airway Pressure (BiPAP/CPAP)) which can be prescribed by the physician and implemented by respiratory therapy, even in patients without a formal diagnosis. Patients already diagnosed with OSA should be encouraged to bring their own mask for use with hospital-owned BiPAP/CPAP machines when hospital rules inhibit the use of outside devices. Other methods to prevent opiate-induced respiratory depression include using regional and peripheral local anesthetic-based techniques to reduce opiate use, as well as using (when possible) non-steroidal antiinflammatory drugs (NSAIDs), non-opiate adjuncts (such as clonidine and ketamine) and physical adjuncts like ice or heat. Setting reasonable patient expectations preoperatively and discussing the importance of safety vis a vis comfort are especially important in high-risk patients.
Opiate-induced respiratory depression
Opiate-induced respiratory depression occurs in patients with OSA, the elderly, premature infants of less than 60 weeks postconceptual age, significant renal disease, cardiac disease or pulmonary disease (eg, chronic obstructive pulmonary disease (COPD)). Furthermore, different opiates pose different risks, such as the accumulation of metabolites that are active, but also have very long clearance half-lives such as morphine/morphine-6 glucuronide27 or hydromorphone which has a delayed onset time, allowing for overdosing when typical patient-controlled analgesia (PCA) settings are used. From the Closed Claims Project examining opiate-related respiratory depression, a number of factors emerged. Physician factors most frequently associated with opiate-induced respiratory depression in the perioperative period are continuous (basal rate) infusions (34%), multiple prescribers (33%), simultaneous prescription of non-opiate sedatives or sleep agents with opiates (34%), PCA only (18%), neuraxial opiates (17%) and multimodal analgesic management with more than one type of opiate available (47%).28 Additional patient risk factors associated with opiate-related respiratory depression are female gender (57%), obesity (66%), American Society of Anesthesiologists (ASA) physical status 1 and 2 (63%), age >50 years (44%), lower extremity surgery (41%), diagnosed OSA (16%), high likelihood of OSA (9%) and chronic opiate use (8%).28
Most opiate-related respiratory events are heralded by somnolence and in the Closed Claims Project were noted in the written record in 62% of cases. Ninety-seven per cent of the events resulting in death or permanent brain damage were thought to have been preventable with better monitoring/surveillance. In 31% of those cases, nursing assessment or response was deemed inadequate. Because of those findings, surveillance tools for detecting opiate-related somnolence include nursing scales such as the Richmond Agitation and Sedation Scale (RASS) and the Pasero Opioid-Induced Sedation Scale (POSS).29 Beyond mere surveillance however, the system must incorporate appropriate responses for somnolent patients. Somnolence should prompt physician notification and even presence at bedside, not simply orders for supplemental oxygen or delivery of rescue doses of naloxone, which can precipitate significant cardiopulmonary side effects. While pulse oximetry with plethysmography may help monitor respiratory rate, pulse oximetry alone fails to detect important accumulations of CO2 in patients experiencing respiratory depression from opiates. CO2 monitoring combined with true respiratory rate monitoring provides the best recognition of incipient respiratory depression from opiates.30 Nursing and support staff should understand that respiratory rates of 10 or below should prompt physician presence to the patient’s bedside.31
OR fires
Figure 3 though OR fires are not exceedingly common, they often result in devastating consequences for patients. The Closed Claims analysis of OR fires addressed 103 fires, 14% of which resulted in disability and 6% caused deaths. In 90% of cases, electrocautery was the ignition source while oxygen provided the oxidizer in 95%. Alcohol-based cleaning solutions provided fuel in 15% of events. Seventy-six per cent of claims were for monitored anesthesia care (MAC) or regional cases using supplemental oxygen. Nasal cannula involved more than half of those cases and 44% of cases involved the airway.32 Certain types of surgical procedures create particular types of fires. For instance, airway surgery is most often associated with endotracheal tube fires, whereas emergency surgery such as stat Cesarean section relates to insufficient drying time for alcohol-based solutions. Roughly 20% of MAC anesthesia burn injuries relate to oxygen accumulating under the drapes and igniting or the patient oxygen source was too close to the electrocautery unit.33 Other events reported in the literature include the ignition of agents such as benzoin.34 Lasers and laparoscopic equipment light sources also cause OR fires and burns.35

ANESTHESIA OR FIRE TRIAD. OR, operating room.
Procedures of the face involved the preponderance of OR fires leading to safety precautions advising against the use of supplemental oxygen for those types of surgeries.36 Central lines and pacemaker/automatic implantable cardioverter-defibrillator (AICD) insertions comprised 6% of OR fires examined by Mehta et al.32 Those patients present a conundrum in that they often are oxygen dependent or suffer significant oxygen desaturation under sedation. Recommendations include providing no more than 30% oxygen (FiO2), avoidance of drapes that might trap/collect oxygen and avoidance of heavy sedation so that patients maintain better spontaneous respiratory effort. Improved use of local anesthetic decreases the need for heavy sedation. Again, effective perioperative management of patient expectations, with emphasis on safety, is crucial.
Neck procedures, including tracheostomy, comprise 12% of the claims studied. Tracheostomy patients may have significant baseline dependence on higher fractions of inspired oxygen (FiO2) percentages. In those cases, surgeons and anesthesiologists must communicate when nearing the trachea. As entry into the tracheal space approaches, decreasing the FiO2% to 21% expired oxygen content (room air equivalent) reduces the risk of tracheal fire. Likewise, suspending active ventilation at the time of entry if cautery is used may limit ignition risk. It is important to remember that either type of electrocautery, unipolar or bipolar, poses an ignition risk.
In the event of OR fire, rapid and appropriate responses decrease the odds of death and may limit injury. Stopping supplemental oxygen and turning off all other gases, smothering/flooding the fire and removing burning elements are important measures. Practising OR fire scenarios (eg, Fire Drills) prepares staff to handle these emergencies. Posting protocols with bulleted points of procedures may also help staff to recall lifesaving information when most needed. Yearly competency materials as part of hospital-based education programs may also have a positive impact.
Nerve injury
The number of claims related to neuraxial anesthesia has been declining. Nonetheless, neuraxial anesthesia constitutes 74% of claims related to nerve injury and includes direct damage to the cord or nerve roots as well as local anesthetic-induced toxicity to those structures. Although these events are quite rare compared with the number of neuraxial anesthetics performed per year in the USA, they often encompass serious outcomes with significant disability. Patient risk factors most associated with neuraxial injury are elderly and woman. Death or brain damage related to neuraxial anesthesia is quite rare but each constitute 9% of claims from neuraxial techniques. In examining those cases where death or brain damage occurred, failure to rescue from cardiac arrest due to high spinal and oversedation were notable antecedents.37
Peripheral nerve blocks are rising in numbers of claims as the use of peripheral regional anesthesia/analgesia increases. The proposed incidence of injury based on large studies is roughly 1:300 blocks, typically represents paresis rather than permanent injury, occurs even in expert hands and most commonly involves interscalene nerve blocks currently.38 Whether that statistic simply reflects the fact that patients are more likely to notice upper extremity deficits relative to that of the lower extremity is unknown. Ultrasound guidance has not decreased the incidence of neural complications associated with peripheral nerve blocks nor has it improved block success, but reduces risk associated with complications surrounding structures such as inadvertent vessel puncture leading to local anesthetic toxicity39 40 or pneumothorax. The use of continuous peripheral nerve block catheters has also expanded, leading to associated complications. A higher incidence of persistent sensory and motor blockade may occur with continuous peripheral nerve block (CNPB) catheters than with single-shot blockade based on some studies; however, there are investigations suggesting that the incidence may be comparable with single-shot injections. Infection related to catheters has been a concern, particularly because catheters become easily colonized with skin organisms. Associated patient risk factors for such an infection include diabetes, catheters in place longer than 48 hours, trauma and ICU status.40
Postoperative visual loss
Vision loss in the perioperative period is devastating and typically permanent. Those procedures most often affiliated are spine surgery and cardiac bypass surgery. However, any surgery in the prone position or where the head is placed lower than the heart for a prolonged period can result in postoperative visual loss (POVL).41 Although spine surgery constitutes the majority of claims,42 other reported cases include prostate, total hip and pilonidal cyst surgeries. Hydrostatic forces play a role when the eyes are lower than the heart. Furthermore, in the prone position, intraocular pressure rises considerably; however, this effect can be decreased by placing the patient in reverse Trendelenburg position.43 Other factors that may play a role in POVL are male gender, younger age,44 diabetes with an associated ‘opathy’ such as neuropathy, retinopathy or nephropathy, renal disease with resultant anemia, large volumes of crystalloid, significant blood loss or hypotension and cases lasting longer than 6 hours. Nonetheless, patients with similar risk factors and similar perioperative management yet sustain no POVL complicate the study of the phenomenon. Anatomic variation that cannot be seen by anesthesiologists may influence which patients develop this rare complication. When it comes to discussing POVL, either the surgeon and/or the anesthesiologist may cover informed consent; however, a study by Corda et al suggests that patients would prefer that surgeons address the issue of POVL before the day of surgery.45 Management of prolonged procedures should include staged surgeries when possible, avoiding hypotension and anemia (hemoglobin <9.0), using central venous pressure monitoring in high-risk patients, keeping the head in neutral position above the level of the heart when possible and using colloids and vasopressors as needed.
Major adverse cardiovascular events
Major adverse cardiovascular events (MACE) constitute 15% of lawsuits against surgeons and anesthesiologists with 64% of those associated with death and 21% with brain damage. Relevant to those events were hemorrhage/blood replacement, stroke and inadequate resuscitation.46 Emergency surgery, total joint replacement, nighttime and weekend surgeries have higher perioperative morbidity and mortality as well.47 Even elective cases after 15:00 were found to have increased mortality in one study.48
Numerous investigations have compared general anesthesia with regional anesthesia and perioperative cardiac events and mortality. With the exception of pregnant women, who are approximately 17 times more likely to die from general anesthesia than neuraxial anesthesia, no clear relationship with mortality exists between the two types of anesthesia. However, analyses of peripheral regional anesthesia or neuraxial anesthesia for total joint replacement reveal decreases in deep vein thrombosis, infection, pneumonia, stroke and perioperative myocardial Infarction (MI) with those methods in comparison with general anesthesia.49
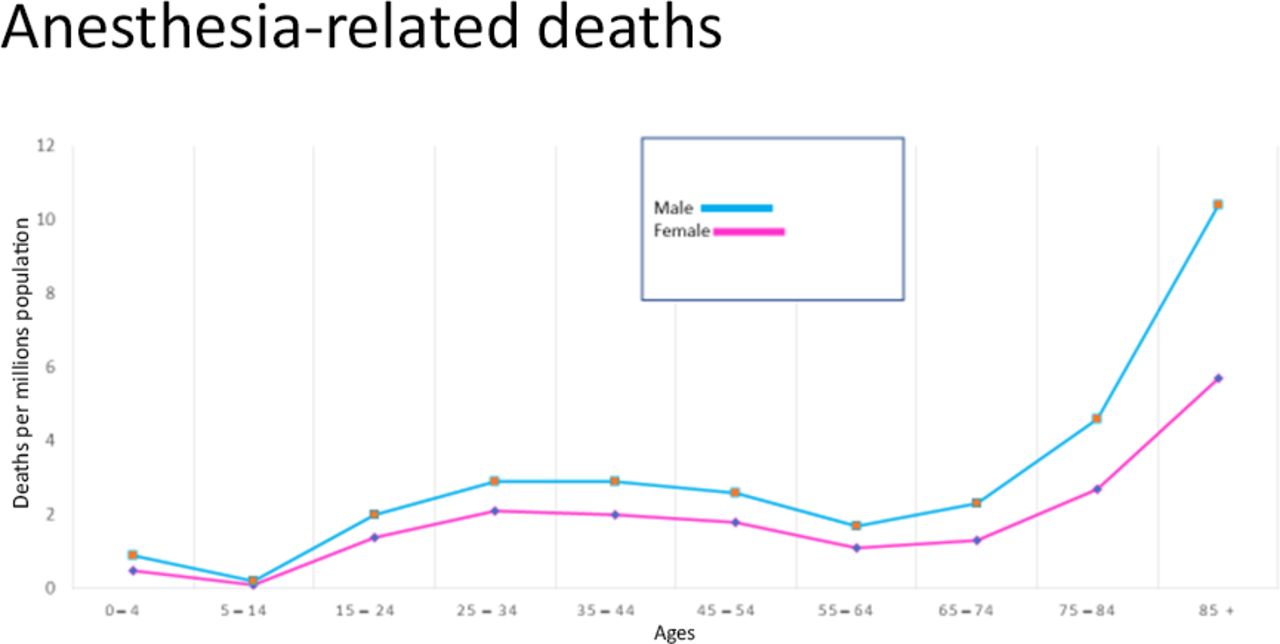
Patient-related risks for MACE in the perioperative period are pre-existing ischemic coronary disease, systolic and diastolic heart failure, male gender, diabetes, renal insufficiency and age greater than 65 years with an exponential increase in risk after age 85.50 Nonetheless, undergoing anesthesia is 97% safer now than it was prior to 1953 (refer to Figure 4).2
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anesthesia-related deaths by age and gender (adapted from Li et al2).
More recent reviews both in Europe and in the USA suggest that PHTN is a very important risk factor for perioperative cardiac death and contributes to death in cases associated with CHF. PHTN presents a particular hazard with total joint replacement.51–53 Some risk factors for PHTN include female gender (autoimmune related), COPD, OSA, history of significant or repetitive pulmonary emboli, CHF, cirrhosis and methamphetamine use. While right heart catheterization is the gold standard for diagnosing PHTN, echocardiography is becoming more reliable (TEE > TTE). Because cardiologists typically only consider left heart impairment as a risk factor for anesthetic morbidity and mortality, the specific question regarding right heart pressures and markers of PHTN must be actively sought!
Temperature management
Temperature management refers to the active avoidance of dramatic shifts in patient core body temperature during the intraoperative period. While hyperthermia (T>100.4°F) is to be avoided, it is unusual to occur in settings other than infection or iatrogenic causes (over warming). More likely is the occurrence of intraoperative hypothermia due to a combination of four types of heat loss: conductive, convective, evaporative and radiant. General anesthesia alters the body’s normal thermoregulatory mechanisms, as vasodilatory heat loss occurs when core body heat is lost after redistribution to the peripheral circulation while simultaneously impairing the compensatory shivering and vasoconstriction mechanisms. Adverse consequences of hypothermia include delayed emergence from anesthesia, shivering/increased oxygen consumption, prolongation of effect of many medications (including paralytics), reduced coagulation/increased transfusion requirements and reduction of surgical site healing and/or increased rates risks of wound infection. Strategies to avoid heat loss start with the pre-emptive efforts to keep the OR (and thereby all of its contents) at greater than 70°F so as to prevent conductive and radiant losses. Additional methods of control include intraoperative administration of fluids through a fluid warmer and perioperative use of artificial heating/cooling devices of varying types (thermal reflective, forced air, underbody warming/cooling water mats, etc).
Beta-blocker therapy
The recommendations regarding perioperative use of beta-blockers are simple and straightforward. If the patient is currently taking a beta-blocker (chronic therapy), they should continue taking their beta-blockers. However, despite the cardioprotective effects of beta-blockade, initiation of beta-blocker therapy in the immediate preoperative period has been associated with significant postoperative morbidity/mortality. More specifically, Wijeysundera and colleagues showed that perioperative beta-blockade started within 1 day or less before non-cardiac surgery prevents non-fatal MI but increases risks of stroke, death, hypotension and bradycardia.54 Additionally, Beattie et al demonstrated in 2010 that in the setting of anemia, beta-blockade significantly increases the risk of major adverse cardiac effects and mortality thereby emphasizing the importance of giving consideration to increasing the threshold of (intraoperative) blood transfusion in patient on beta-blocker therapy.55
Anticoagulant therapy
Perioperative anticoagulant therapy has changed dramatically in recent years and the number of therapeutic agents has increased substantially. When determining the appropriate course of action and timing of surgical intervention for a patient on anticoagulant therapy (regardless of the agent), consultation with the prescribing provider (cardiologist/internist) is essential to progress. Of note, if central neuraxial anesthesia (epidural/spinal) does not supersede the primary provider/cardiologist’s input regarding the importance of continuity of the patient’s anticoagulation therapy.
Enhanced recovery after surgery
While enhanced recovery after surgery protocols are gaining acceptance nationwide and have been emphasized in recent years, the concept is still largely in its nascency. While the value of these protocols is coming to light, specific non-adherence or failure to implement such protocols has (as yet) not been proven to be directly associated with life-threatening adverse events after surgery.
Summary
Even as delivering anesthesia becomes safer due to improved medications, equipment and monitoring, the continued study of perioperative morbidity and mortality discloses risk factors for poor outcomes. Some hazards are more readily rectified such as removing oxygen from the operative field in high-risk surgeries, improving medication delivery systems that prevent wrong drug or dose errors or avoiding opiates in high-risk patients. Other perils are less easily emended, such as needing to perform emergency surgery on patients with multiple comorbidities. Ultimately, accurate and comprehensive communication between anesthesiologists and surgeons throughout the perioperative period will help prevent complications and improve patient outcomes.
References
Footnotes
Contributors BC, CS and LC all contributed by way of additional information and editing of the manuscript written by JS.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement None of the data contained in the article is original as this is a review article compiling pertinent information from previously published sources.