Article Text

Abstract
Background Fixation of diaphyseal tibial fractures by plates is not considered the best option due to complications that may eventually arise; however, if principles of stability and proper surgical techniques are used, it is possible to obtain fracture consolidation without major risks.
Methods We conducted a cross-sectional observational descriptive study by retrospectively analyzing medical records of patients with diaphyseal tibial fractures that were treated with plates from the period between June 2011 and June 2014 at San José and Susana López Hospitals in the city of Popayan, Colombia. 3 treatment groups were created and analyzed according to the type of fracture (Association Osteosynthesis/Osteosynthesis Trauma Association AO/OTA): group I: simple fractures 42A/B, absolute stability; group II: simple fractures 42A/B, Minimally Invasive Plate Osteosynthesis (MIPO) technique, relative stability; group III: multifragmentary fractures 42C, MIPO technique, relative stability. A descriptive analysis of patients, fracture consolidation time, and complications in each group were performed.
Results 45 patients with tibial fractures treated with osteosynthesis plates were analyzed. Group I: 14 patients, 42A (n=13) and 42B (n=1), had an average consolidation time of 16.38 (SD=1.98) and 14 weeks, respectively. In group II: 19 patients, out of which 18 achieved fracture consolidation (42A n=15 and 42B n=3) with an average time of 17.4 (SD=3.33) and 17.3 weeks (SD=6.11), respectively. Finally, in group III: 12 patients all with 42C fractures with a consolidation time of 16.86 (SD=2.93) weeks. The average fracture consolidation time for all 44 patients was 16.86 weeks (SD 2.93).
Conclusions Osteosynthesis plates are an alternative to intramedullary nailing for diaphyseal tibial fractures and their outcomes can be favorable as long as the management of soft tissues and the proper principle of stability are taken into account.
Level of evidence IV.
- tibial fractures
- Plates
- internal fixation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
From the beginning of the modern era of osteosynthesis, fixation plates constituted the first choice for surgical treatment of fractures of the tibial shaft.1 ,2 With the advent of intramedullary nailing and due to postoperative problems associated with fixation plates, which are essentially due to two factors, very broad approaches were adopted to expose the area of the surgery thus lacking coverage of soft tissues of the tibia, leading to infection. Hence, there was a non-consolidation in the affected zone; the use of plates for the management of diaphyseal tibial fractures went into a secondary role and were relegated to epiphysial, proximal and distal metaphyseal tibial fractures.3–7 However, given our better understanding of fixation principles, the importance of soft tissue management and the availability of new plate designs, osteosynthesis plates have become a viable option for diaphyseal tibial fractures once again.4–6 ,8 The aim of this study is to present treatment outcomes of osteosynthesis plates in diaphyseal tibial fractures according to the characteristics of the fracture type, fixation principle, and the careful management of soft tissue.
Ethical considerations
Approval by the Ethics Committee (Internal Review Board) was obtained prior to the start of the study.
Methods
A cross-sectional descriptive observational study was conducted by retrospectively analyzing medical records of patients with diaphyseal tibial fractures who were treated surgically by osteosynthesis plates during the period June 2011 to June 2014 at the San José University Hospital (HUSJ) and Susana López de Valencia Hospital (HSLV) in the city of Popayan, Colombia.
We developed a data collection tool in which variables such as age, sex, mechanism of trauma, the Association Osteosynthesis/Osteosynthesis Trauma Association (AO/OTA) Classification of Fractures and Dislocations, type of fracture (open or closed), time of fixing after admission, plate type, length, number of screws used, consolidation time, complications, and early fracture stabilization times were recorded.
Patients with diaphyseal tibial fractures were grouped according to AO/OTA classification.9 ,10 Also, depending on the condition of the tissue found in open fractures they were further grouped according to the Gustillo-Anderson classification system.11
Groups were made according to the type of fracture AO/OTA and the defined principle of stability: group I: simple fractures 42A/B, open or closed reduction, absolute stability; group II: simple fracture 42A/B, closed reduction, Minimally Invasive Plate Osteosynthesis (MIPO) technique, relative stability; group III: multifragmentary fractures 42C, closed reduction MIPO technique, relative stability.
The first author participated in all surgical procedures and radiographic follow-ups were performed every 4 weeks. A fracture was considered consolidated when a bone bridge was observed in one of the corticals in the anteroposterior and lateral projections and when the patient could bear weight without pain. Simple fractures were considered consolidated when the fracture was not visible by radiography. Also, we defined consolidation as normal when it occurred within the first 6 months. It was considered delayed consolidation between 6 and 9 months and pseudoarthrosis if it occurred longer than 9 months.
Surgical technique
All patients underwent surgery under conduction anesthesia and received prophylactic antibiotic treatment with first-generation cephalosporin for 24 hours. No tourniquets were used during the procedure.
In order to achieve fracture reduction based on fracture characteristics and required stability (absolute or relative) we used: external fixators, femoral retractor and Shanz screws or percutaneous clamps. Fracture reduction maneuvering or alignment was performed under close image intensifier monitoring (figure 1).

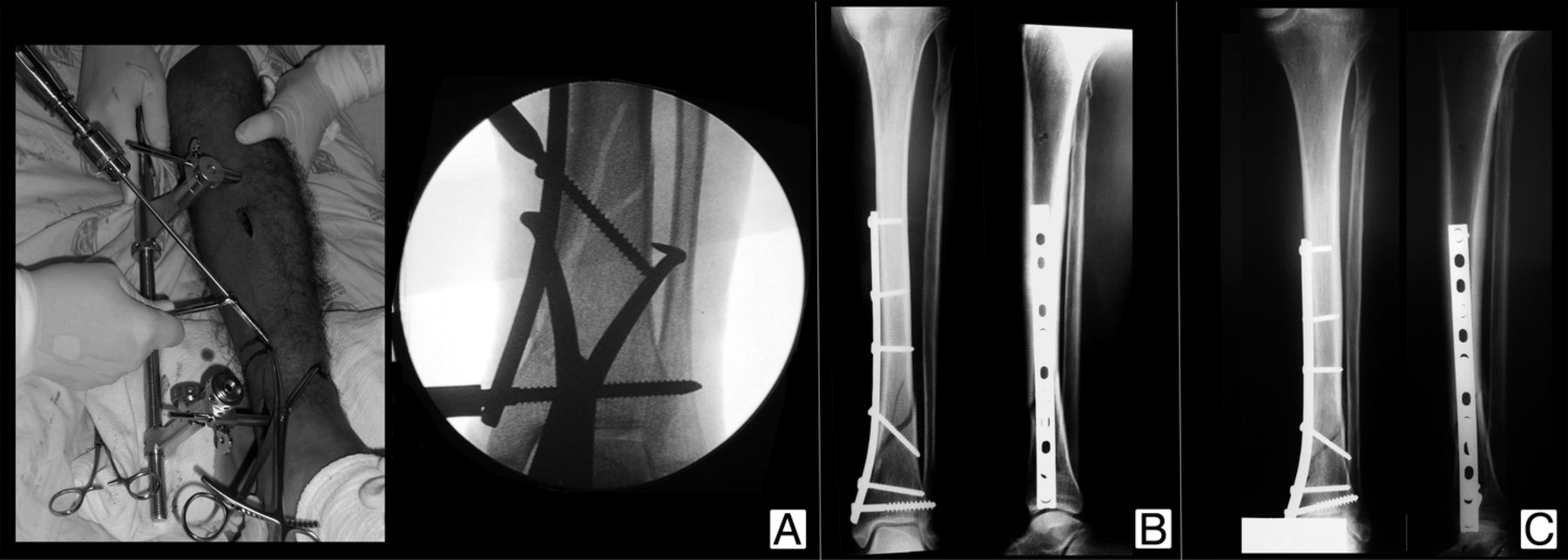
Fracture reduction with absolute stabilization MIPO technique. (A) Closed reduction with percutaneous pinning of the fracture. (B) Absolute stability of the fracture. (C) Bone healing. MIPO, Minimally Invasive Plate Osteosynthesis.
For open fracture cases, we performed conventional management, debridement and temporary external fixation (damage control) in some cases as well as definitive fixation with a plate in others.
The surgical technique for group I (absolute stability) consisted of an anterolateral approach, careful dissection to the medial side while preserving the periosteum, direct fracture reduction using a needle-nose pliers and focal fracture compression with an interfragmentary compression screw or with a fixation plate (figures 1 and 2). Similarly, some cases in this group were performed with closed reduction and interfragmentary compression via the MIPO technique (figure 1).

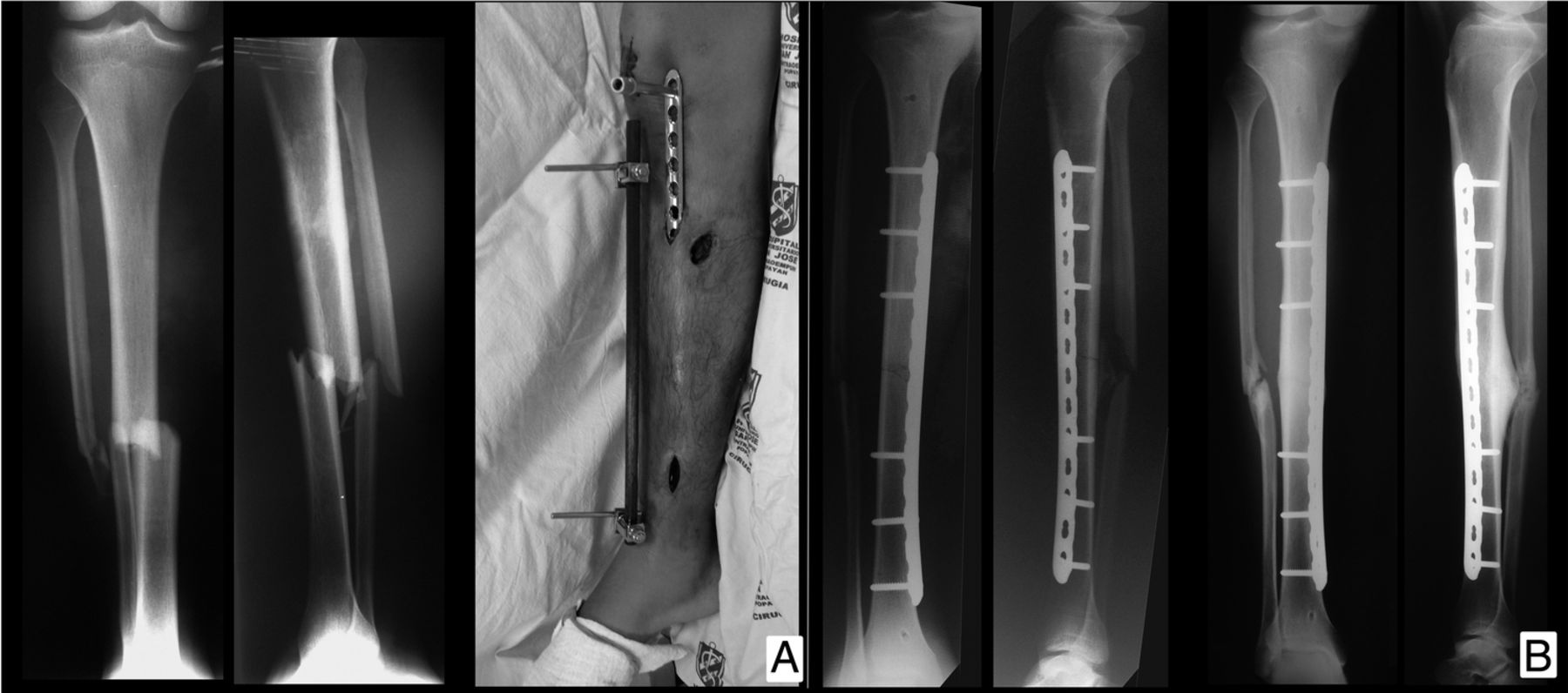
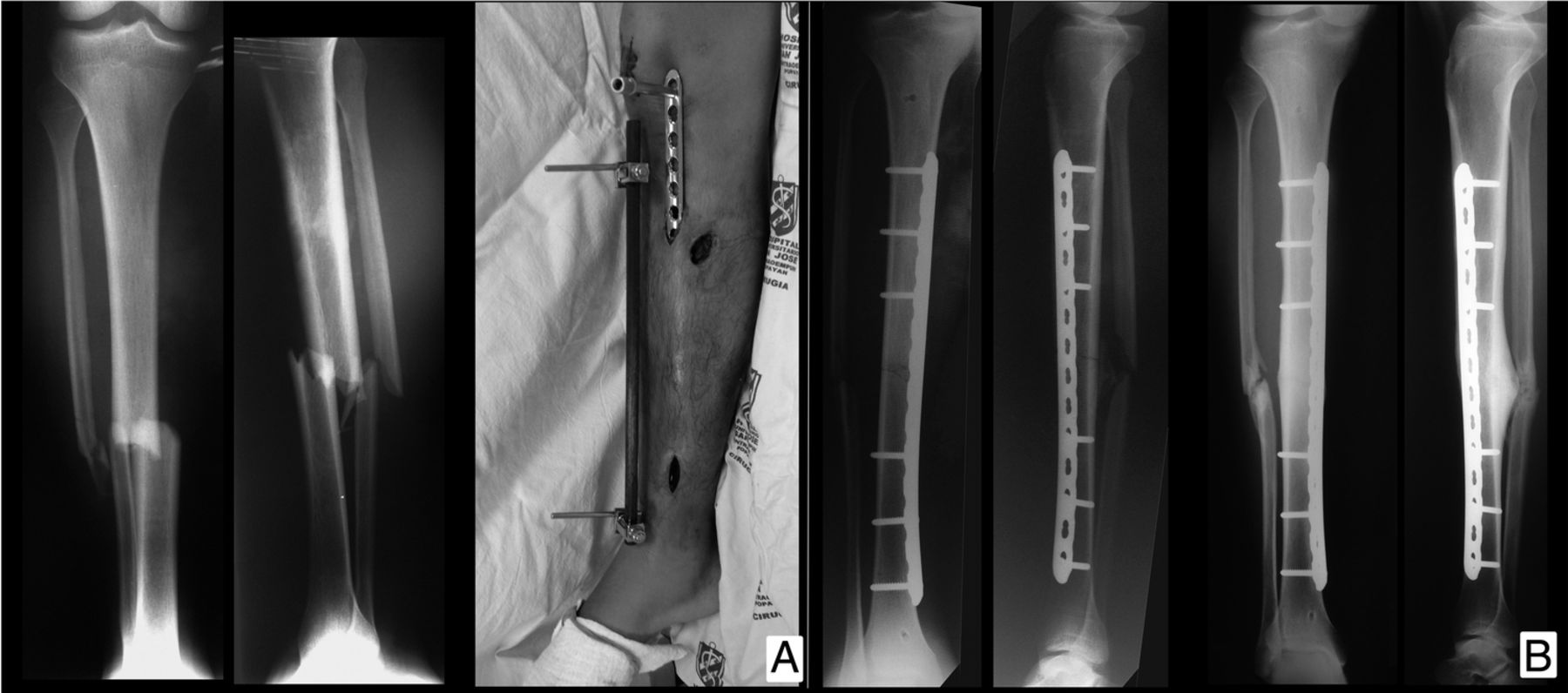
Open reduction and absolute stability. (A) Fracture and opened reduction. (B) Absolute stability and bone healing. MIPO, Minimally Invasive Plate Osteosynthesis.
Group II: simple fractures (MIPO-relative stability): Fracture reduction was performed indirectly using a retractor or an external fixator. This was performed through a distal incision of ∼3–4 cm through which a previously molded plate was placed while protecting the saphenous vein. Reduction and plate position were subsequently verified via fluoroscopy. Screws were fixed percutaneously and long implants and low-density screws were used. Finally, skin closure was performed with 3-0 nylon suture (figure 3).
MIPO technique relative stability simple fracture 42A. (A) Fracture and closed reduction. (B) Relative stabilization with plate and MIPO. MIPO, Minimally Invasive Plate Osteosynthesis.
Group III (multifragmentary fracture-MIPO-relative stability) fracture reduction and fixation were performed similarly to group II; however, screws were distributed near the fracture focal point so that the working length corresponded to the area of comminution (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Indirect reduction by MIPO technique and relative stabilization using multifragmentary plate fracture 42C. (A) Complete fracture and indirect reduction. (B) Stabilization with plate. (C) Bone healing. MIPO, Minimally Invasive Plate Osteosynthesis.
Rehabilitation was started the day after surgery and weight bearing was restricted in all cases until the fourth week at which point partial weight bearing was initiated with the help of crutches. Total weight bearing was authorized depending on clinical and radiographic evolution of the case.
Statistical analysis
We developed an Excel data collection file for collecting information, recording and coding of the variables and a descriptive statistical analysis was performed subsequently using statistical software (STATA V.12). Nominal variables were analyzed for frequencies and proportions with their respective 95% CIs; also, continuous variables were analyzed for their distribution and their averages were calculated with their respective SDs, as well as their maximum and minimum values. Finally, a descriptive analysis of consolidation time of each tibial fracture type studied (AO42) in each respective surgical technique and stabilization approach group was performed. In this study, a purely descriptive statistical analysis was performed on the use of plates in diaphyseal tibial fractures, and no comparison was made for hypothesis test analysis that generated a p value, so it was not the objective to perform a bivariate analysis and there was no control group either.
Results
Medical records from n=45 patients with diaphyseal tibial fractures were analyzed. Thirty were operated at HUSJ and 15 at HSLV, respectively.
The most common type of fracture was 42A (n=27). Five patients in group I (n=20) and five patients in group III (n=14) were stabilized subsequent to damage control of their exposed fracture. Also, the average age of patients was consistent with that of young working age adults and mostly men (table 1).
Patient demographics and fractures based on stabilizing method
The most common mechanism of injury was caused by motor vehicle incidents in which motorcycle accidents were the most frequent with 27 cases (n=45). Patients were operated between 4 and 10 days after the original trauma. Similarly, the right lower limb was most commonly affected in 29 patients (n=45).
Relative stability with fixation plates was performed in 19 fractures in which non-complex fracture lines AO42.A and AO 42.B were included.
The plate type most commonly used was the Locking Compression Plate (LCP); however, in most cases they were used with conventional screws. LCPs with locking screws were used in MIPO multifragmentary fractures (group III).
Plate length according to the number of holes in stabilization techniques on groups II and III was on average 14 and 13 holes, respectively, and the density of the screws had a rate of 0.4 screws/hole for the two groups analyzed.
Consolidation time was similar in all three groups (table 2) and only one case of non-union was found.
Consolidation time in weeks based on surgical technique and type of fracture
Complications
One case in group II did not consolidate due to implant failure at 6 months. Intramedullary nailing and bone grafting were performed to achieve consolidation in this case. Three cases of infection were observed, two of them in group II and one in group III. All infections were treated and resolved by debridement, surgical scrubbing and antibiotic treatment. Six patients had varus or valgus deformities of <10°, but had no clinical or functional presentation.
Discussion
The surgical treatment of diaphyseal tibial fractures has been usually performed using locked intramedullary nailing. This treatment has shown high rates of consolidation with few complications.12–14 Problems associated with the use of fixation plates such as infection, osteosynthesis material exposure, and delay in fracture consolidation have restricted their use.3–7 ,15
However, we find that the adequate understanding of fixation principles, the proper management of soft tissues and the availability of new plate designs have yielded favorable outcomes in the management of diaphyseal tibial fractures.4–6
In this study, the average consolidation of tibial diaphyseal fractures that were part of the absolute closed stabilization group for AO 42.A fractures were 16.4 weeks with a SD of 1.9 and for fractures AO 42.B was 14 weeks with a SD of 6.1. The group of fractures AO 42.C was only MIPO and the consolidation time was 17 weeks with a deviation of 2.62. This average consolidation is similar to that found in the work of Fernandes et al,16 in which the average time of plates consolidation was 16 weeks and nails was 20 weeks with a p 0.019 (Student's t-test). Based on the above, it is stated that the plates may have a shorter consolidation period. In addition, the meta-analysis of Mao et al17 found no significant difference in the management of the fracture with nails or plates both in the consolidation period and in the complications, and similar results have been found in other studies.18–20 This suggests that it is possible to obtain favorable outcomes in diaphyseal tibial fractures using plates and screws as long as careful management of soft tissues is performed and the proper surgical technique is applied according to the selected principle of stability.21 ,22
There were 10 open fractures in our group series (grade I n=3, grade II n=7), all consolidated without complication with the exception of one case mentioned previously, which required a muscle flap. Clifford et al23 ,1 showed a series of 97 diaphyseal tibial fractures that were treated with plates, with low incidence of complications and recommended its use in grades I and II open fractures based on the Gustillo system.
Nineteen patients with simple fractures were treated by means of relative stability, a bridge plate and closed reduction by MIPO technique, which provides biological advantages for consolidation.22 Long plates using an average of 14 holes with a screw density of 0.4 were used to allow micromotion at the focal fracture point and facilitate osteocallus formation. All cases consolidated. Twelve patients with type C multifragmentary fractures were also treated with long plates and in this group the comminution area was left as the working length area. Consolidation was achieved in all fractures in this group as well. Most cases were resolved using conventional screws, and locked screws were only used in cases of fractures extending towards the metaphysis.
Gautier and Sommer24 highlight the importance of the length of the plate, plate working length, and low screw density when using bridge plate techniques for the purpose of fracture consolidation. This same concept was applied to all of our patients. Williams and Shenck25 presented a series of 20 cases of diaphyseal tibial fractures treated with blocking plates with MIPO technique yielding excellent outcomes in 19 patients; findings that are consistent with our work. Other authors like Hasenboehler et al26 have shown favorable results from the use of plates in distal tibial fractures where intramedullary nailing was contraindicated. He et al27 reviewed 11 publications in a meta-analysis comparing the use of intramedullary nails with percutaneous plating in diaphyseal tibial fractures and found no significant differences in the outcomes between these two methods.
A weakness of our study is the small series of cases that were available for review; however, our results support the notion that it is possible to obtain a favorable outcome in diaphyseal tibial fractures using plates and screws as long as careful management of soft tissues is performed and the proper principle of stability is applied according to the fracture.21
This study results support the management of tibial fractures 42A with plates and also warrants future multicenter studies under the conditions of a randomized clinical trial comparing plates with intramedullary nailing, which will aid in treatment decision-making for patients with diaphyseal tibial fractures.
Conclusion
Internal fixation of diaphyseal tibial fractures by plate fixation is not often considered the treatment of choice due to complications that may eventually arise; however, osteosynthesis plates are a viable alternative to intramedullary nailing and their outcomes can be favorable if principles of stability, management of soft tissues, and proper surgical techniques are performed appropriately.
References
Footnotes
This paper was presented at The Congreso Nacional SCCOT Medellin Colombia, April 2016
Contributors JMCS was involved in all surgical interventions described in this work, the postoperative follow-up of the cases, formulation of the research question, literature searching, taking photos, the analysis of the data and the writing, correction and translation of this manuscript. JLO-R was involved in formulation of the research question, literature searching, statistical analysis and data interpretation, writing, correction and translation of this manuscript. ASD was involved in surgical interventions described in this work, the postoperative follow-up of the cases, the analysis of the data and the writing, correction and translation of this manuscript.
Competing interests None declared.
Ethics approval Hospital Susana Lopez de Valencia.
Provenance and peer review Not commissioned; externally peer reviewed.