Article Text

Abstract
Many patients with blunt splenic injury are considered for nonoperative management and, with proper selection, the success rate is high. This paper aims to provide an update on the treatments and dilemmas of nonoperative management of splenic injuries in adults and to offer suggestions that may improve both consensus and patient outcomes.
- Spleen injuries
- angiography
- salvage
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Each year in the United States approximately 1.5 million adults suffer blunt injury with almost 40 000 suffering a splenic injury.1 Based on recent studies, as well as data from the American College of Surgeons National Trauma Data Bank, 10% to 15% of patients admitted with blunt splenic injury will undergo an urgent splenectomy within six hours of admission, primarily due to ongoing bleeding and hemorrhagic shock.2 The remaining patients with blunt splenic injury are considered for nonoperative management and most of them are successfully managed in this manner.
The nonoperative management of blunt splenic injury has evolved over decades and includes multiple disciplines. Careful patient selection for nonoperative management should result in high rates of overall splenic salvage. But the decision matrix and patient outcomes are not quite that predictable. Several treatment choices, including selective or main artery angioembolization, repeat CT scan, and/or continued observation, have resulted in variations in clinical practice. None of these options has proven definitive for splenic hemostasis and/or salvage.3–5 The aim of this paper is to address dilemmas in decision-making and suggest some principles that may bring consensus to the care of these patients and hence improve patient outcomes.
Spleen anatomy and its relationship to splenic salvage
To understand the development of the modern protocols for the management of blunt splenic injury, it is important to review the relevant splenic anatomy and physiology. The spleen has three to seven segments, each with its own vascular supply but separated by avascular planes. The splenic artery arises from the celiac axis and divides into the superior (larger) and inferior (smaller) branches, which further divide into segmental arteries to supply the splenic parenchyma. An understanding of the segmental blood supply is essential as it may play a role in splenic salvage. Lacerations parallel to the segmental vessels typically result in minimal hemorrhage, whereas those perpendicular to the segmental vessels cause more significant hemorrhage.6 7 Also, the characteristics of the splenic capsule may contribute to injury tolerance as it varies in thickness throughout the organ. Thicker splenic capsules, such as those in children, are more tolerant of damage and hence potentially contribute to a greater success rate of nonoperative management in the injured pediatric patient.7
Immune function of the spleen
The spleen plays a critical role in immune function. It filters encapsulated, poorly opsonized bacteria, produces opsonins, properdin, and tuftsin, destroys senescent or malformed erythrocytes, and removes inclusion bodies. It also processes and clears antigens, produces antibodies, and forms and stores blood cells. As early as 1951, the association between the spleen and immune function was recognized by Gruber and colleagues, who described overwhelming sepsis after splenectomy in an infant treated for idiopathic thrombocytopenic purpura.8 Subsequent reports solidified the role of the spleen as an organ with immune capability.9 10 Zarrabbi reported cases of 47 adults who developed serious infections after splenectomy for trauma.11 Two important findings from this study included the following: (1) although most of the cases of serious infection occurred during the first decade after splenectomy, some were documented as far out as three decades; and (2) most of the cases occurred in the young, potentially indicating that they are particularly vulnerable to sepsis after splenectomy.
The evolution of nonoperative management of the spleen
An accumulating bank of knowledge supported the important immunological role of the spleen and, by association, the importance of splenic salvage. In order for nonoperative management to be widely practiced, a better way to assess the severity of the splenic injury was required. In 1979, Drs. Hounsfield and Cormack shared the Nobel Prize in Medicine for the development of the CT scanner.12 Eventually, the resolution and speed of the CT scanner improved allowing for better assessment of intra-abdominal organs. These technological improvements provided a major step toward nonoperative management of solid organ injuries. Other CT scan advancements included the ability to visualize the organ in axial, coronal, and sagittal views to analyze the depth and extent of parenchymal injury, as well as the extent and activity of intraparenchymal and extraparenchymal vascular abnormalities. All of these advancements contributed to further characterization of splenic injuries and the use of that information for patient management.
Splenic injury grades and nonoperative management
In 1989, the American Association for the Surgery of Trauma (AAST) developed a splenic injury grading system as an aid to better characterize the injured spleen, providing consistency in describing organ injury and allowing its use as a guide in patient management (table 1).13 14
Adaptation of AAST Organ Injury Scale for Spleen
A subsequent revision of the grading system recommended advancing one grade of injury, up to grade III, if the patient had an additional solid organ injury. Grades I and II splenic injuries are considered low grade and grades IV and V are high grade. As per the revised scale, grade III injuries are usually grouped with the higher-grade injuries, especially if the patient sustains a concomitant solid organ injury. Another version of the splenic grading system was proposed by Marmery to better characterize splenic injuries with distinct vascular abnormalities as visualized on the CT scan.15 This grading system differentiates active intraparenchymal and subcapsular splenic bleeding, the presence of a pseudoaneurysm or arteriovenous fistula, and active intraperitoneal bleeding. The authors concluded that these distinctions improved their ability to better determine which patients with blunt splenic injury need angioembolization or another intervention.
Risk factors for the failure of nonoperative management
It is well accepted that the presence of hemodynamic stability and the absence of peritonitis are important factors in the proper selection of patients for nonoperative management. In the multicenter study from the Eastern Association for the Surgery of Trauma, Peitzman and colleagues found that all causes of mortality significantly increased from 4%, for patients whose spleens were successfully managed nonoperatively, to 16.5%, for those who failed nonoperative management.16 Similarly, Olthof’s Delphi study showed a consensus on the need for hemodynamic stability as a core factor for successful nonoperative management.17 They also agreed on the principle that hemodynamic instability (which they defined as a blood pressure <90 mm Hg and heart rate >130 beats per minute) of the patient was a clear indication for operation. But these are not the only factors that contribute to the success of nonoperative management. The age of the patient, grade of splenic injury, presence/quantity of hemoperitoneum, concomitant solid organ injury, and the presence of splenic vascular abnormalities or pseudoaneurysms complicate the decision matrix and make successful nonoperative management less predictable.4 16 18–20 Hence, once a hemodynamically stable patient without an overt indication for operation is deemed to be a good risk for nonoperative management, the surgeon’s challenge is to determine the best management for the patient so as to minimize failure and maximize the opportunity for splenic salvage. Each of these factors deserves discussion as none has been shown to consistently predict success or failure of nonoperative management.
Age
In 1996, Godley et al studied patients who underwent nonoperative management of the spleen for blunt trauma and they found that 10 of the 11 patients who were >55 years of age failed nonoperative management. Hence, they concluded that nonoperative management was contraindicated in this age group especially as the older patients had more complications than their younger counterparts.21 These results were similar to those of Bee, who found higher failure rates (11%) in patients >55 years of age versus only 7% in those patients who were <55 years of age.22 But several other studies have shown that nonoperative management of splenic injury in patients >55 years of age is safe and the patient outcomes are equivalent to those who are much younger. For example, Barone and colleagues studied 33 patients (mean age, 72±10 years) who were divided into two groups, 10 patients who underwent immediate exploration and 23 patients who underwent observation.23 Although observation of patients with blunt splenic injury failed in four of the 23 patients, there were no patient deaths related to the method of management of the splenic injury and hence they concluded that the failure rate of 17% was acceptable. Another study that supports the success of nonoperative management of splenic injury in this age group is Cocanour’s retrospective review of 375 patients over a five-year period.24 Of those patients, 29 were >55 years of age and they had higher Injury Severity Scores (ISS) and mortality rates (ISS, 29.3±2.6 vs. 19.5±2.1; mortality: 67% vs. 4%) than those patients who were <55 years of age. Although mortality rates were higher in the older patients, no deaths were attributed to the splenic injury. The authors concluded that although the older adults had more severe injuries, they had similar failure rates of nonoperative management compared with those of younger adults and, because the splenic injuries were not the direct causes of the mortalities, nonoperative management should not be contraindicated in this group. Harbrecht investigated the combination of older age and higher grade of injury and found a higher mortality rate compared with younger patients, thus making the failure rates in those patients >55 years of age 2.5 times as great as that for those <55 years of age.25 Although there is support for both points of view regarding nonoperative management and age, extra caution should be applied for older patients with comorbidities and those taking antiplatelet medications.
Grade of injury and the quantity of hemoperitoneum
Several studies have shown that high-grade injuries or large amounts of hemoperitoneum are associated with higher failure rates of nonoperative management of the spleen.16 26–28 This is not unexpected as the higher-grade injuries usually bleed more and hence are associated with larger amounts of hemoperitoneum. In an effort to add more precision to the relationship between the quantity of blood estimated on the CT scan and the failure rates of nonoperative splenic management, Federle et al determined that moderate (250 mL to 500 mL) to large (>500 mL) amounts of hemoperitoneum were associated with increased failure rates of nonoperative management.29 Although not a consistently predictable factor for determining the failure rate of nonoperative management, the quantity of hemoperitoneum is frequently cited as an important determinant.17 30
Concomitant solid organ injury
It seems intuitive that when multiple solid organs are injured, the rate of failure for nonoperative management increases. Data demonstrating this relationship are from a study conducted by Malhotra and colleagues, who examined 163 patients with blunt injuries to both the liver and the spleen.31 These patients had higher ISS, higher admission lactate levels, and lower admission systolic blood pressures than their 1125 cohorts who sustained a single solid organ injury. Other comparisons between the groups showed that the patients with multiple injured organs had worse outcomes having higher failure rates (11.6% vs. 5.8%) of nonoperative management, greater transfusion requirements, and higher mortality rates. The authors cautioned that extra vigilance is needed when choosing nonoperative management for patients with multiple solid organ injuries.
Vascular abnormalities
Splenic vascular abnormalities may be considered contrast blushes, pseudoaneurysms, or arteriovenous fistulae, and all have been associated with increased failure rates of nonoperative management.3 32–36 The presence, number, and size of these vascular abnormalities make a difference in splenic outcomes as reports indicate an 11% to 40% greater failure rate compared with those injured spleens without such abnormalities. For this reason, most experts agree splenic artery embolization is indicated for patients with blunt splenic injury and a vascular abnormality on the admission CT scan.
Angioembolization: pros and cons
The higher rate of nonoperative failure for injured spleens with vascular abnormalities has prompted an aggressive pursuit for the early diagnosis and treatment of vascular abnormalities. One of the earliest reports examining the role of angioembolization in patients with splenic injuries was a case series from Kings County Hospital Center in New York City.37 Using a variety of materials to embolize the splenic vessels, the authors were able to curtail splenic bleeding and, based on these successes, they began to collect data on subsequent patients with injured spleens. Several years later, the authors published the results of 60 patients undergoing angioembolization for blunt splenic injury with a 93% success rate for hemorrhage control and improved splenic salvage rates.33
Angioembolization is both a diagnostic and therapeutic intervention as it is effective in verifying the presence of a vascular abnormality and selectively embolizing its associated vessel to improve splenic salvage. In general, angioembolization is indicated for the termination of bleeding from intraparenchymal or extraparenchymal splenic blushes. When the presence of an actively bleeding vessel or ‘blush’ is noted on the initial CT scan, it is associated with more than a 20-fold increased risk of splenectomy.2
Although angioembolization is indicated for defined vascular abnormalities present on the initial CT scan, it may also be considered for higher-grade splenic injuries even when there is no obvious vascular abnormality identified.2 30 34 35 38 39 Differences in the timing of the arterial contrast bolus may influence the visibility of these abnormalities on the CT scan. Some surgeons recommend that patients who sustain higher-grade splenic injuries should undergo angiography after the initial CT scan to identify any latent vascular abnormalities.5 36 39 Although lower-grade splenic injuries may contain several vascular abnormalities, Haan et al showed that the use of routine angioembolization to detect latent vascular abnormalities in these patients resulted in a low yield and hence were unnecessary procedures.40 Studies like these have helped to focus the routine use of angiography for those patients with high-grade splenic injuries as failure rates for nonoperative management decreased.38 39
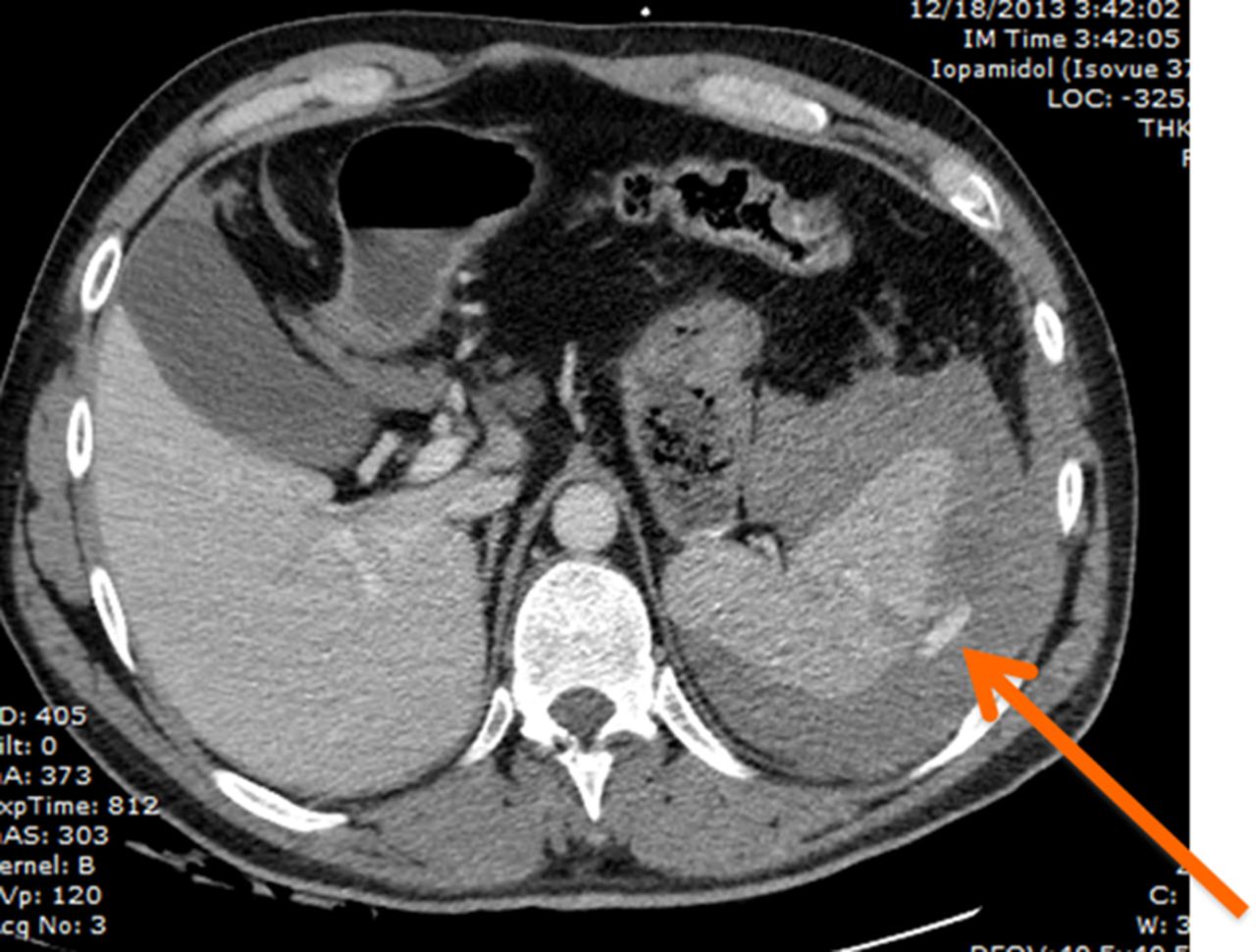
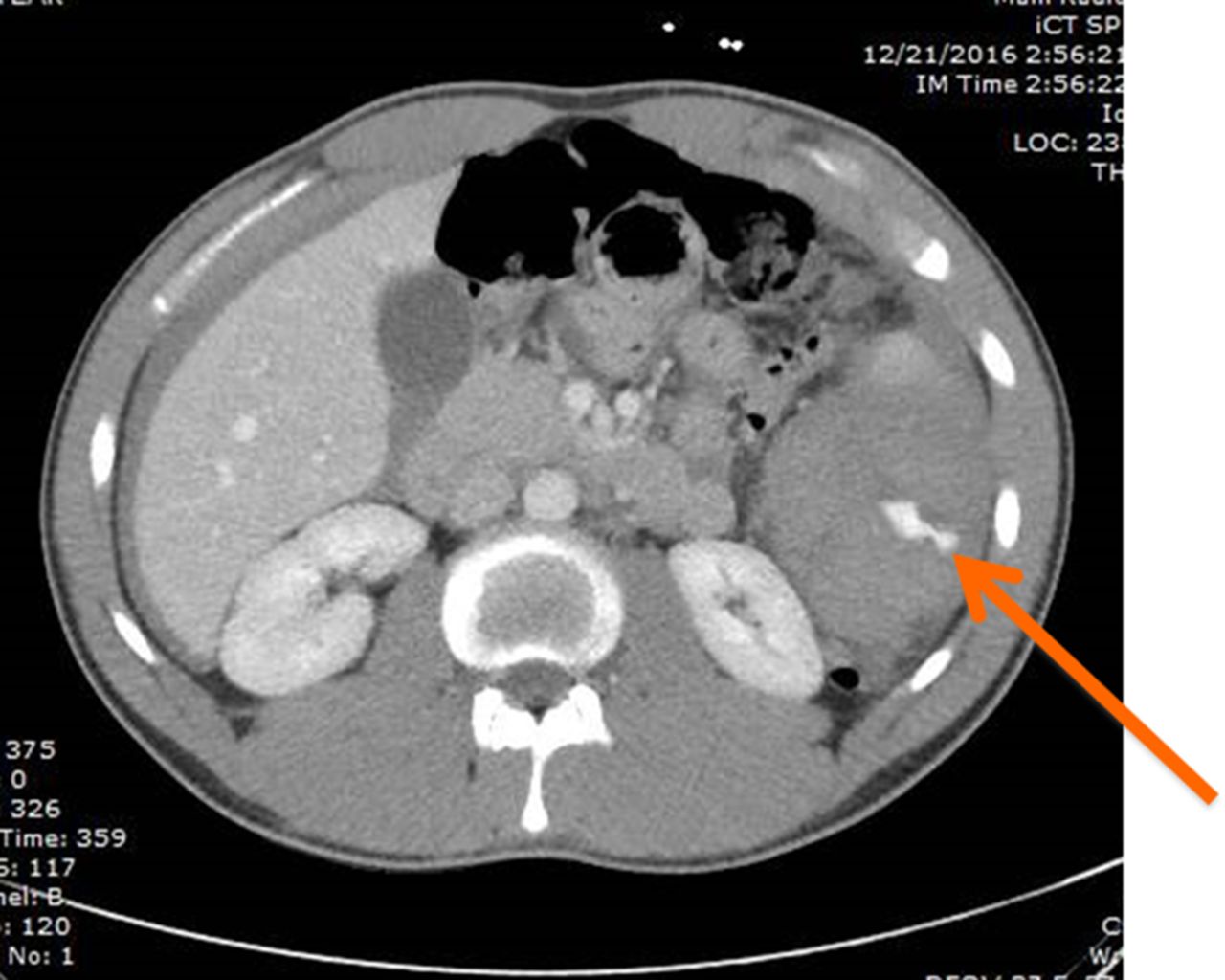
Despite the evidence to support angiography for high-grade splenic injuries, the adaptation of such protocols to do so remains controversial. A survey of 260 members of the AAST showed that only 25% thought that grades IV and V splenic injuries should undergo mandatory angiography.41 The hesitancy to adopt strict angiography protocols may be based on studies that have shown no consistent improvement in patient outcomes after angiography was performed, even for high-grade splenic injuries.4 35 39 40 42 Further, angioembolization has some drawbacks including (1) despite selective or main artery splenic angioembolization, the spleen can bleed, indicating that the procedure does not ensure splenic salvage (figures 1–3); (2) angiography may not identify a vascular abnormality that was seen on CT scan, hence making selective angioembolization challenging; and (3) despite selective angioembolization of a segmental artery, vascular abnormalities not related to that segmental artery may arise and splenic bleeding may occur at a later time42 43 (figures 4 and 5). Haan and colleagues studied 126 patients who sustained blunt splenic injury and underwent angiography to enhance the rate of splenic salvage.3 Although 86 (68%) patients had normal angiographic findings, that is, no identifiable blush to embolize, seven of the patients subsequently bled and required splenectomy. The other 40 (32%) patients underwent angioembolization for positive angiographic findings (actively bleeding vessels) but three of those patients bled and required splenectomy. Both groups had statistically similar splenic salvage rates as 10% in either group failed to achieve hemostasis. Another study examined the efficacy of angiography for blunt splenic trauma and found that of the 349 patients who were managed nonoperatively, 46 had angioembolization whereas the remaining 303 underwent observation only.4 The authors found that both groups were well matched for age, gender, initial and lowest systolic blood pressure, and hospital length of stay. When the outcomes of the 46 patients were compared with those patients who underwent observation alone, there were no statistically significant differences, thus diminishing enthusiasm for the routine use of angiography for blunt splenic injuries. Further, there are data to suggest that angiography may not be as effective in preserving spleens after blunt splenic injury as some studies using retrospective controls indicate. Harbrecht et al showed that there has been a significant increase in the detection of minor spleen injuries over time as the resolution of the CT scanner has improved.4 A higher detection rate of minor injuries would enrich the denominator with patients who are unlikely to bleed, making nonoperative management appear more successful than overall studies indicate. Compared with historical controls with patients who sustained fewer lower grade injuries in the denominator, a spurious reduction in splenectomy rates may appear to be attributed to the use of angioembolization when, in fact, it is more likely due to more patients with lower grade splenic injuries in the denominator. In a multi-institutional study, the six-month risk of delayed splenectomy after nonoperative management showed no positive association between angiography and splenic salvage.44 Without a randomized controlled trial to guide management, there is likely to be continued controversy in this area of blunt splenic injury management. Regardless of the success or failure of angioembolization in controlling bleeding, the procedure has some drawbacks as previously noted and potential complications, such as rebleeding, splenic abscess, and iatrogenic vascular injury to another organ or vessel, and adverse immune function. Bessoud et al evaluated the immunological effects after proximal splenic artery angioembolization in 37 patients by examining for Howell-Jolly bodies (basophilic nuclear remnants found in the blood after splenectomy) and serum antibody titers for pneumococcus and Haemophilus influenza B.45 The Howell-Jolly bodies were found in only 2 patients and yet all 37 patients had sufficient immunity as measured by a response to the H influenza B. Based on these findings, the authors concluded that immune function remains relatively normal after proximal splenic artery embolization. The authors recognized that this study has a small number of patients and no control group, so they suggested that a large prospective study would add more credibility to the findings. In a systematic review and meta-analysis, authors from the University of Southern California found that proximal and selective angioembolization had equivalent rates of rebleeding, infarctions, and infections, hence underscoring that proximal splenic artery embolization is not necessarily harmful compared with a selective procedure.42 Overall, despite some drawbacks, angioembolization is a valuable tool in the nonoperative management of patients with blunt splenic injury but its timing relative to the injury may be crucial. In a study that compared the results from high-use ANGIO centers (those with ANGIO use proportion >20%) and low-use ANGIO centers (those with ANGIO use proportion >0.01% to 19.9%), the authors found that the high-use centers performed the angiography sooner and therefore are more often associated with splenic salvage.39 Similarly, Banerjee noted that centers that used frequent angioembolization of the splenic artery had higher rates of splenic salvage.35
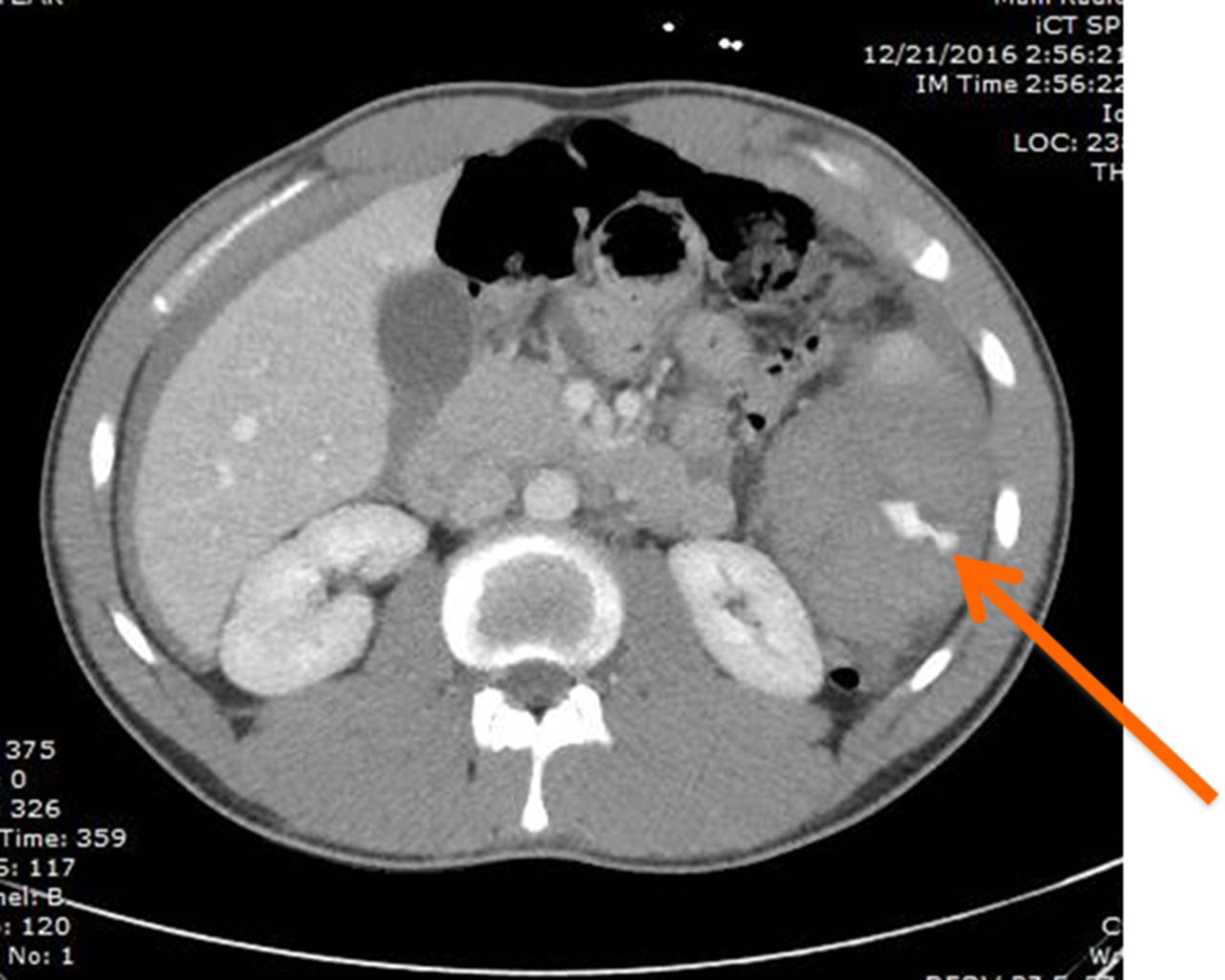
Pseudoaneurysm (arrow) noted on initial CT scan.
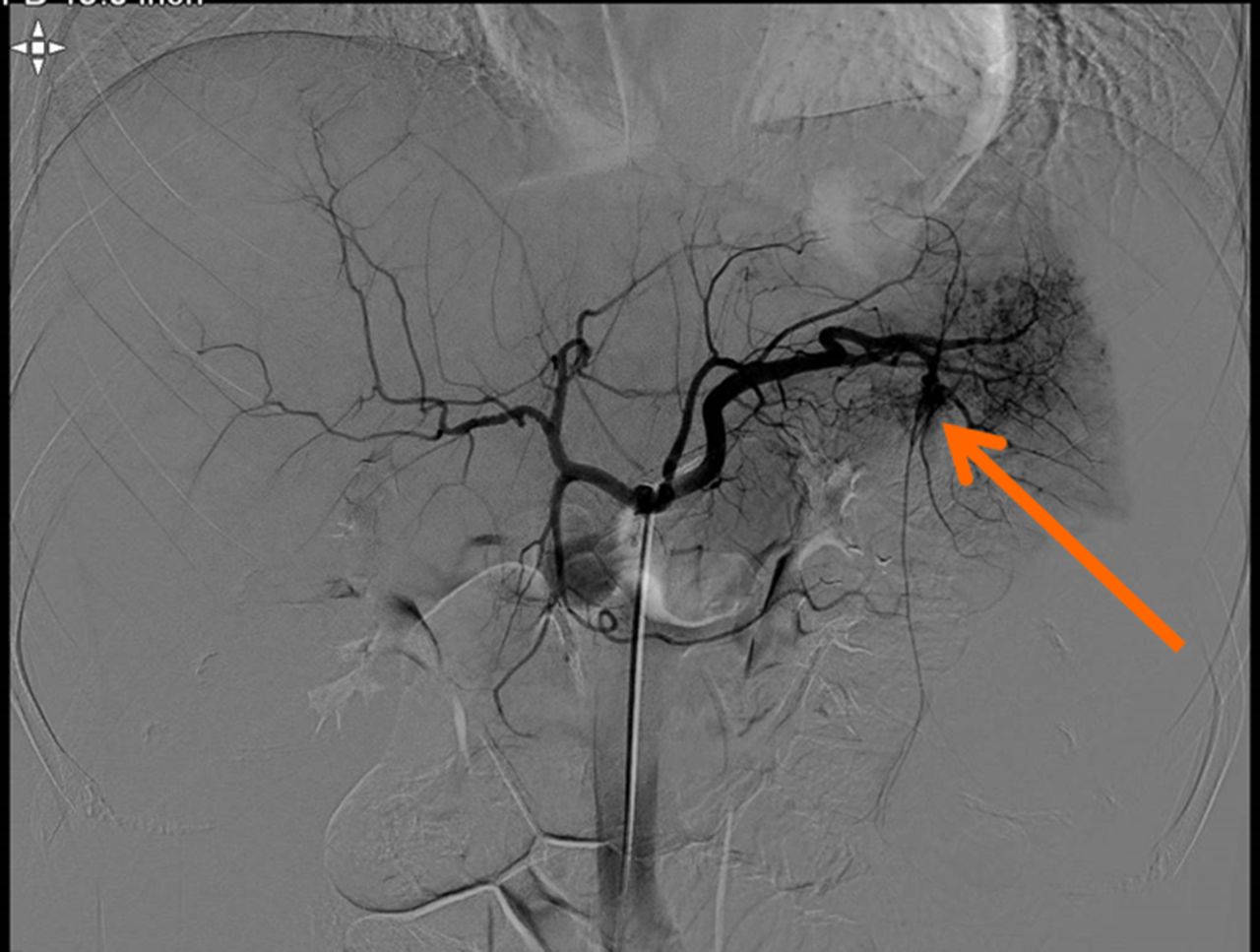
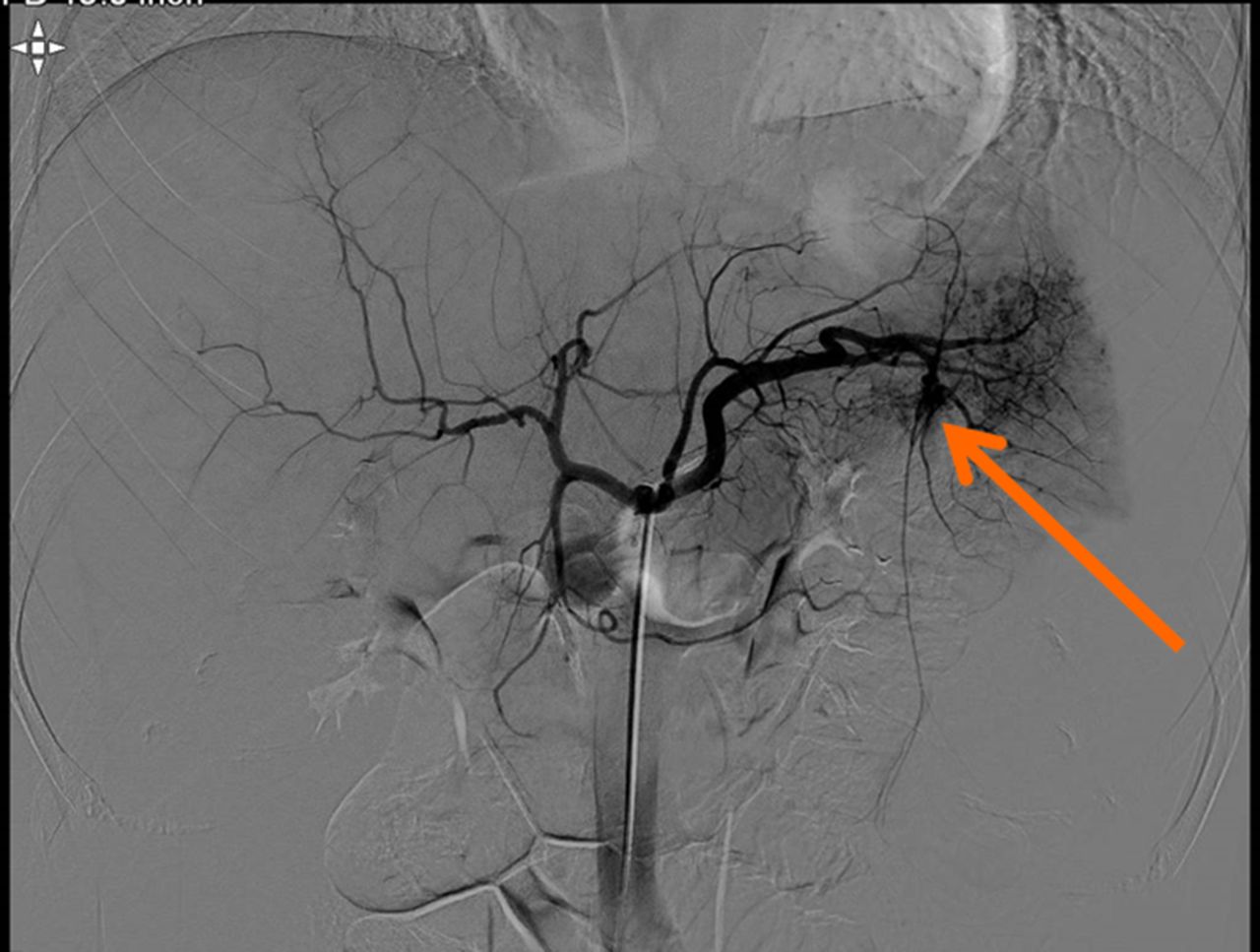
Selective angioembolization of bleeding splenic vessel (arrow).

Specimen shows embolized portion of spleen as dark area (arrow). Bleeding occurred from splenic hilum.

Transverse image of spleen with pseudoaneurysms in the upper pole. Contrast is poorly timed as neither the aorta nor pseudoaneurysm appear bright.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Repeat CT scan showing splenic hematoma and extraparenchymal pseudoaneurysm (arrow).
Monitoring the patient
Conventional patient monitoring includes the tracking of vital signs, performance of serial physical examinations, and obtaining several hemoglobin levels, all of which can be helpful in determining if the patient is hemodynamically normal and if bleeding is a concern. In addition to these assessments, a determination should be made if there are any trends toward hemodynamic instability such as a rising heart rate or a rise in diastolic blood pressure indicating a narrow pulse pressure. These trends, if identified early, may indicate that the patient may be bleeding and has failed nonoperative management. Although some studies report the frequency with which these evaluations and tests are performed, the Eastern Association for the Surgery of Trauma practice management guidelines report that there are not enough evidenced-based studies to justify a recommendation.46 Other areas that have shown variation in practice include frequency of abdominal examinations, repeat imaging, and the optimal time to mobilize the patient.
With increasing emphasis on decreasing the hospital length of stay and improving patient throughput, early mobilization and discharge of patients with blunt splenic injuries are becoming more common practices. London’s retrospective review of 454 patients who sustained solid organ injuries showed that failure rates of nonoperative management were not associated with the day of mobilization, and they concluded that prolonged bed rest is not necessary.47 But of concern also is that early discharge may not be without risk to patients as there is a potential for splenic rupture to occur in the outpatient setting.44 To understand the risk of outpatient rupture and to reduce the risk of this occurrence, it is important to understand the time course to splenectomy for those patients initially managed nonoperatively. Smith and colleagues used data from the National Trauma Data Bank to determine the time from admission to splenectomy in >23 500 patients.28 They found that about 10% of the patients required splenectomy within two hours of hospital admission. Further, those patients with isolated blunt splenic injury who were managed nonoperatively were observed for a mean of 5 days prior to discharge. Of those patients who failed nonoperative management, 95% did so in the first 72 hours of hospital admission and only a few additional patients (1.5% of the total study population) failed nonoperative management between three and five days postinjury. Therefore, the authors concluded that a three to fiveday period of observation after injury may be adequate to ensure splenic salvage. Using a statewide hospital discharge database in Tennessee, Zarzaur et al followed patients for 6 months who sustained a splenic injury and had been discharged alive from their level I trauma center. The authors found that the risk of outpatient splenic rupture was 1.4% over the 6-month period.48 The risk of outpatient rupture was much lower (0.27%) in a prospective study of 383 patients from 11 level I trauma centers.2 These data suggest that delayed splenic rupture is rare but may still occur despite the grade of injury. Overall, many splenectomies occur within 48 hours of admission and the decision to operate is based on the patient’s hemodynamic instability or abnormal physical examination findings. Further, >90% of all splenectomies occur within 5 days of injury. If early discharge is anticipated, patients should be advised of the potential risk of outpatient rupture and the associated symptoms so that they seek prompt medical attention when symptoms arise. With this study and others from Memphis, it is difficult to justify a specific length of stay for these patients, but rather a period of observation, even if it is in the outpatient setting, is recommended.5
Patient follow-up and repeat imaging
Another area of controversy has to do with the utility of repeat imaging of an injured spleen in the inpatient and the outpatient settings. For inpatients, the goal of repeat imaging is to detect the formation of latent vascular abnormalities, particularly splenic artery pseudoaneurysms, and to intervene with angioembolization to improve overall splenic salvage. The group from Memphis initiated a protocol of performing a repeat CT scan of the abdomen within 48 hours after the initial CT scan. In studies by Davis and Weinberg, a repeat CT scan showed an acceptably low failure rate of nonoperative management compared with historical controls.5 36 According to their protocol, when a new and actively bleeding vessel was identified on the follow-up CT scan, a selective angioembolization was performed. Their data showed that almost half of splenic vascular pathology detected on the repeat imaging was not present on the initial CT scan of the spleen, hence demonstrating that the repeat imaging was worthwhile.
In the outpatient setting, the use of follow-up imaging to assess splenic healing and provide support for patients to return to full physical activity is controversial. In one of the largest series examining the role of the follow-up CT scans in patients with splenic injury, Savage and colleagues found that 80% of patients with lower-grade (AAST grades I–II) injuries showed complete healing of the spleen by postinjury day 50.44 This finding suggests that for low-grade splenic injuries repeat imaging may not be indicated unless the patient develops signs and symptoms consistent with intra-abdominal bleeding. Of those patients with higher-grade injuries, 80% showed complete healing within 75 days of injury. Conversely, repeat imaging of 10% of those patients showed worsening of their injuries, with only two patients requiring splenectomies. It is likely that this subset of patients may need closer outpatient monitoring at least until signs of organ healing are documented on the outpatient CT scan. In the outpatient setting, repeat imaging may also be helpful when a patient desires to return to a vigorous activity, such as contact sports. In such circumstances, the repeat CT scan may help demonstrate that the spleen is healed and that there is a reduced chance that it will rupture if a strong blow to the abdomen occurs.
Conclusions and recommendations
The spleen, an important organ of our immune system, is a commonly injured organ in blunt trauma. Its immune function has been the basis for supporting splenic salvage, and the technological advancements of CT scan have provided the necessary visual framework to do so.
The indications for emergent splenectomy have remained consistent for years, that is, hemodynamic instability from hemorrhage and peritonitis. The evolution of splenic salvage has focused on careful patient selection, use of angioembolization, and patient follow-up, including physical examination and imaging. Based on the current literature, the following generalities and recommendations are suggested:
CT scan is a valuable adjunct for detecting the grade of organ injury, presence of hemoperitoneum, and intraparenchymal or extraparenchymal vascular abnormalities. All of these findings may factor into the decision matrix for the proper selection of patients for nonoperative management. A repeat CT scan is particularly valuable for the detection of latent pseudoaneurysms regardless of the grade of injury.
Angioembolization has evolved to become an important diagnostic and therapeutic tool for splenic salvage. The high association between vascular abnormalities identified on the initial CT scan and the need for subsequent splenectomy justifies the liberal use of angiography in the assessment of these patients. Further, the procedure is more effective in enhancing splenic salvage if used soon after the patient’s injury. Caution should be exercised that despite selective or main splenic artery embolization there are studies showing postprocedure splenic hemorrhage occurs, thus suggesting that angioembolization is not consistently reliable for arresting splenic hemorrhage and that a period of patient observation is still needed.
Patients with low-grade splenic injuries may be observed without the need for a repeat study.
It is advisable that each trauma center adopt a protocol or algorithm that is consistent with safe practice and local resources.46 49 Such a screening protocol may include mandatory angiography for all high-grade injuries or a repeat CT scan in 24 to 48 hours to rule out a developing contrast blush.
Immediate operative intervention should be performed for any patient with a splenic injury who develops hemodynamic instability or requires substantial transfusion of blood due to splenic injury.
References
Footnotes
Contributors GSR and BLZ: writing and review.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.