Article Text

Abstract
Objectives The triage of trauma patients with potential COVID-19 remains a major challenge given that a significant number of patients may be asymptomatic or pre-symptomatic. This study aimed to compare the specificity and sensitivity of available triage systems for COVID-19 among trauma patients. Furthermore, it aimed to develop a novel triage system for SARS-CoV-2 detection among trauma patients in centers with limited resources.
Methods All patients referred to our center from February to May 2020 were enrolled in this prospective study. We evaluated the SARS-CoV-2 triage protocols from the WHO, the Iranian Ministry of Health and Medical Education (MOHME), and the European Centre for Disease Control and Prevention (ECDC) for their effectiveness in finding COVID-19 infected individuals among trauma patients. We then used these data to design a stepwise triage protocol to detect COVID-19 positive patients among trauma patients.
Results According to our findings, the WHO protocol showed 100% specificity and 13.3% sensitivity. The MOHME protocol had 99% specificity and 23.3% sensitivity. While the ECDC protocol showed 93.3% sensitivity and 89.5% specificity, it did not prioritize patients based on traumatic injuries and unstable conditions. Our stepwise triage protocol, which prioritizes traumatic injuries, had 93.3% sensitivity and 90.3% specificity.
Conclusion Our study shows that the triage protocols from the WHO, MOHME and ECDC are not best equipped to diagnose SARS-CoV-2 infected individuals among trauma patients. In our proposed stepwise triage system, patients are triaged according to their hemodynamic conditions, COVID-19 related clinical states, and COVID-19 related laboratory findings. Our triage model can lead to more accurate and resource-effective management of trauma patients with potential COVID-19 infection.
Level of evidence Level Ⅲ.
- COVID-19
- multiple trauma
- diagnosis
- triage
Data availability statement
Data are available upon reasonable request. No free text required.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Following the sudden and unexpected outbreak of SARS-CoV-2 in Wuhan, China, in December 2019, and its rapid spread around the world, on March 11, 2020, the WHO declared the SARS-CoV-2 a global pandemic and attempted to mobilize all available resources to combat this pandemic.1
However, given the very rapid expansion of the illness and its unique and disproportionately severe presentation, this new pandemic has led to a major global health crisis and has caused the death of more than 1.53 million people since its emergence.2 3 (As of the date of this paper, April 4, 2021, this number is now in excess of 2.8 million people.) There is no definitive treatment, and despite the discovery of the vaccine, its availability, distribution and universal access remain a challenge.4 To this end, early detection and strict isolation play an essential role in decreasing the transmission rate, leading to better management of healthcare resources, and improvavailability of treatment facilities for critically ill patients and personal protective equipment (PPE).5
This global pandemic has severely strained healthcare resources, and shortages of various types, such as hospital beds, PPE, skilled healthcare workers, etc, have further complicated this global crisis. One of the proposed mechanisms for slowing the pandemic and limiting the number of infected individuals has been widespread community testing and isolating infected individuals. Unfortunately, in under-resourced countries, which account for the vast majority of the world, widespread testing has not been available, so those countries have resorted to testing only those individuals who are clinically symptomatic. This presents a particular problem since a significant number of carriers of the disease may be asymptomatic. Thus, early identification of both symptomatic patients, as well as asymptomatic carriers, remains a challenge and, if overcome, may help in slowing the pandemic significantly, leading further to the more effective management of SARS-CoV-2 on a global scale.
In this regard, the triage protocol for trauma patients has been particularly problematic. Before the SARS-CoV-2 outbreak, the trauma triage protocol was relatively uncomplicated and focused solely on treating life-threatening injuries in the shortest possible time. However, the SARS-CoV-2 outbreak and the presence of asymptomatic carriers poses a new and uncontested challenge regarding their triage and the protection of healthcare staff and other trauma patients. So far, the question of the potential triage of a trauma patient with an unknown SARS-CoV-2 status remains unanswered.
Currently, reverse transcription-polymerase chain reaction (RT-PCR) seems to be the most widely used serological test in most healthcare systems to confirm the diagnosis in people with suspected COVID-19 infection. The diagnosis of suspected patients is based on the history of clinical symptoms associated with the disease and epidemiological history. The WHO has identified the presence of fever with symptoms of acute respiratory infection in a patient with close contact with a confirmed patient, or a history of traveling to endemic areas within 2 weeks before the onset of symptoms, as diagnostic criteria for a suspected patient.6 Other healthcare organizations in different countries have characterized suspicious patients, with some modification in the above definition. The Iranian Ministry of Health and Medical Education (MOHME) has defined the ‘suspected patient’ as someone with acute respiratory symptoms along with a history of close contact with a confirmed patient or travel to endemic areas within the previous 2 weeks. The presence of a fever is not a mandatory symptom in this definition.7 According to the European Centres for Disease Control (ECDC), the presence of fever or respiratory symptoms or impaired sense of smell and taste is sufficient to diagnose the possibility of the disease, as shown in table 1.8
Definition of suspicious COVID-19 cases, according to WHO, MOHME, and ECDC protocols.
The other modality of para-clinical investigation, which has been widely used as an adjunct diagnostic tool for SARS-CoV-2, is the chest CT. The presence of ground-glass opacity on chest CT within the clinical context has been used to confirm the diagnosis of SARS-CoV-2. While the chest CT findings do not necessarily associate with the clinical status of the SARS-CoV-2 patients, another complication in this regard is the utility of the chest CT for the diagnosis of SARS-CoV-2 among trauma patients, given that often trauma patients suffer from pulmonary contusion and potential ground-glass opacities on their chest CT, which may be secondary to their lung trauma and not their SARS-CoV-2 infection.9
The effective management of trauma patients with potential COVID-19 infection may be complicated by a number of other potential factors, including unstable clinical conditions, the presence of brain injury and decreased level of consciousness,5–7 the presence of fever secondary to trauma, the rise in inflammatory markers as well as leukocytosis secondary to trauma, and the impracticality of obtaining an accurate clinical history, along with clinical symptoms such as pulmonary contusion. Taken together, the use of available triage systems as well as diagnostic methods, whether case definition, certain laboratory findings or chest CT, etc, do not seem to fully apply to trauma patients. Furthermore, the asymptomatic carriers of SARS-CoV-2 pose a major challenge given that there is no established protocol for evaluating these patients in trauma centers.10 11
Given the significant limitations of global healthcare resources as well as the difficulties mentioned above and the shortcomings in available triage protocols, as they relate to trauma patients, we set out in this study to compare the available triage methods and also to establish a novel triage system which could prove to be more accurate and resource effective.
Methods
All adult patients referred to the largest trauma center in the south of Iran, Rajaee Hospital, Shiraz, from February 1 to May 30, 2020, who had been evaluated with RT-PCR for COVID-19, were enrolled in this prospective study. Patients who had not undergone RT-PCR for COVID-19 were excluded. This proposed triage system was approved by the hospital Trauma Quality Improvement Program (TQIP). Patients enrolled in the study included those with unstable vital signs, decreased level of consciousness (LOC), typical features of COVID-19 in their chest CT scans, all suspected patients according to the MOHME definition, and those who developed COVID-19 related symptoms during their hospital course. In addition, all patients admitted to the intensive care unit (ICU) were enrolled and evaluated with an RT-PCR test to assess asymptomatic patients at the time of arrival. In addition to regular sampling for RT-PCR from individuals who were transferred to the COVID-19 special wards, we took another sample for RT-PCR from the lower respiratory tract (according to the WHO guideline) when needed. Following the discharge of PCR-negative patients from the special COVID-19 wards, they were followed for another 2 weeks to monitor for potential hospital-acquired COVID-19.
We classified the patients based on their RT-PCR results into definite and non-infected groups. At first, patients were assessed by the WHO, ECDC, and MOHME criteria to find suspected cases (table 1). The sensitivity and specificity of each protocol were then calculated. Given the low accuracy and poor applicability of these triage protocols, we then used a combination of both objective (vital signs and laboratory data) and subjective parameters to develop a novel triage system with higher applicability and accuracy. These parameters were selected according to comparisons between definite and non-infected cases (table 2) and other studies conducted in non-trauma patients.12
Demographic data and clinical histories of the suspicious cases (n=132)
Moreover, the laboratory tests were chosen based on their routine use in trauma centers and the rapid availability of laboratory results (<1 hour). In each of the following stages, patients meeting our criteria were transferred to the COVID-19 special wards for further evaluation while the others were assessed in the next stages. At first, we recommended considering patients with unstable vital signs, decreased LOC, and in need of life-saving surgeries as suspicious for COVID-19 and transferred them to our special wards. Medical staff dealing with these patients used appropriate PPE. In the second stage, we assessed the patients using their medical histories, epidemiological risk factors (as subjective parameters), body temperature, respiratory rate (RR), and oxygen saturation (as objective parameters). In the third stage, we evaluated the individuals according to their laboratory data for potential identification of asymptomatic carriers. The other patients were closely observed for the emergence of COVID-19 related signs and symptoms. Of note, all patients admitted to the ICU wards and those who developed COVID-19 related symptoms were also evaluated during the hospital course. Figure 1 illustrates our recommended pathway for the management of trauma patients in detail.
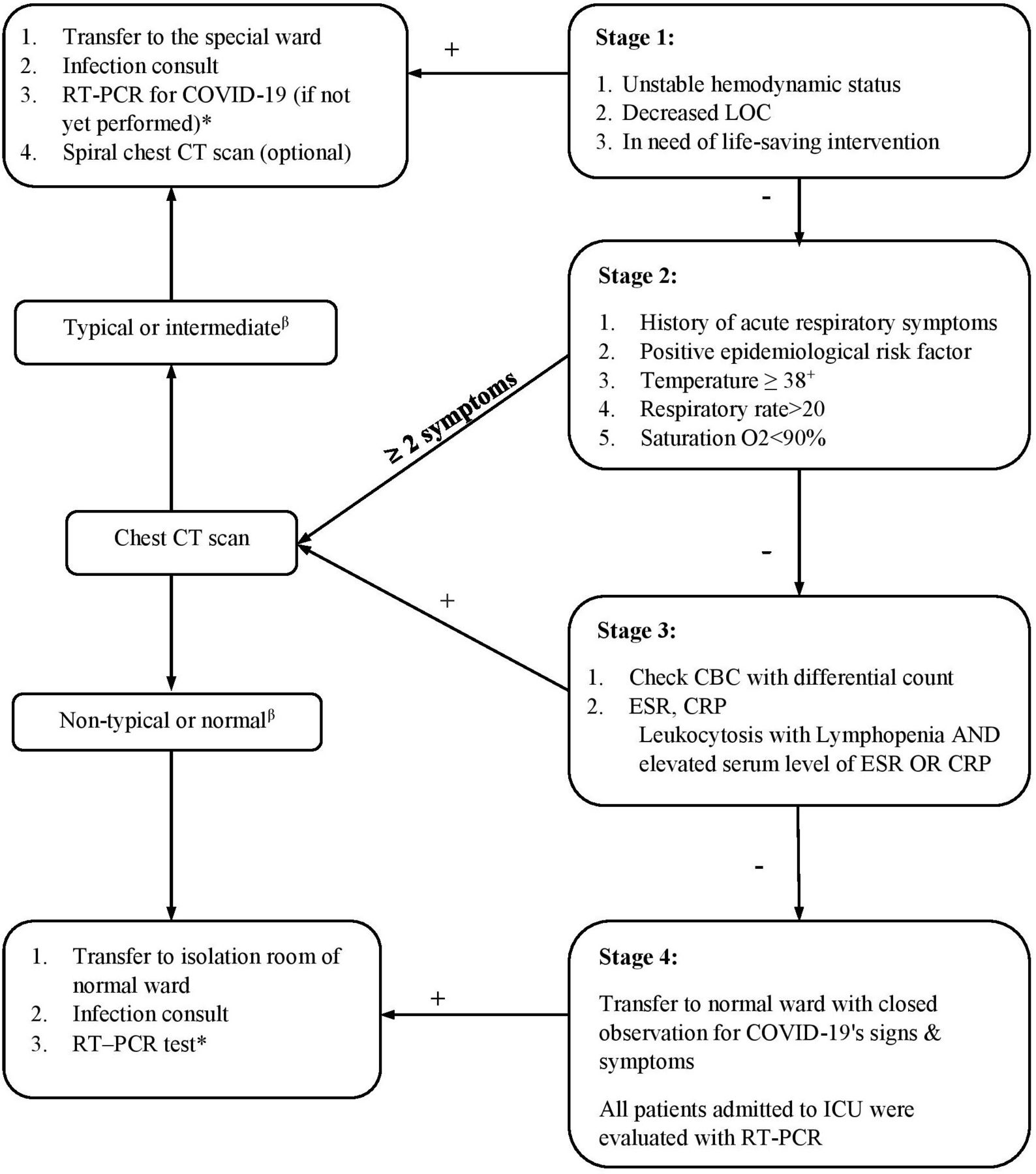
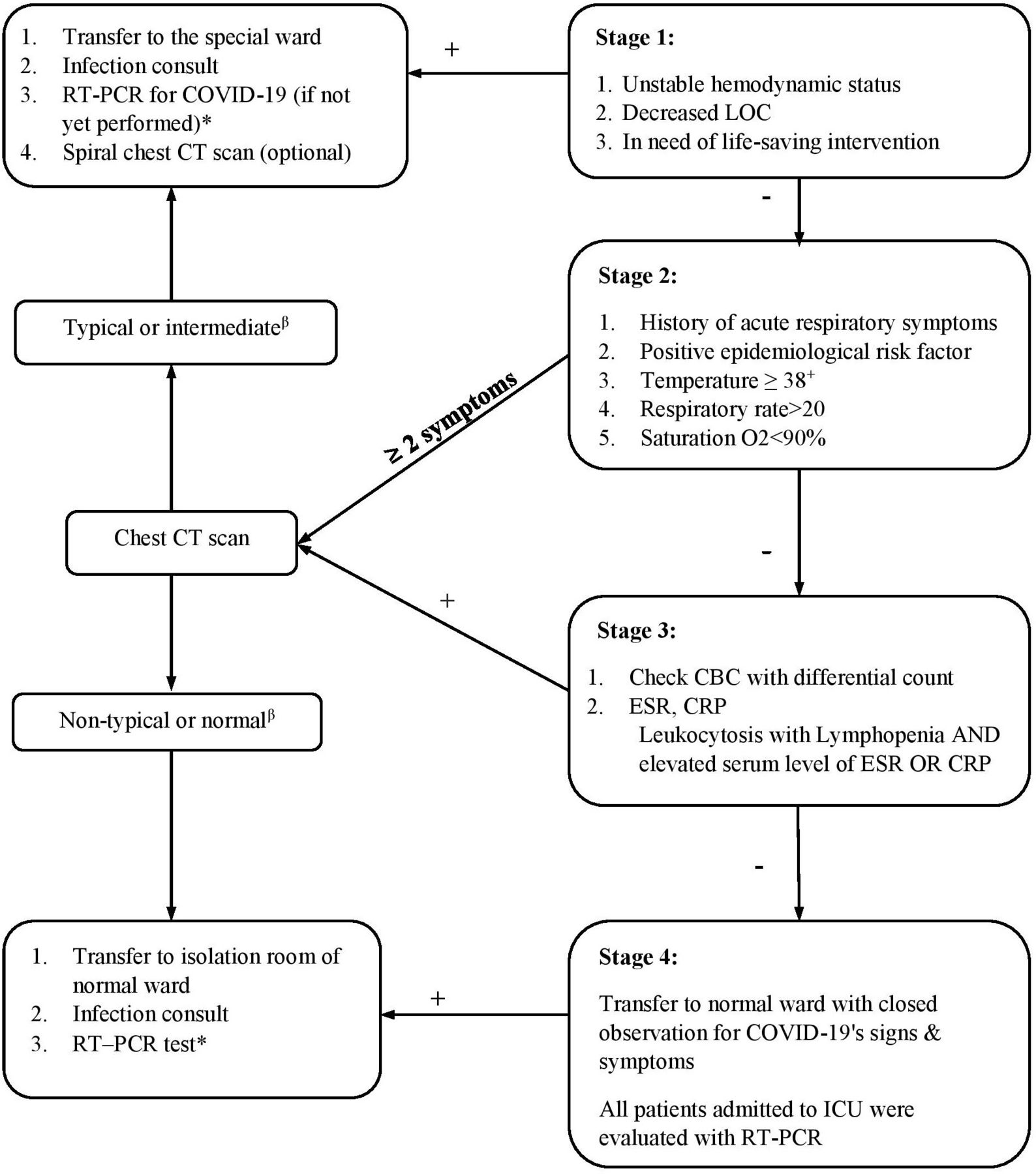{kind=link}
In our triage model, patients with unstable vital signs, decreased LOC, and in need of life-saving surgeries were considered suspicious for COVID-19 and transferred to special wards after proper resuscitation. In the second step, other patients who did not meet the above criteria, were assessed using their medical histories, epidemiological risk factors (as subjective parameters) and body temperature, respiratory rate (RR), and oxygen saturation (as objective parameters). In the third step, we evaluated individuals according to the obtained laboratory data for evaluating asymptomatic carriers. All other patients were transferred to regular wards and were closely monitored for signs and symptoms of COVID-19. All patients admitted to the ICU wards and those who developed COVID-19 related symptoms were also evaluated during their hospital course using RT-PCR. *A negative result was repeated 4 days later from the lower respiratory tract. **All ICU-admitted patients: evaluated by RT-PCR test. +Two times in 30 min. β, according RSNA classification. CBC, complete blood count; CRP, C-reactive peptide; ESR, erythrocyte sedimentation rate; ICU, intensive care unit; LOC, level of consciousness; RSNA, Radiological Society of North America; RT-PCR, reverse transcription-polymerase chain reaction.
Collected data were analyzed using the Statistical Package for Social Sciences, version 20.0 (SPSS Inc, Chicago, IL). Quantitative variables were presented as mean±SD, although categorical variables were shown as frequencies (numbers and percentages). We used the χ2 test or Fisher’s exact test to compare categorical variables and independent t-test or Mann-Whitney U test for quantitative variables. Moreover, sensitivity and specificity were calculated for each protocol. The value of p≤0.05 was considered statistically significant.
Our study was approved by the Institutional Review Board (IRB) of Shiraz University of Medical Sciences (SUMS) with an ethics number of IR.SUMS.REC.1399061. When available, demographic data, past medical histories, other comorbidities, and epidemiological risk factors were obtained from the patients’ medical records. Some of the records were completed according to the patient or their next of kin at the hospital on their arrival or when they became stable. Furthermore, the laboratory data were collected from the centre’s data bank. Given the surveying nature of our study and the fact that our study did not require any additional imaging or blood work outside the set protocols by our hospital, the IRB of SUMS did not mandate written informed consents from the patients.
Results
Six hundred and forty adult patients were enrolled in this study between February and May 2020 based on our center’s triage system. The first triage system’s criteria included all patients with unstable vital signs (42 patients), decreased level of consciousness (30 patients), suspicious patients according to MOHME criteria (eight patients), typical features of COVID-19 in chest CT scan based on Radiological Society of North America (RSNA) criteria (31 patients), all patients admitted in ICU during the hospital course (517 patients), and those who developed COVID-19 symptoms during the hospital course (12 patients). All the patients were evaluated by RT-PCR for COVID-19. Patients admitted in the ICUs and those who developed COVID-19 symptoms during hospitalization were transferred to the wards for COVID-19 patients if RT-PCR tests were positive.
One hundred and thirty-two individuals of all enrolled patients (20.62%) were detected as suspicious cases and transferred to COVID-19 special wards according to our triage pathway. They were classified as definite (30 patients, 22.72%) and non-infected (102 patients, 77.27%) groups based on the RT-PCR test results. Demographic data and clinical histories of these suspicious patients are shown in table 2. The comparison of definite and non-infected patients admitted to the gray wards showed no difference in the average length of stay (ALOS) in the hospital, the need for ICU admission, the need for intubation, and the mortality rate between them. Concerning the symptoms and clinical histories associated with COVID-19, the history of direct contact with a COVID-19 patient, respiratory distress, and abdominal pain were significantly higher in the definite group. Also, evaluation of patients with a positive RT-PCR test showed that 10 individuals (33.3%) had no COVID-19 related respiratory symptoms at admission (asymptomatic carriers) who were screened due to other criteria of our center’s screening system.
Based on the completed data bank, we evaluated the WHO, ECDE and MOHME protocols for their sensitivity and specificity in detecting COVID-19 definite patients. Sensitivity and specificity of these protocols have been carried out based on the completed history of patients regarding the existence of COVID-19 related symptoms and regardless of the ability to obtain these symptoms at admission. The results are shown in table 3.
Diagnostic capability of available protocols in detecting COVID-19 among trauma patients
According to the WHO protocol (table 1), only four patients (3.03% of all suspected patients) were suspected of COVID-19, and all of them had positive RT-PCR (specificity 100%). Unfortunately, only two out of these four cases were able to give histories to the medical staff; the other two had decreased LOC and hemorrhagic shock. therefore, we could take a history only when they were stabilized. Therefore, it seemed we already missed 50% of suspected patients.
Regarding the MOHME protocol (table 1), only eight cases (6.06% of all suspected patients) met the criteria for the suspicious case, and seven of them had positive RT-PCR results. Also, two RT-PCR positive patients were intubated due to hypoxia, so the physicians could not take an appropriate history. The ECDC protocol had the highest sensitivity to detect COVID-19 among trauma victims, but 10 cases could not report a proper history due to pre-hospital intubation and decreased LOC. While the ECDC protocol showed 93.3% sensitivity and 89.5% specificity, it did not prioritize patients based on traumatic injuries or unstable conditions.
Data obtained from our study showed that in our proposed novel triage system (figure 1), among enrolled patients, only two patients with positive RT-PCR tests were not found to have had COVID-19. These two patients were asymptomatic carriers and only had an increased C-reactive peptide (CRP) blood level. Therefore, our recommended novel triage system showed 93.3% sensitivity and 90.3% specificity in diagnosing COVID-19 in trauma patients enrolled in the study.
Discussion
Asymptomatic or pre-symptomatic carriers are believed to be the primary source for the COVID-19 spread and pose a challenge for pandemic control.13–15 We know that several trauma patients might lack the ability to report a proper history of close contact to positive patients and COVID-19 signs and symptoms in conditions such as traumatic brain injury, hemodynamic instability, severe pain, and even anxiety at the hospital arrival. Therefore, physicians cannot exclusively rely on subjective parameters routinely recommended by the WHO, ECDC, and MOHME to find patients with potential COVID-19.6–8 Moreover, trauma patients usually have abnormal vital signs and/or laboratory data. Indeed, Balvers et al have shown that hypothermia is common in traumatic injuries which may mask the COVID-19-induced fever. Furthermore blood transfusions may lead to fever in trauma patients, although in non-trauma patients, fever (>38°C) was one of the most common findings among COVID-19 patients (43%).16 17 These concomitant conditions make the body temperature an impractical parameter in the potential detection of COVID-19 infected patients. Given the inapplicability of the available triage systems for detection of COVID-19-positive individuals among trauma patients, we hypothesized that a more practical and accurate triage system can be developed in which these limitations may be addressed.
The optimal approach would be the performance of RT-PCR testing for all trauma patients at the time of admission and their isolation in COVID-19 special wards until the PCR results become available. However, many low- and middle-income countries do not have the necessary resources to comply with this approach, given the significant limitations in their hospitals’ isolation rooms and equipment, PCR kits, and PPE. In addition, the higher proportion of trauma patients in Iran and other low- and middle-income countries could make the overcrowded trauma centers a potential focal point for spreading the disease.18 19
Evaluation of sensitivity and specificity of the three conventional (WHO, ECDC and MOHME) protocols showed that these subjective-based protocols could not detect COVID-19 in trauma patients effectively on hospital arrival; therefore, they might increase the risk of cross-infection between infected patients or medical staff, and other non-infected individuals. Due to the weakness of conventional triage systems as well as limitations in relation to trauma patients, and with the aim of achieving a more effective diagnosis of COVID-19 patients at the time of admission, we recommend this novel stepwise triage system. This triage protocol would clearly help in better and more practical management of trauma patients with potential COVID-19 infection, particularly in countries with limited healthcare resources. This resource limitation may potentially be related to COVID-19 definite diagnostic tests, access to rapid definite diagnostic tests, limitations of special wards for COVID-19 patients, and PPE.
Considering the priority of treating life-threatening injuries, and the inability to obtain a history related to COVID-19 symptoms in some trauma patients, we recommend that all patients with unstable vital signs, decreased level of consciousness and in need of life-saving procedures be considered as suspected COVID-19 patients, as indicated in the first step of our proposed triage protocol. Our data have revealed that implementing this precautionary approach in the triage of trauma patients will identify a significant number of RT-PCR positive patients early on. This will help limit the spread of COVID-19 among other trauma patients as well as those providing care in the trauma centers
A group of subjective as well as objective criteria, including history of acute respiratory symptoms, positive epidemiological risk factors, temperature ≥38°C, respiratory rate >20 and O2 saturation <90%, can then be used as the second step of the proposed triage protocol.
In the cluster of various criteria used for the second step of our triage protocol, respiratory distress and direct contact with definite COVID-19 patients were chosen as subjective criteria associated with COVID-19. Combined with respiratory rate and O2 saturation as equivalent objective criteria for respiratory distress, these four criteria showed a significant difference in the group of positive RT-PCR patients compared with non-infected patients. Considering the existence of fever as one of the most common symptoms in studies of non-trauma patients with COVID-19, this criterion was also determined as the last criterion of the second stage in our novel triage system. Evaluation of RT-PCR positive trauma patients with at least two out of five of the above mentioned criteria showed that the prevalence of typical manifestations of COVID-19 in chest CT scans of patients with a positive RT-PCR test was higher than non-infected individuals. Therefore, further investigation is recommended in the above-noted patients based on the pathway shown in figure 1. The evaluation of patients admitted to the special ward of COVID-19 showed that 30% of patients with definite COVID-19 will be identified at this stage if the novel protocol is implemented. It should be noted that this step can be performed in <1 hour in trauma patients (table 4).
Frequency of positive clinical and laboratory findings in suspected patients (n=130)
Considering the importance of asymptomatic carriers of COVID-19 in the spread of the disease and the prevalence of 33.3% of these patients in this study, all asymptomatic individuals with positive RT-PCR tests were evaluated to select appropriate criteria for triage in the shortest possible time. Evaluation of on-arrival laboratory tests in asymptomatic carriers showed that 100% of them had an increase in CRP blood level, 70% had leukocytosis, and 50% developed lymphopenia or an abnormal erythrocyte sedimentation rate. Also, according to studies on the role of a chest CT scan in the early diagnosis of asymptomatic carriers compared with COVID-19 definite diagnostic tests in non-trauma patients, the evaluation of patients with criteria determined in the third step of the novel triage system is also performed by CT scan. Therefore, to triage asymptomatic carriers in less than an hour, we recommend using the above tests on patients’ arrival as step 3 of our novel triage system.
The evaluation of patients with a positive RT-PCR test showed that 86.7% of patients with positive RT-PCR test results would be identified in the first three steps of our proposed triage protocol within 1 hour.
Considering the possibility of asymptomatic carriers, the existence of patients in the pre-symptomatic stage of the disease, and the likelihood of COVID-19 infection due to hospital contact, we recommend triaging other patients, who were not included in the first three steps, according to the fourth step of our triage protocol. Furthermore, considering the high possibility of direct contact with asymptomatic carriers following nursing care in patients admitted to ICUs, evaluating all patients at the ICU admission by RT-PCR test is recommended in this step.
Overall, our data indicate that the proposed novel triage system described in this study can help physicians detect the most suspicious and definite COVID-19 cases with this stepwise system in less than an hour. This approach significantly decreases the time to diagnosis, leading to a reduction in non-protected exposure between suspected and healthy patients and medical staff, and decreasing the risk of COVID-19 spread. The implementation of this triage protocol detected 28 COVID-19 positive patients (93.3%) during the first hour of hospital admission, which reduced the risk of cross-infection to our medical staff and other patients. This triage protocol also detected two asymptomatic COVID-19 positive patients on arrival with normal laboratory findings. They were detected on ICU admission after orthopedic surgery.
Among other triage protocols for the general patient population, the WHO protocol had the most specific definition for suspicious individuals (100%), but it showed low sensitivity (13.3%). ECDC was the most sensitive protocol, which showed 93.3% sensitivity and 89.5% specificity, but did not prioritize patients based on trauma and their unstable condition. Instead, our pathway focused on managing trauma patients and detecting suspicious cases limiting disease transmission in the shortest period.
To the best of our knowledge, few studies have been conducted to design a stepwise pathway to manage trauma patients during the pandemic. Porcel et al recommended evaluating all patients with the RT-PCR test to find asymptomatic, positive cases in trauma patients with low-energy fractures.20 As mentioned above, we (and other low- and middle-income countries) cannot run this system due to our limitations.
Our study had some limitations. In addition to its small sample size, it was conducted in a single trauma center. Therefore, other studies must be conducted with larger sample sizes in various trauma centers to help further strengthen and refine this proposed triage system. However, despite its limitation, our new triage system was advantageous in detecting most of the COVID-19 positive patients in the first stage, reducing the risk of COVID-19 transmission to both medical staff and other patients. Therefore, we believe that this proposed triage protocol can be used as a guide and help improve the triage systems in all trauma centers, particularly those with limited resources.
Data availability statement
Data are available upon reasonable request. No free text required.
Ethics statements
Ethics approval
This study was approved by the Institutional Review Board of Shiraz University of Medical Sciences with Ethical Code: IR.SUMS.REC.1399061.
Acknowledgments
We thank our colleagues from the emergency room of Rajaee Hospital who provided insight and expertise that greatly assisted the research.
Footnotes
Contributors HAF: Conceptualization, methodology, writing-review & editing. RB: Methodology, formal analysis, investigation, writing - original draft. GS: Conceptualization, methodology, writing-review & editing. ZS: Conceptualization, methodology, formal analysis. SB: Writing-review & editing, methodology. HRA: Software, investigation, resources, supervision. SA: Methodology, writing-review & editing, formal analysis. MS: Methodology, formal analysis. SP: Methodology, writing-review & editing. ATA: Methodology, writing-review & editing. LS: Methodology, writing-review & editing, formal analysis. MZ: Methodology, writing-review & editing. SM-A: Conceptualization, methodology, supervision, validation, writing - original draft, writing-review & editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.