Article Text

Abstract
An increasing number of potent antiplatelet and anticoagulant medications are being used for the long-term management of cardiac, cerebrovascular, and peripheral vascular conditions. Management of these medications in the perioperative and peri-injury settings can be challenging for surgeons, mandating an understanding of these agents and the risks and benefits of various management strategies. In this two-part review, agents commonly encounter by surgeons in the perioperative and peri-injury settings are discussed and management strategies for patients on long-term antiplatelet and anticoagulant therapy reviewed. In part I, we review warfarin and the new direct oral anticoagulants. In part II, we review antiplatelet agents and assessment of platelet function and the perioperative management of long-term anticoagulant and antiplatelet therapy.
- anticoagulation
- warfarin
- Oral anticoagulation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Long-term antiplatelet and anticoagulant therapy is increasingly encountered in patients undergoing either elective and emergent surgical interventions or who are acutely injured. Antiplatelet and anticoagulant therapy is indicated for the prevention of arterial and venous thromboembolic events including stroke, deep vein thrombosis and pulmonary embolism, and myocardial infarction, with the risk for these prothrombotic disorders significantly increasing with age. The prevalence of atrial fibrillation (AF), the most common indication for long-term anticoagulation, doubles with each advancing decade of age from 0.5% at age 50–59 years to almost 9% at 80–89 years.1 AF currently affects over 2.3 million people in the USA, a number expected to more than double by 2050.2 Patients with AF have a fivefold increase in the risk of stroke, and oral anticoagulants reduce this risk by up to two-thirds.3 ,4 As the geriatric demographic is the fastest growing group within the USA, the frequency of surgical interventions on patients treated with antiplatelet and anticoagulant therapy is likely to increase substantially. In 2014, roughly 48 million people were 65 years or older in the USA, accounting for 15% of the population. By 2060, this number is projected to double to 100 million, making up nearly one-quarter of the total US population.5 Additionally, while individuals 65 years and older currently make up only 15% of the population, they undergo roughly 40% of all the surgical procedures.6 The need for perioperative and peri-injury management of antiplatelet and anticoagulant therapy by surgeons is increasingly prevalent.
For decades, aspirin and warfarin have been the predominant antiplatelet and anticoagulant alternatives. Beginning with the introduction of the antiplatelet agent clopidogrel in 2002, several more potent oral antiplatelet and oral anticoagulant agents have been approved for use. The increase in the number of therapeutic agents and the population at risk requires that surgeons have an understanding of the risks and benefits of reversing these agents in various settings and an understanding of the most appropriate methods for doing so. In this two-part review, agents commonly encountered by surgeons in the perioperative period and management strategies for patients on long-term oral anticoagulation will be reviewed.
In part one of this practice management overview, we review warfarin and its urgent reversal in warfarin-induced coagulopathy, and provide a summary of the newer direct oral anticoagulant (DOAC) agents. In part two, to appear in the next issue of the journal, the management of antiplatelet agents in the surgical setting is reviewed, followed by general recommendations for the management of anticoagulated patients in the perioperative setting.
Warfarin: one of the most dangerous drugs on the formulary
Warfarin, a vitamin K epoxide reductase inhibitor, was first approved as an oral anticoagulant medication in 1954 and was the only option for outpatient anticoagulation for decades. Clinical trials in the 1980s and 1990s demonstrated that warfarin was highly effective at preventing strokes related to AF.7–9 The combination of these trials demonstrated an impressive 62% reduction in the risk of stroke. Despite the development and proliferation of novel oral anticoagulant alternatives, warfarin use remains prevalent and complicates the management of hemorrhagic and non-hemorrhagic surgical emergencies. As recently as 2011, warfarin was one of the top 25 most commonly prescribed medications in the USA.10 Warfarin is Food and Drug Administration (FDA) approved for the management of relatively common medical problems: the prophylaxis and treatment of venous thromboembolism and the reduction of embolic risk associated with non-valvular atrial dysrhythmia, mechanical heart valves, and the sequelae of myocardial infarction. Although it is likely the use of warfarin for these common diseases will decrease to make way for the newer oral anticoagulant alternatives, patients on warfarin will still be encountered frequently by acute care surgeons. In the setting of bleeding or a non-hemorrhagic emergency where the indicated procedure puts the patient at risk for bleeding, the surgeon must be prepared to manage the reversal of this anticoagulant agent.
Warfarin is often a contributor to bleeding events requiring hospitalization. Warfarin, alone or in combination with other mediations, was implicated in one-third of emergency hospitalizations for medication-related adverse events in the elderly between 2007 and 2009.11 The incidence of intracranial hemorrhage (ICH) or retroperitoneal hemorrhage leading to hospitalization is as high as 16% per year, and the risk of fatal bleeding is as high as 3%.12 As warfarin use is relatively common, preinjury warfarin use in trauma victims is frequently encountered. In trauma patients aged 65 and older admitted to US trauma centers, roughly 1 in 10 can be expected to be on warfarin therapy at the time of injury, complicating management.13 Not surprisingly, patients on warfarin therapy at the time of traumatic injury are at higher risk of mortality.13 ,14
The risk of warfarin-associated hemorrhage is correlated with the level of anticoagulation as measured by the international normalized ratio (INR), with the risk of bleeding increased by a factor of 1.43 for each 0.5 unit increase in INR.15 For warfarin to be effective and relatively safe, the therapeutic window for the medication is between an INR of 2 and 3 (or slightly higher for mechanical valves). However, INR levels outside of this therapeutic window over the course of warfarin therapy are commonplace, increasing thrombotic and hemorrhagic risk. Factors contributing to a supratherapeutic INR include interactions with other medications (particularly antibiotics), acute medical illness and traumatic brain injury or other trauma-related hemorrhage.
Urgent warfarin reversal: Fortunately, the anticoagulant effect of warfarin is reversible. The reversal strategy should be tailored to the clinical scenario (active bleeding or impending risk of bleeding from procedure vs no active or impending bleeding risk) and the level of the INR. The remaining section addresses the rapid reversal of warfarin for clinical scenarios in which ongoing therapeutic anticoagulation provides a major risk to the patient.
The reversal strategy is based on warfarin's mechanism of action. As a vitamin K epoxide reductase inhibitor, warfarin competitively inhibits the hepatic synthesis of the vitamin K-dependent clotting factors II, VII, IX, and X. To immediately reverse the anticoagulant effect of warfarin, replacement of the depleted vitamin K-dependent clotting factors is the first course of action. Therapeutic options for factor replacement include fresh frozen plasma (FFP) and prothrombin complex concentrates (PCCs). Other prohemostatic agents, such as activated factor VII and anti-inhibitor coagulant complex (FEIBA), are not recommended for this purpose. To maintain reversal of warfarin, which has an effective half-life of 20–60 hours exceeding some components of FFP and PCC, supplemental vitamin K should be administered. Supplemental vitamin K allows for the resumption of native hepatic synthesis of the vitamin K-dependent factors by overcoming the competitive inhibition of warfarin on the reductase enzyme.
Fresh frozen plasma: Although FFP is commonly used in the USA to reverse warfarin, evidence for its effectiveness with respect to INR correction in the setting of hemorrhage, intracranial, or otherwise is poor. In a study of nearly 5000 FFP transfusions for varying indications, the median reduction in INR was 0.2.16 FFP is a component of whole blood that contains all of the coagulation factors and is stored frozen to preserve the function of the heat-labile factors V and VIII. As such, it cannot be administered quickly because of the time required to thaw. Each unit is ∼200 mL in volume, and the recommended initial dose is 15 mL/kg, which translates to roughly four units for a 70 kg patient. This relatively large volume may be of benefit in situations of significant blood loss, where intravascular volume is depleted. In situations where intravascular volume is not depleted (such as an intracranial bleed or a situation where warfarin needs to be reversed prior to an operation), however, the relatively large volume of plasma required to reverse warfarin can be deleterious, potentially contributing to transfusion-associated circulatory overload in patients with limited cardiac reserve.
Prothrombin complex concentrate: PCCs comprise a group of products containing vitamin K-dependent factors. Initially indicated for the replacement of factor IX in patients with hemophilia B, PCCs have become approved for warfarin reversal in many parts of the world. Although plasma remains the first-line factor replacement therapy in clinical practice within the USA, current practice guidelines from around the world, including the American College of Chest Physicians, recommend PCC as the first-line factor replacement therapy rather than plasma.17 In the USA, one particular PCC, Kcentra, has recently been approved for warfarin reversal by the FDA. All of the available PCCs contain high doses of plasma-derived vitamin K-dependent coagulation factors II, IX, and X. The presence of significant concentration of factor VII in a PCC formulation distinguishes four-factor PCCs, such as Kcentra, from three-factor PCCs with negligible factor VII content.
PCCs offer some significant advantage over plasma in the treatment of warfarin-related coagulopathy. In distinction to plasma, PCCs are stored in lyophilized powder form on the shelf and can be rapidly reconstituted and infused. Also in contrast to plasma, the volume of infusion required to reduce INR is substantially smaller (<100 mL), effectively negating any risk of volume overload. The primary disadvantage of PCCs as compared with plasma is one of cost, whereby PCCs are generally 10-fold the expense of plasma transfusion.18
The efficacy of PCC in comparison with plasma is supported by two industry-funded clinical studies comparing the four-factor PCC Kcentra (trade name Beriplex outside of the USA) with plasma for warfarin reversal efficacy. The first study was a phase IIIb, multicenter, open-label, non-inferiority trial.19 Non-surgical patients on warfarin, with an elevated INR and an acute major bleeding event, were randomized to receive either four-factor PCC or plasma. The end points were rapidity of INR reduction and effectiveness of hemostasis. PCC demonstrated significantly superior efficacy with respect to the rapidity of INR correction, whereby rapid INR reduction (INR<1.3 at 30 min from start of treatment) was achieved in 62% of the PCC group, but only 10% of the plasma group. With respect to hemostatic efficacy (rated by a blinded adjudication board), effective hemostasis in the first 24 hours from start of treatment was similar between groups (72% of PCC patients vs 65% of plasma patients). The second study was also an industry-funded phase IIIb, multicenter, randomized, open-label trial comparing four-factor PCC with plasma in patients needing rapid warfarin reversal before an urgent surgical or invasive procedure.20 The end points of this study were also rapidity of INR reduction and effectiveness of hemostasis. Similar to the prior study, the PCC patients achieved INR correction more rapidly than the plasma patients. In addition, this study demonstrated a significantly higher rate of hemostatic efficacy in the PCC group (90%) versus the plasma group (75%).
Until recently, four-factor PCC has not been available in the USA; therefore, three-factor PCC had been used ‘off-label’ to reverse warfarin. Although a perceived disadvantage of three-factor PCC is the lack of factor VII, proposed advantages compared with four-factor PCC include a lower cost and potentially lower risk of thromboembolic complications. The two formulations of PCC have not, however, been compared to date in a clinical trial. The observational experience with these agents, either alone or in retrospective comparison, is mixed, with some studies suggesting greater efficacy associated with four-factor PCC and others suggesting no difference in efficacy between the two formulations.21–24 However, there is a recurring observation among many of these studies that three-factor PCC, which does not provide factor VII replenishment, is less effective at normalizing INR >4. This may be explained by the fact that only 10–20% level of factor VII activity is required for coagulation, and an INR>4 reflects factor VII activity under 5–10%. Therefore, three-factor PCC may be sufficient for factor replacement when there is sufficient native factor VII activity (>10% or INR<4). Should a patient's baseline INR be >4, it would be reasonable to administer plasma in addition to three-factor PCC to provide exogenous replacement of factor VII.
Vitamin K: Vitamin K is an important adjunct to warfarin reversal. While factor replacement with either FFP or PCC provides immediate exogenous factor replacement, vitamin K supplementation results in native factor synthesis which will sustain the normalization of coagulation. As the half-lives of factors VII and IX are relatively short compared with the half-life of warfarin, the administration of vitamin K prevents recurrence of coagulopathy following the initial factor replacement and diminishes the need for ongoing exogenous factor replacement. When rapid reversal of warfarin is indicated, intravenous vitamin K is recommended over oral or subcutaneous injection, as it has the fastest onset and results in a lower INR 4–6 hours after infusion. There is a risk of an anaphylactoid reaction with intravenous administration that is related predominately to the rate of administration. A total of 5–10 mg of vitamin K should be diluted in 50 mL of intravenous fluid and given over 20 min. Patients should be monitored during administration.
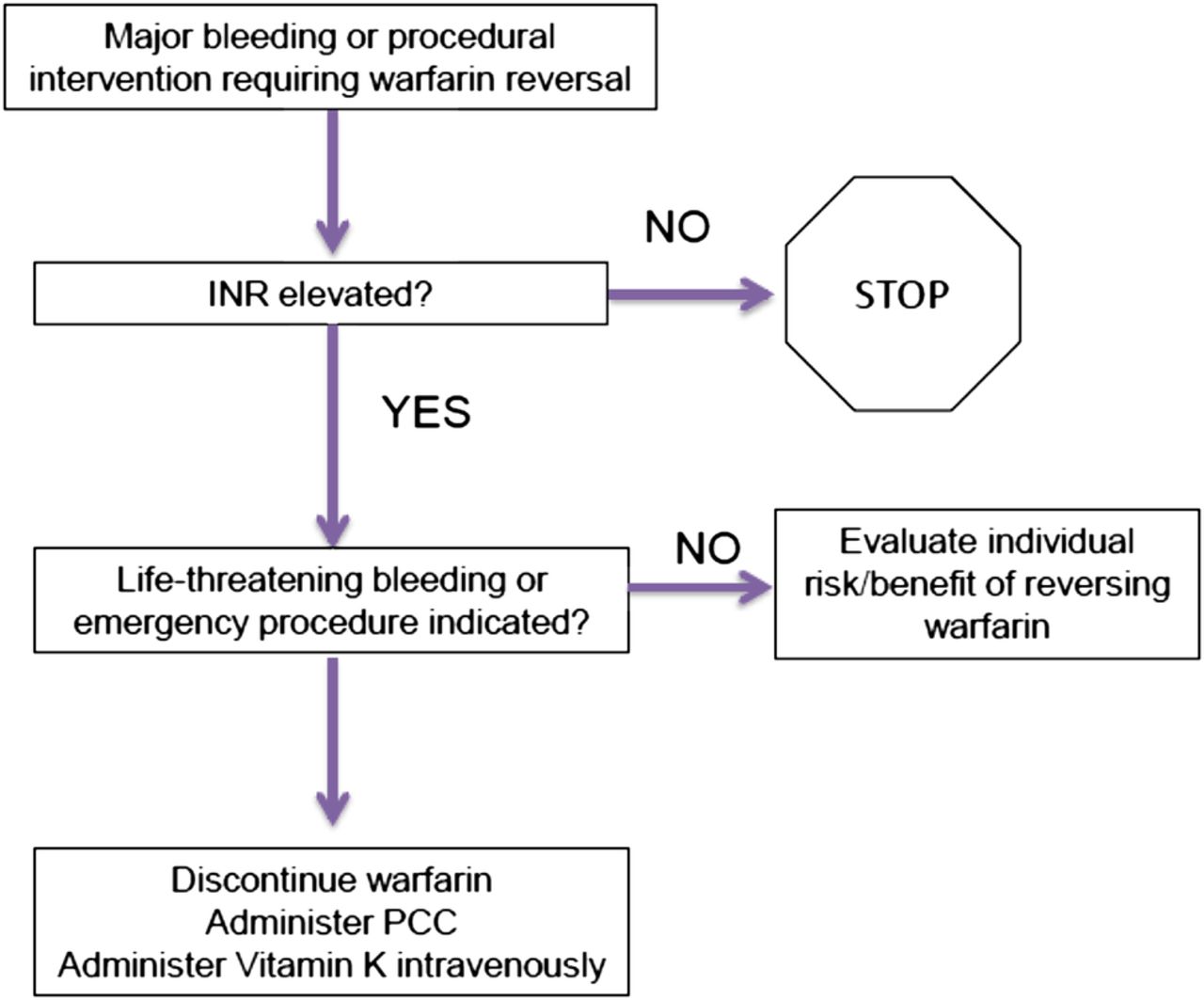
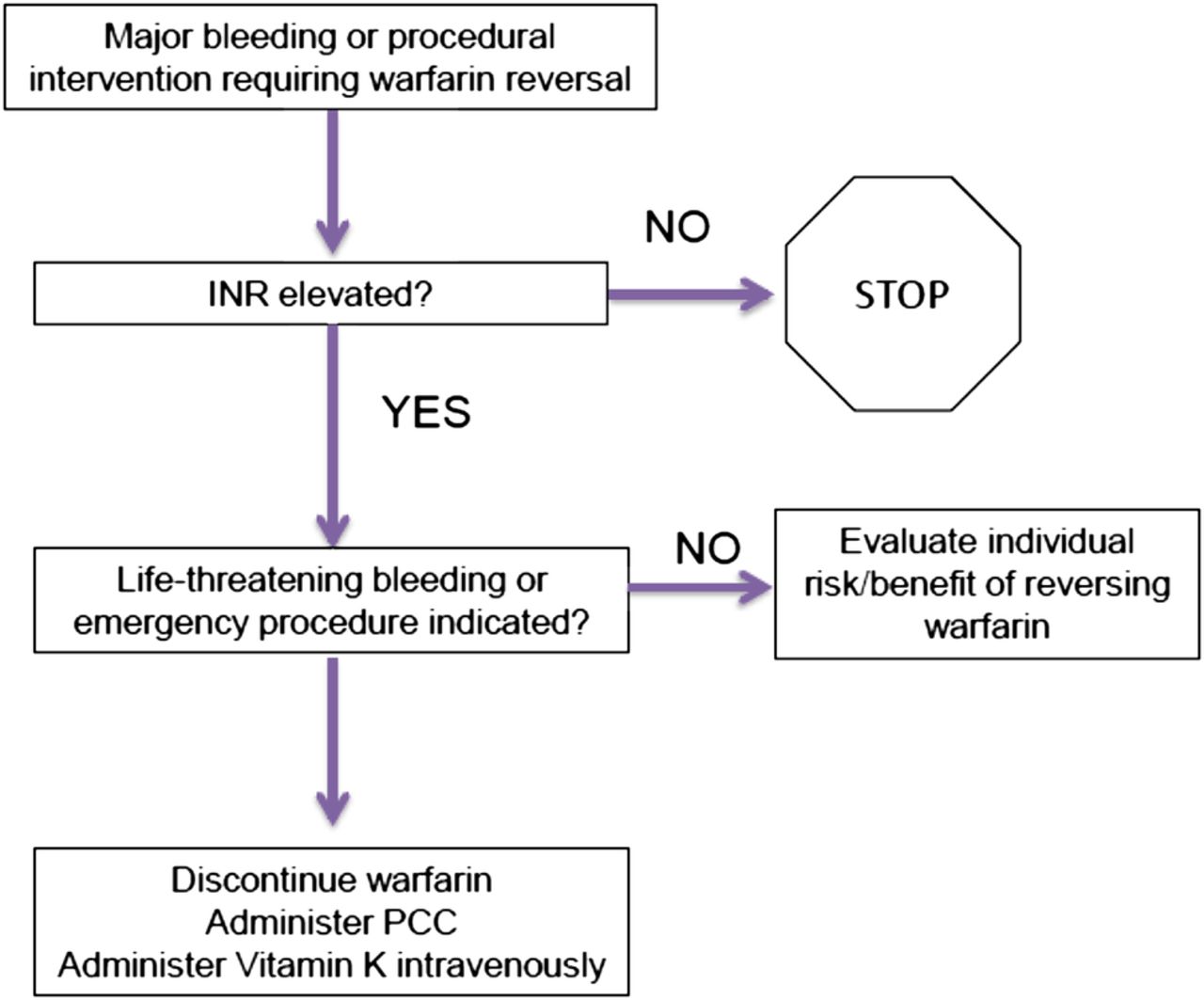
Reversal protocols: Despite the evidence in favor of PCC and intravenous vitamin K, evidence from clinical trials suggests national guidelines are not being followed in practice. Analysis of major bleeding events in patients receiving warfarin in five separate phase III trials comparing warfarin with dabigatran demonstrated only 1.2% of patients received PCC and only 27% received vitamin K.25 To maximize outcomes in high-risk patients, the surgeon must be familiar with the approach to rapid warfarin reversal and prepared to implement it quickly. Rapid correction of warfarin anticoagulation may be facilitated by predefined protocols. A treatment algorithm for warfarin reversal in the emergency setting is demonstrated in figure 1. Clinical consensus guidelines universally support the use of PCC over plasma for exogenous factor replacement due to the more rapid and consistent reversal with lower fluid volumes. Table 1 demonstrates the dosing protocol for vitamin K and PCC at the Elvis Presley Trauma Center, Memphis, Tennessee.
Warfarin reversal protocol (Elvis Presley Trauma Center, Memphis, TN)
{kind=link}
Algorithm for warfarin reversal (Elvis Presley Trauma Center, Memphis, TN). INR, international normalized ratio; PCC, prothrombin complex concentrate.
The new DOACs
As noted above, the most common indication for oral anticoagulation is for the reduction of stroke risk in AF. Since its approval in 1954, warfarin has remained the standard therapy for prevention of thromboembolic events in patients with AF until recently. The difficulty of achieving steady therapeutic dosing and the bleeding risks introduced by warfarin have led to efforts to develop DOACs with improved efficacy and safety. Recently introduced DOACs including rivaroxaban (Xarelto: Bayer HealthCare AG, Leverkusen, Germany), apixaban (Eliquis: Bristol-Myers Squibb Company, Princeton, New Jersey, USA and Pfizer Inc, New York, New York, USA), and dabigatran (Pradaxa: Boehringer Ingelheim Pharmaceuticals, Inc, USA) are rapidly replacing warfarin in the prevention of thromboembolic events in patients with AF. Unlike warfarin, which acts on the vitamin K-dependent factors (factors II, VII, IX, and X), these new agents target specific steps within the coagulation cascade. This targeted approach results in a more favorable pharmacokinetic response, thereby eliminating the need for anticoagulant monitoring and allowing patients to be prescribed a standard dose. Rivaroxaban and apixaban are inhibitors of activated factor X, which is the primary regulator step in the coagulation cascade.26 Dabigatran is a direct thrombin inhibitor acting very specifically within the coagulation cascade where fibrinogen is converted into fibrin.26 Characteristics of these three DOACs are summarized in table 2.
Characteristic of direct oral anticoagulant agents
Three large, randomized controlled trials investigating the effectiveness of these medications, enrolling over 50 000 patients, have established the efficacy and safety of these three agents. These three clinical trials, Randomized Evaluation of Long-term Anticoagulant Therapy (RE-LY),27 Rivaroxaban Once-Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET-AF),28 and Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE),29 will be briefly discussed below highlighting efficacy and safety.
RE-LY clinical trial (dabigatran vs warfarin): The RE-LY trial was designed to evaluate the effectiveness of an oral direct factor Xa inhibitor dabigatran against warfarin among patients with non-valvular AF.27 This multicenter, blinded, randomized control trial had the primary end point of stroke and systemic embolism (non-inferiority). Patients were randomized to dabigatran (low dose (n=6015) or high dose (n=6076)) daily versus dose-adjusted warfarin with target INR 2–3 (n=6022). A total of 18 113 patients were randomized into the study. Based on the primary outcome of stroke or systemic embolization prevention, this study demonstrated (1) low-dose dabigatran to be non-inferior to warfarin (1.53% vs 1.69%, RR 0.91, 95% CI 0.74 to 1.11, p<0.001) and (2) high-dose dabigatran to be superior to warfarin (1.11% vs 1.69%, RR 0.66, 95% CI 0.53 to 0.82, p<0.001). Dabigatran dose of 150 mg reduced the risk of stroke compared to warfarin by 34%. Also seen in this study was a reduction in the rate of ischemic strokes. Even more compelling was the reduction in hemorrhagic stroke, which was an unexpected finding of the study (0.10% vs 0.38%, respectively; p<0.001). All-cause mortality in the high-dose dabigatran versus warfarin group was 3.64% vs 4.13% (p=0.051).
ROCKET-AF clinical trial (rivaroxaban vs warfarin): The goal of the ROCKET-AF trial was to evaluate the effectiveness of an oral direct factor Xa inhibitor rivaroxaban against warfarin among patients with non-valvular AF with either a history of systemic embolization or at least two additional risk factors defined as congestive heart failure (CHF), left ventricular ejection fraction (LVEF) <35%, hypertension (HTN), age >75, or diabetes.28 This blinded, randomized control trial had the primary end point of stroke or systemic embolism (non-inferiority). Patients were randomized to rivaroxaban 20 mg oral daily (n=7131) versus dose-adjusted warfarin with target INR 2–3 (n=7133). A total of 14 264 patients were randomized into the study. Based on the primary outcome of stroke or systemic embolization prevention, this study demonstrated rivaroxaban was non-inferior to warfarin in the intention-to-treat analysis (2.1 vs 2.4 events per 100 patient-years, HR 0.88; 95% CI 0.75 to 1.03; p<0.001 for non-inferiority; p=0.12 for superiority). All-cause mortality was 1.9 vs 2.2 events per 100 patient-years. A comparison of adverse events demonstrated similar rates for all major and non-major clinically relevant bleeding episodes (14.9 vs 14.5, p=0.44). However, there was a reduction of ICHs (0.5 vs 0.7, p=0.019) and major gastrointestinal bleeding episodes (3.2% vs 2.2%, p<0.001) with rivaroxaban. The authors concluded that the use of the direct Xa inhibitor rivaroxaban was non-inferior to warfarin. However, the on-treatment analysis revealed that rivaroxaban was associated with reduced incidence of stroke without an excess of major bleeding or serious adverse events.
ARISTOTLE clinical trial (apixaban vs warfarin): The ARISTOTLE trial compared apixaban (5 mg twice daily) with warfarin in patients with non-valvular AF and at least one additional risk factor for stroke.29 This blinded, multicenter, randomized control trial had the primary end point of stroke or systemic embolism. Patients were randomized to apixaban (n=9120) versus dose-adjusted warfarin with target INR 2–3 (n=9081). A total of 18 201 patients were randomized into the study. Based on the primary outcome of stroke or systemic embolization prevention, this study demonstrated apixaban was superior to warfarin in preventing stroke or embolism (1.27% vs 1.60% per year, HR 0.79; 95% CI 0.66 to 0.95; p=0.01 for superiority, p<0.001 for non-inferiority). There was a modest reduction in ischemic stroke by about 8%. The major advantage of apixaban was observed with the reduction of hemorrhagic stroke where the prevalence was cut in half. This study was the only trial to show less major bleeding than warfarin. Complications of bleeding including fatal bleeds and ICH were cut by more than half. Also noteworthy, this is the only trial which demonstrated a statistically significant improvement in mortality rate. There was an 11% reduction in all-cause mortality (3.52% per year vs 3.94% per year, HR 0.89; 95% CI 0.80 to 0.99; p=0.047). In summary, patients with AF and at least one risk factor, apixaban was associated with a greater reduction in rates of stroke or systemic embolism while having a lower rate of bleeding than warfarin.
Summary of results and reversing agents: The DOACs are effective at reducing ischemic strokes. The most significant benefits of these drugs are the reduction of hemorrhagic strokes which was cut in half and the profound reduction of ICH. Additionally, the reduced need for therapeutic monitoring is a substantial benefit of the new oral anticoagulants over warfarin. A major concern regarding this class of agents has been the lack of reversal agents in the emergent settings.30 Each of these drugs has a half-life between 8 and 15 hours, and their use can significantly complicate the management of acutely injured patients and increase bleeding risk for emergent surgical procedures.
Four-factor PCCs have the potential to reverse bleeding in the setting of DOAC therapy based on their ability to increase levels of factors II, VII, IX, and X and are recommended by some authors in the setting of life-threatening bleeding.30 ,31 However, there are insufficient data to definitively conclude reversing the DOAC effect as judged by laboratory tests correlates with improved clinical outcomes.30 Recombinant FVIIa is only partially effective for reversing DOACs in experimental models and would likely increase the thrombotic risk relative to PCC. Several agents are in development for the specific reversal of DOAC activity. At present, only dabigatran has an approved reversal agent on the market. Idarucizumab, a humanized monoclonal antibody fragment that binds to dabigatran, received accelerated approval in October 2015 based on limited clinical data and a reduction of unbound dabigatran and normalization of coagulation parameters in healthy volunteers.32 Its use in acutely ill patients has not been extensively studied, although trials are ongoing. At least two other agents are in clinical trials, andexanet alfa (recombinant, modified human factor Xa) and ciraparantag (PER977—a water-soluble, small-molecule, non-specific reversal agent).30 These drugs have not received FDA approval.
References
Footnotes
Portions of this review were presented at the 2015 Clinical Congress of the American College of Surgeons, October 7, 2015, Chicago, IL.
Contributors Each author has contributed substantially to this manuscript and has approved the final version.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.