Article Text

Abstract
The covid-19 global pandemic due to the SARS-CoV2 (CoV2) virus has created the need to adapt hospital workspaces and staffing models, and trauma is no exception. While the optimal configuration of a trauma resuscitation area is debatable, the space needs to be large enough to accommodate the trauma team and ancillary staff. It also needs to have ready access to supplies and equipment to quickly and easily control hemorrhage, secure an airway and initiate fluid resuscitation. Lastly, stores of personal protective equipment in the form of fluid resistant gowns, head covering, face shield, and gloves (both sterile and non-sterile) should be readily available but under strict access. As CoV2 carriers increased in our population in New Jersey, we treated each incoming trauma patient as a potentially CoV2-positive case and sought to reconfigure out trauma resuscitation area to minimize exposure of our supplies to aerosolized virus.
- disasters
- body fluids
- emergency treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
During the 2020 covid-19 pandemic, the trauma bay is definitely a potentially contaminated area. With the surge of CoV2-positive patients into our trauma catchment area, we have noted a substantial number of asymptomatic trauma patients that mandated that all trauma patients be considered potentially positive. Trauma resuscitation bays must accommodate three key components: staff, supplies needed for immediate control of hemorrhage and resuscitation, and personal protective equipment (PPE).1 2 Unfortunately, supplies and equipment kept out and readily available, results in them being contamination by aerosolized virus. With this in mind, we reconfigured our trauma resuscitation area with the following goals in mind: (1) maintaining protection of staff without excessive use of PPE, (2) maintaining easy accessibility of supplies and equipment without contaminating stores and (3) limiting traffic in and out of the ‘hot zone’ of potential CoV2 exposure. The following describes our approach to the trauma patient during the covid-19 pandemic.
Personal protective equipment
The 10th addition of the Advanced Trauma Life Support (ATLS) states ‘Due to concerns about communicable diseases… the Centers for Disease Control and Prevention (CDC)… strongly recommend the use of standard precautions (eg, face mask, eye protection, water-impervious gown, and gloves) when coming into contact with body fluids. The ACS COT considers these to be minimum precautions and protection for all healthcare providers’. With PPE in short supply, there is also a necessity to shepherd this resource and having everyone gown up is simply not possible. Doffing PPE is a high-risk activity that needs to be done carefully, correctly and best performed under supervision.
Trauma bay
All supplies were removed from the storage shelves with the only equipment remaining are the stretcher, monitor unit and Mayo stand (figures 1 and 2). The routine equipment carts were moved well away from the trauma bay. The trauma bay and resuscitation area were divided into hot, warm and cold zones (figure 3) in accordance with Environmental Protection Agency (EPA) Hazmat practices.3 The hot zone was the area directly around the patient. The limit of the hot zone was marked using red duct tape to ensure a clear visual signal. Everything on the patient side of the red tape was considered potentially contaminated. Three feet from the hot zone was the warm zone and marked with yellow duct tape. This represents an area of lower potential contamination. In this area, we placed an operating room (OR) back table. This table was our ‘transfer station’ where we placed supplies from the cold zone to the hot zone to be used by the trauma team (figure 4). Mask, gloves and head covering was mandatory, but full and more stringent PPE was advised depending on the severity of the trauma and potential for contamination. This is the zone that the personnel who were in the hot zone doffed their PPE. The cold zone was outside the yellow tape and was where all supplies and persons not involved in the resuscitation were staged (figures 5 and 6). The team leader could easily direct the trauma resuscitation from this zone.
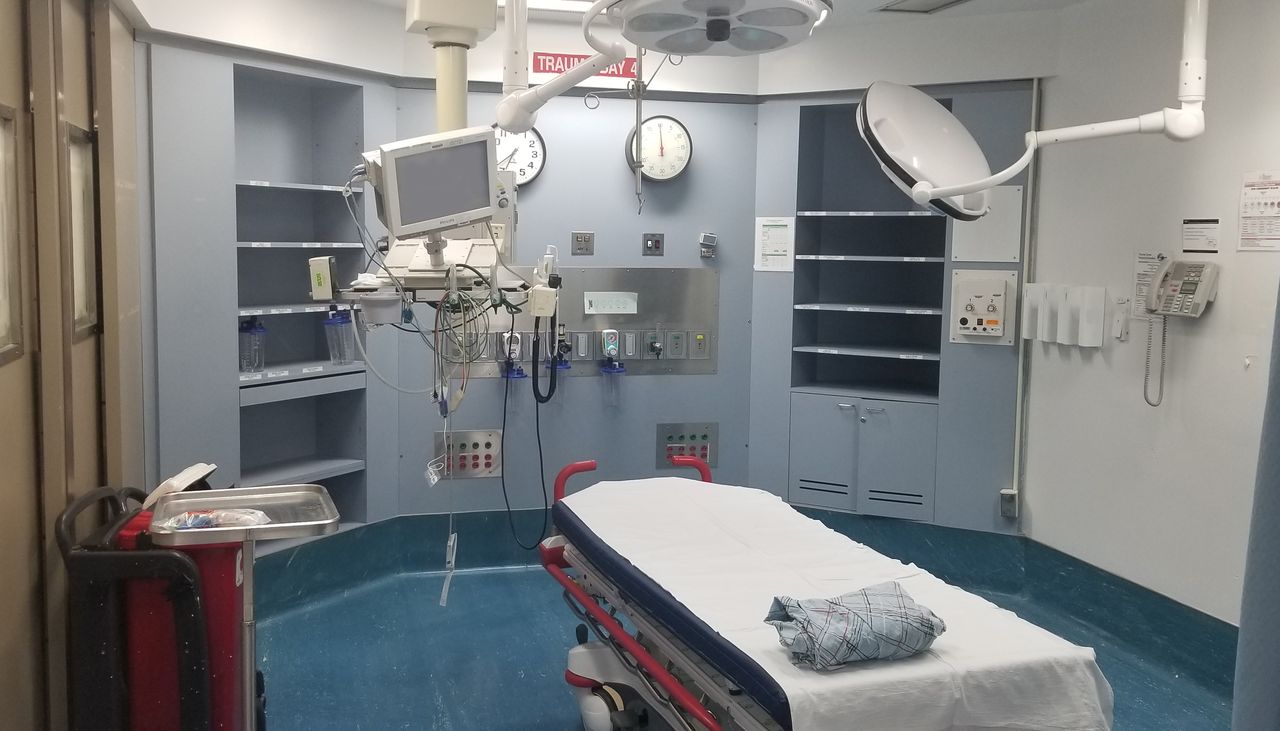
Individual trauma bay after removing all supplies from shelves and equipment. Mayo stand with single patient supplies in lieu of standard nursing cart.

Trauma resuscitation area with clearly delineated hot (red tape), warm (yellow tape) and cold zones. Transfer table is present in the warm zone with all other easily accessible supplies in the cold area.
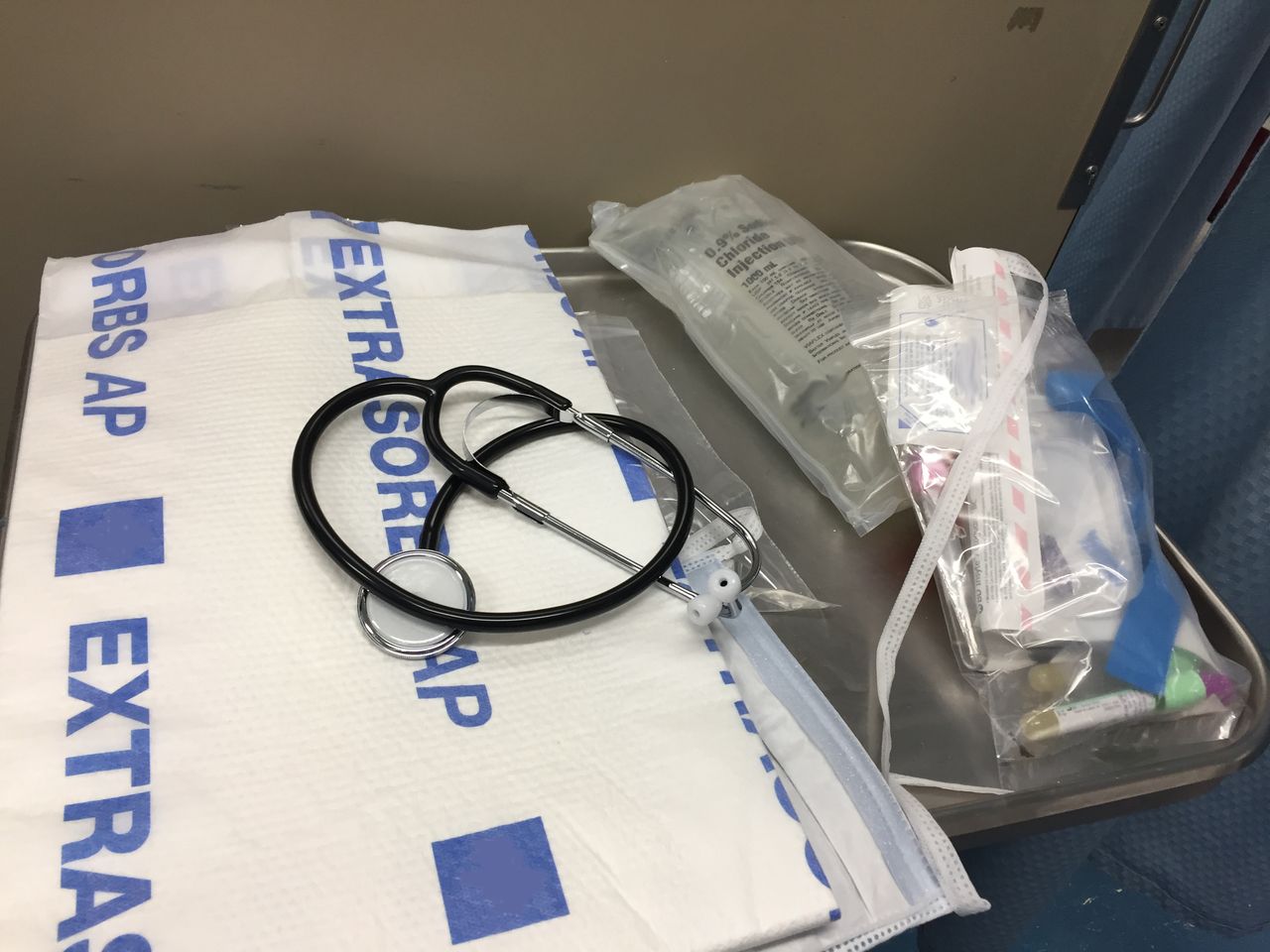
Close up of the supplies for stationed for each case. Individually bagged intravenous and phlebotomy tubes, extra masks for patient, underbody absorbent pad and disposable stethoscope.

Trauma team awaiting level 1 activations, multiple gunshot wounds. Due to potential severity of activation, team consists of chief and midlevel trauma residents, a senior emergency medicine resident and trauma nurse. Trauma attending staff is present in the cold zone as team leader and readily available but not gowned and gloved to conserve PPE. Equipment carts (A)) at each end of the trauma resuscitation area. The main supply (red arrow), PPE carts (purple P) and airway cart (not visualized) are kept centrally.

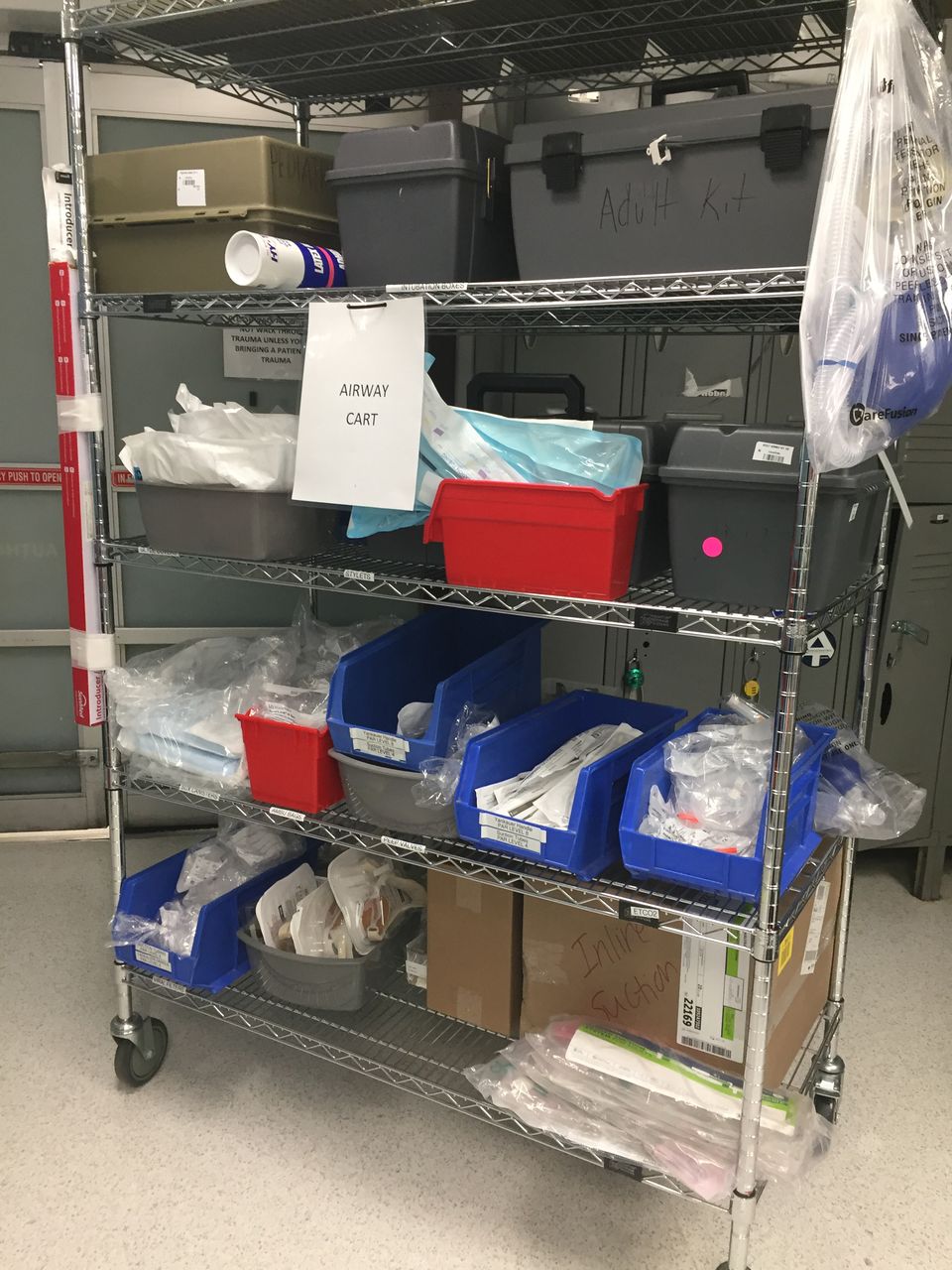
Dedicated airway cart.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
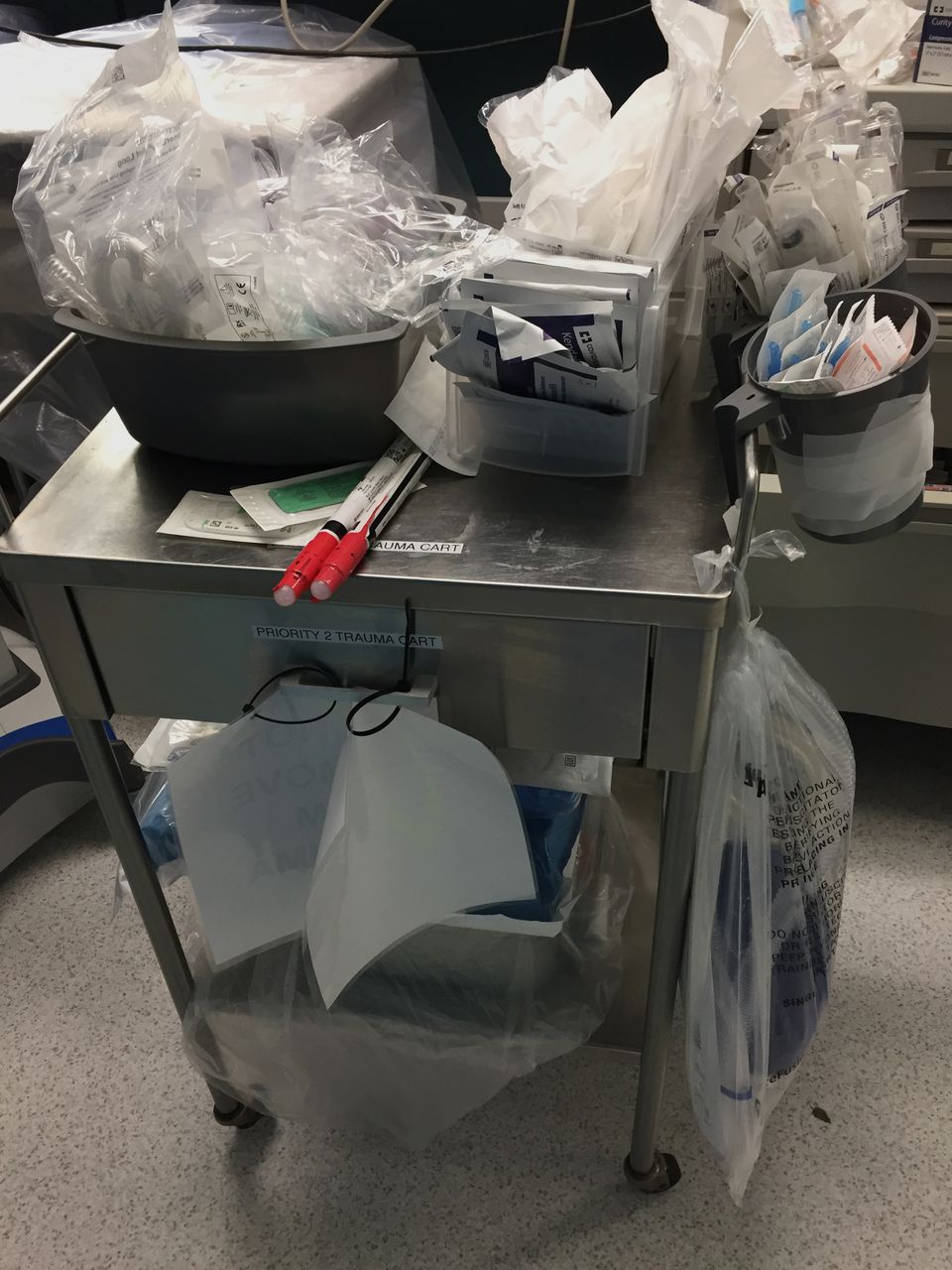
Equipment cart with tube thoracotomy supplies, syringes, commonly used sutures, suction tubing and procedure tray (bottom shelf). These small portable carts allow easy access to resuscitations supplies to be passed into the hot zone.
Personnel
Trauma nursing and physicians would appropriately don PPE. As PPE was in short supply, the team leader/attending surgeon dictated the number of people involved in the hands-on resuscitation. For example, in hemodynamically stable level 2 activation, this was often a single resident and the nurse. An ED tech or aide was used to pass supplies or instruments to the hot zone. Depending on how the trauma evaluation evolved, the team could be flexed up or down based on needs with overarching principle to limit exposing providers
Supplies
Early in our experience, we realized we had removed easy access to all of our supplies making resuscitations problematic. We then placed intravenous, fluid, and blood collections tubes in large plastic bags for each resuscitation. A small procedure cart was stocked with chest tubes and procedure trays. These could be easily brought up to the warm zone and needed equipment put on the transfer table and used by the resuscitation team. All other supplies were on our standard carts in the cold zone.
Radiology
The trauma ultrasound probe is covered with a plastic bag to decrease contamination. A lead/plexiglass barrier was brought from the OR to allow the trauma team to remain in the hot zone when obtaining X-rays.
PPE
As noted by many, supplies of PPE have been limited during this pandemic, especially impervious gowns, N95 and surgical masks as well as cleaning supplies. PPE in limited numbers were placed in a dedicated cart in our trauma resuscitation area under the watchful eye of the trauma nurses and attending physicians. This approach reduced waste and pilferage.
In summary, this reconfiguration of the trauma bay for the covid-19 pandemic has maintained the ability to resuscitate severely injured trauma patients without unnecessarily exposing personal and supplies. While each trauma program will need to adapt based on the geography of their trauma resuscitation area and patient population, we strongly endorse the concept of a hot, warm and cold zone as described by the EPA with a station to move medications and supplies into the hot zone as the optimal way to conduct trauma resuscitations during this pandemic.
Footnotes
Contributors All authors participated in the planning of the project and editing of the document.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.