Article Text

Abstract
Objective We aimed to compare general surgery emergency (GSE) volume, demographics and disease severity before and during COVID-19.
Background Presentations to the emergency department (ED) for GSEs fell during the early COVID-19 pandemic. Barriers to accessing care may be heightened, especially for vulnerable populations, and patients delaying care raises public health concerns.
Methods We included adult patients with ED presentations for potential GSEs at a single quaternary-care hospital from January 2018 to August 2020. To compare GSE volumes in total and by subgroup, an interrupted time-series analysis was performed using the March shelter-in-place order as the start of the COVID-19 period. Bivariate analysis was used to compare demographics and disease severity.
Results 3255 patients (28/week) presented with potential GSEs before COVID-19, while 546 (23/week) presented during COVID-19. When shelter-in-place started, presentations fell by 8.7/week (31%) from the previous week (p<0.001), driven by decreases in peritonitis (β=−2.76, p=0.017) and gallbladder disease (β=−2.91, p=0.016). During COVID-19, patients were younger (54 vs 57, p=0.001), more often privately insured (44% vs 38%, p=0.044), and fewer required interpreters (12% vs 15%, p<0.001). Fewer patients presented with sepsis during the pandemic (15% vs 20%, p=0.009) and the average severity of illness decreased (p<0.001). Length of stay was shorter during the COVID-19 period (3.91 vs 5.50 days, p<0.001).
Conclusions GSE volumes and severity fell during the pandemic. Patients presenting during the pandemic were less likely to be elderly, publicly insured and have limited English proficiency, potentially exacerbating underlying health disparities and highlighting the need to improve care access for these patients.
Level of evidence III.
- COVID-19
- emergency treatment
- emergency medical services
- general surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
As cases of COVID-19 rose in the USA in early 2020, federal, state and local governments enacted interventions to quell the spread of the virus and preserve hospital capacity. Among these interventions was a widespread shift to virtual healthcare and cancellation of elective surgeries. Together with fear of acquiring COVID-19, this interruption in care prompted concerns about patients’ hesitancy to access emergent medical services, as seen previously. Most recently, the 2003 SARS epidemic led to significant reductions in utilization of services across healthcare settings due to fear of acquiring and stigma associated with SARS.1–3
Reports early in the pandemic suggested that non-COVID-19 medical and surgical emergencies fell, leading to widespread concern about patient barriers to seeking care and downstream effects on health.4–6 However, current healthcare utilization literature is largely limited to trends immediately following the onset of the COVID-19 pandemic and little is known about changes in volume, demographics and type of presentations for general surgical emergencies (GSEs).
Our institution, the University of California, San Francisco (UCSF) Medical Center, cancelled all elective surgical cases on March 13, 20207 and the City and County of San Francisco issued a shelter-in-place (SIP) order on March 16, 2020,8 specifying that adults aged 65+ years should isolate at home.9 In addition, San Francisco public transportation was significantly scaled back, onsite community clinics closed and lack of patient access to technology and provider training limited telehealth expansion. These barriers to accessing care may disproportionately impact vulnerable populations already at higher risk of COVID-19.10 These include patients who are older, have comorbidities, are from structurally disadvantaged racial and ethnic groups, have limited English proficiency and are uninsured/underinsured.11 12
In this study, we aimed to assess changes in GSE volume, patient demographics and illness severity of presentation during COVID-19 and to determine if particular groups were disproportionately affected.
Methods
All adults (aged ≥18 years) presenting to the emergency department (ED), regardless of ED disposition, for potential GSEs at a single tertiary-care hospital between January 2018 and August 2020 were included. Data were extracted from the UCSF electronic medical record (EMR) system. Defined by International Classification of Diseases-10 (ICD-10) code, we included gastric ulcer, duodenal ulcer, peptic ulcer, appendicitis, diverticular disease, other diseases of the intestine, peritonitis, cholelithiasis, cholecystitis and acute pancreatitis (Online supplemental file 1). Demographic variables included age, sex, race/ethnicity, interpreter use and payor, all variables included in our EMR. Proxy measures for disease severity included severity of illness (SOI) score,13 sepsis (based on ICD-10 code) and length of stay (LOS). The SOI index, whereby a severity score is assigned to each patient at discharge based on seven clinically relevant dimensions (including diagnosis, complications, concurrent conditions, among others), is the standard severity index tracked by our Medical Center. Other metrics measuring severity included white blood cell (WBC) count at presentation and maximum WBC in the first 24 hours of hospitalization.
Supplemental material
To compare GSE case volumes, an interrupted time-series (ITS) analysis was performed using segmented linear regression comparing the two time periods designated pre-COVID-19 (January 1, 2018–March 15, 2020) and during COVID-19 (March 16, 2020–August 31, 2020), using San Francisco’s March 16, 2020 SIP order as the start of the COVID-19 period. The Durbin-Watson statistic was used to test for autocorrelation of error terms in the regression model, with values <1 or >3 indicating concern. Each hospitalization encounter was treated independently in the analysis because the percentage of patients with more than one hospital encounter during the study period was below a previously accepted cut-off.14 We also completed ITS analyses on seven subgroups by disease process: ulcer, appendicitis, gallbladder disease, peritonitis, acute pancreatitis, diverticular disease and other diseases of the intestine. We used an ITS to examine changes in the percentage of patients whose GSEs were surgically managed in the two time periods. Bivariate analyses were used to compare patient demographic and disease severity characteristics before and during COVID-19, including t-tests for continuous variables and χ2 tests for categorical variables.
Data analysis was completed in SAS V.9.4 (SAS Institute, Cary, North Carolina, USA) and Stata V.16 (StataCorp, College Station, Texas, USA). P values of ≤0.05 were considered to be statistically significant.
Results
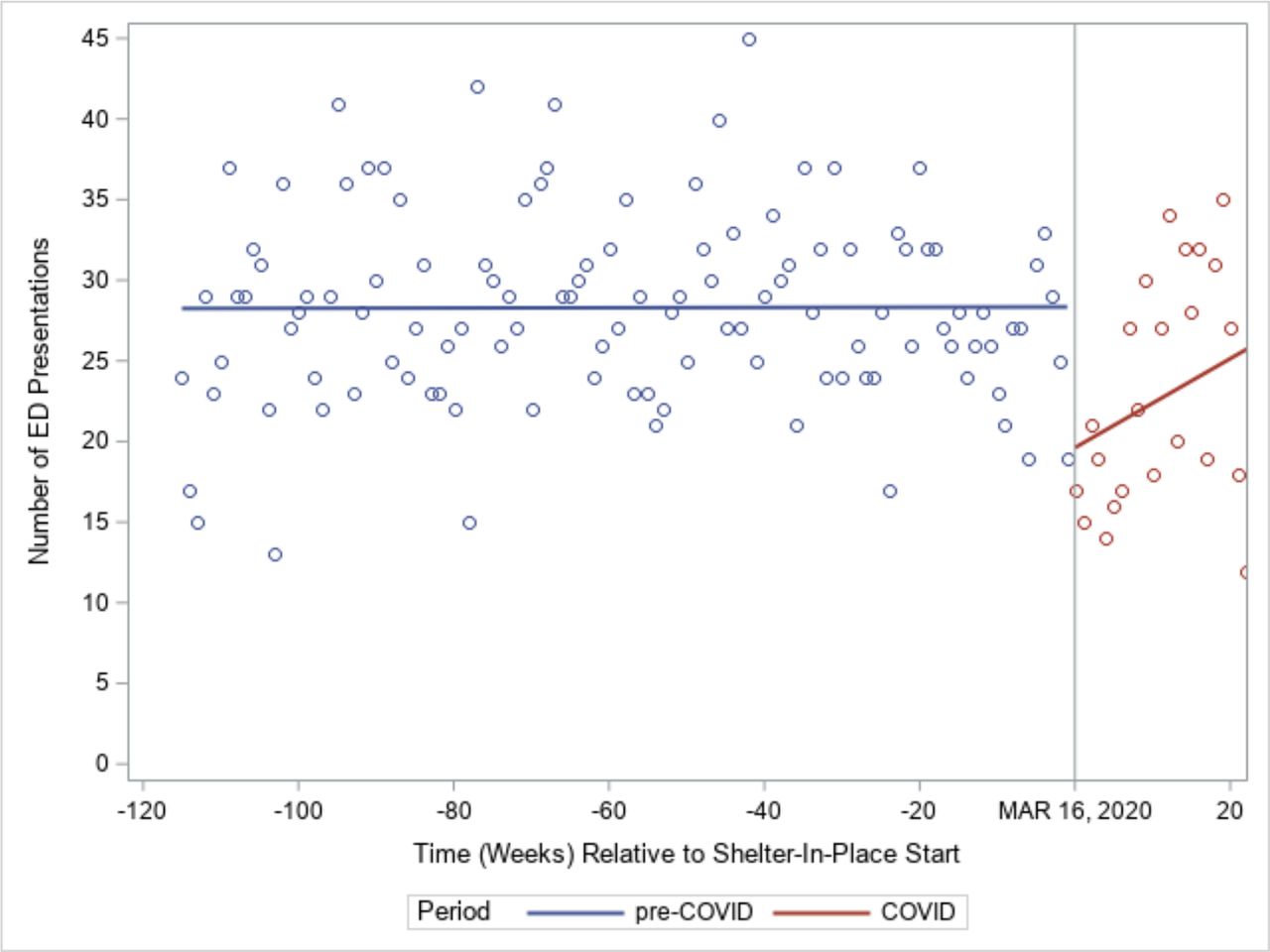
Pre-COVID-19, a total of 3255 patients (28/week) presented with potential GSEs (71% admitted), compared with during COVID-19, when 546 (23/week) presented (77% admitted). When SIP started, presentations fell by 8.7/week (31%) from the previous week (95% CI (−13.9 to –3.57), p<0.001) and subsequently increased towards pre-COVID-19 levels the following weeks.
However, the overall change in number of GSE presentations per week during COVID-19 was not significantly different from the change in number of GSE presentations per week pre-COVID-19 (difference in slopes=0.28, 95% CI (−0.07 to 0.62), p=0.12). Both time periods had non-significant positive slopes for change in the number of GSE presentations per week. Pre-COVID-19, the number GSE presentations increased by 0.0009 per week (95% CI (−0.03 to 0.03), p=0.96), and during COVID-19 the number of GSE presentations increased by about 0.28 per week (95% CI (−0.07 to 0.62), p=0.12) (figure 1). Correction for autocorrelation was not done as the Durbin-Watson test statistics did not indicate concern.

General surgery emergency presentation volumes before and during the COVID-19 pandemic. ED, emergency department.
The same analysis was performed on the seven subgroups of interest, with only the peritonitis and gallbladder disease subgroups having significant differences in number of presentations between the pre-COVID-19 and during COVID-19 time periods (online supplemental file 1). During the first week after the SIP order, the number of ED presentations in each of these two subgroups decreased by nearly three from the previous week (peritonitis: β=−2.76, 95% CI (−5.03 to –0.48), p=0.017; gallbladder disease: β=−2.91, 95% CI (−5.28 to –0.54), p=0.016). However, the change in the number of ED presentations per week (slope) during COVID-19 was not significantly different from the change in number of ED presentations per week pre-COVID-19 for either subgroup (figure 2A,B).
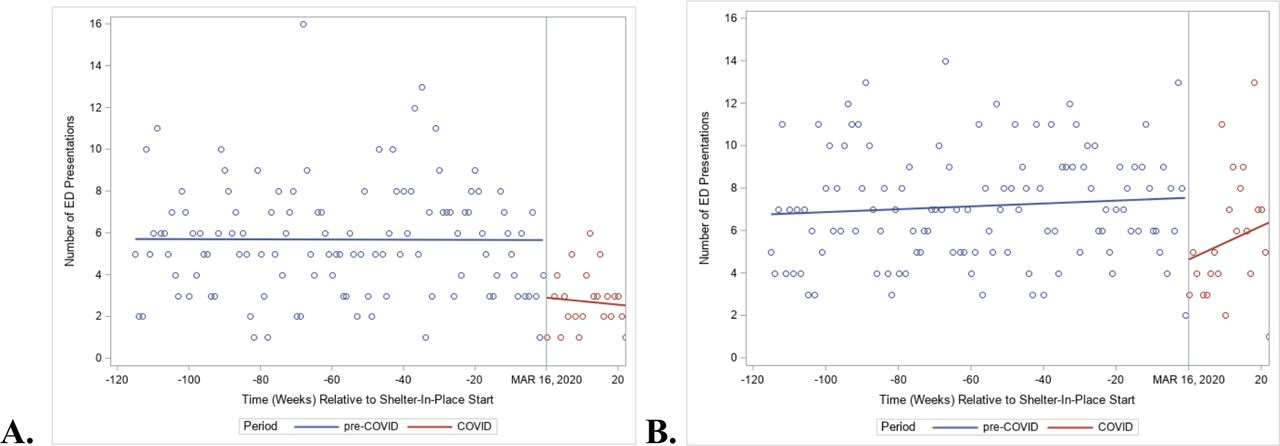
Peritonitis (A) and gallbladder disease (B) emergency department (ED) presentation volumes before and during the COVID-19 pandemic.
By demographic characteristics, the mean age pre-COVID-19 was 56.86 years, compared with 53.95 years during COVID-19 (p=0.001) (table 1). This was driven by a decrease in the proportion of patients aged 50–64 years (23% vs 28% pre-COVID-19) and 65+ years (34% vs 37% pre-COVID-19) and an increase in the proportion of patients aged 18–34 years (21% vs 15% pre-COVID-19). During COVID-19, patients were less likely to have public insurance (Medicare or Medicaid) and more likely to have private insurance (p=0.024). Among patients below the Medicare age cut-off of 65 years, the proportion who were publicly insured fell from 45% to 37% (p=0.005). During COVID-19, fewer patients required the use of an interpreter (12% vs 15% pre-COVID-19, p<0.001). There were no differences in GSE presentations by gender (p=0.058) or race/ethnicity (p=0.181) pre-COVID-19 and during COVID-19.
Demographic characteristics pre-COVID-19 and during COVID-19
The percentage of people who had surgery for their GSEs was 46% during COVID-19, compared with 52% pre-COVID-19 (p=0.007) (table 2), largely driven by a drop to 20% and 24% in the first and second week after SIP, respectively (β=−9.87, 95% CI (−18.6 to –1.15), p=0.027) (figure 3). In terms of illness severity, the lowest SOI group (minor) increased from 14% of the population pre-COVID-19 to 19% during COVID-19, and the highest SOI group (extreme) decreased from 30% to 20% (p<0.001). Fewer patients presented with sepsis during COVID-19 (15% vs 20% pre-COVID-19, p=0.009). After excluding high outliers with LOS >30 days, average LOS was 3.91 days during COVID-19 compared with 5.50 pre-COVID-19 (p<0.001). While during COVID-19 there was a decrease in WBC at presentation (10.8 vs 11.24 pre-COVID-19) and maximum WBC in the first 24 hours after presentation (11.37 vs 11.83 pre-COVID-19), differences were not statistically significant (p=0.225 and p=0.230, respectively).

{kind=link}
{kind=link}
{kind=link}
Percentage of patients with surgical intervention for general surgery emergency before and during the COVID-19 pandemic. ED, emergency department.
Disease severity metrics pre-COVID-19 and during COVID-19
Discussion
In this study, we investigated the change in volume and characteristics of GSEs during the COVID-19 pandemic. Our results show that the number of GSEs dropped drastically in the period immediately after the SIP order in San Francisco, but over time rebounded to rates closer to those pre-COVID-19. The largest drivers of this drop were generalized peritonitis and gallbladder disease. One possible explanation of the drop in volume is decreased number of ED presentations for postoperative complications due to the cancellation of elective surgeries. However, the timing of the drop preceded our institutions’ cancellation of elective surgery, thus is unlikely to be the primary factor. However, the drop in volume we saw at our institution is consistent with other studies, which found that patients stayed home rather than presenting to the hospital for multiple different medical and surgical conditions during COVID-19.5 6 15–19 Importantly, patients presenting after the SIP order were less likely to be elderly, publicly insured and have limited English proficiency, revealing a possible disparity in access to care in these groups.
We found that the rate of patients presenting with sepsis as well as the overall SOI score decreased during COVID-19. The progression of untreated GSEs typically includes fever, anorexia and pain, which generally prompts patients to present to an ED. We had hypothesized that during COVID-19 patients would delay presenting to the ED due to exposure concern, and would thus present at a later, more severe stage of disease. However, contrary to our expectations, we found that average severity of patients presenting with GSEs actually decreased. These findings prompt concern that the most critically ill patients may be dying at home of surgical disease during COVID-19. This may be related to SIP messaging targeted at older adults, who already have lower reserve and may be less resilient to delays in care. This possibility has been raised in other disease processes, such as heart failure or myocardial infarction, and is supported by the declining volumes and reduced average severity of patients who present to the ED.
We were similarly surprised that average LOS decreased during COVID-19. We speculate three drivers. First, shorter LOS is consistent with our finding of decreased illness severity. Second, our organization’s shift towards non-operative antibiotic management early in the pandemic, when the risks of laparoscopic surgery were not fully understood, may have contributed to shorter hospitalizations. Finally, cancellation of elective cases at our institution may have allowed for more timely operative intervention for those who warranted it, resulting in an overall LOS.
Understanding which populations are facing increased barriers to care and targeting public health messaging for these groups is especially critical as COVID-19 persists. The fact that the proportion of younger, English-speaking and privately insured patients at presentation is significantly higher during COVID-19 raises concern that older, non-English speaking and publicly insured adults are disproportionately affected. While the transition to telemedicine has increased access to care for many patients, challenges in the rapid scaling of telehealth services may have inequitably impacted already vulnerable populations, including those with less access to technology or technological literacy.20 This is critical knowledge in order to target public service announcements to older adults and ensure that information is distributed in non-English languages. Notably, we saw a decreased proportion of patients needing an interpreter during COVID-19, while no difference in race/ethnicity was observed. This is likely driven by the sizeable number of patients from the Middle East and Eastern Europe that our medical center serves. These patients may not be proficient in English but would be classified as ‘white or Caucasian’, underscoring the importance to consider a broad spectrum of languages.
Additionally, older patients may require increased outreach and support in the use of telehealth platforms so they can seek advice on whether to present to a hospital. Increased focus on restoring access to care in these groups is important across healthcare settings, not only in GSEs, as the COVID-19 pandemic persists and SIP orders continue. Our findings suggest that these groups should be specifically targeted in public health messaging related to stay-at-home orders and outreach efforts around vaccination. Furthermore, while COVID-19 has highlighted these disparities in the context of a public health crisis, these groups may continue to be vulnerable to future social and economic events.
A limitation of this study is that it is a single-center investigation, thus limiting our ability to understand ED presentations to outside hospitals. However, UCSF Medical Center is the largest and busiest hospital in San Francisco and third in California, thus reaching a large proportion of patients from our region. Second, the San Francisco SIP order was announced early and the city was less impacted by COVID-19 relative to other geographies, which may limit the generalizability of our findings. However, at the onset of SIP, the trajectory that COVID-19 would take in our region was unknown; thus, fear of the disease, and insufficient messaging and access to telehealth to overcome it, rather than the severity of the COVID-19 outbreak itself, may still drive significant changes in patient behavior. Future research should aim to examine region-wide trends in ED presentations (eg, using a statewide database) to confirm differences in presentation for underserved communities; investigate whether the onset of COVID-19 impacted causes of death outside the hospital to understand if patients with serious GSEs died at home; and develop infrastructure to increase hospital and telemedicine access for vulnerable populations, especially older adults, as the pandemic continues.
Conclusion
The number of patients presenting with GSEs fell at the onset of COVID-19. This significant drop, together with the fact that average severity at presentation decreased, raises the possibility that critically ill individuals died at home rather than presenting to a hospital. The disproportionate drop in older, publicly insured and non-English-speaking patients suggests that COVID-19 is potentially exacerbating underlying health disparities. Further work should be done to develop outreach strategies for vulnerable communities, increase telehealth access and investigate potential deaths at home.
Acknowledgments
The authors would like to thank Yumiko Abe-Jones and the Division of Hospital Medicine for their support and collaboration in developing this project and acquiring data; Amy Shui, MA and the Department of Surgery Biostatistics Core for her biostatistical and data visualization expertise; and acute care surgeons from UCSF and across the nation who continued to provide high-quality care for patients in the face of fear and uncertainty. Publication made possible in part by support from the UCSF Open Access Publishing Fund.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ALG and HS are joint first authors.
Contributors ALG and HS should be considered co-first authors, as they both equally contributed to study conception and design; acquisition of data; data analysis and interpretation and drafting and revising the manuscript. CRC and YMK assisted with study conception and design; data interpretation and revision of the manuscript. RM, MM and JPR served as senior advisors to the study team for study conception and design; data interpretation and manuscript revision. The senior author for this manuscript, TB, provided guidance on study conception and design; ongoing oversight over the group’s work in acquiring, analyzing and interpreting the data, and editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
Competing interests TB is funded by the Agency for Healthcare Research and Quality (AHRQ) (K12HS026383). JPR receives funding from Merck & Co. for unrelated research.
Patient consent for publication Not required.
Ethics approval This study was approved by the UCSF IRB.
Provenance and peer review Not commissioned; externally peer reviewed.