Article Text

Abstract
Background Pain management after injury is critically important for functional recovery. Although opioids have been a mainstay for treatment of pain, they are associated with adverse events and may contribute to long-term use or abuse. Opioid-minimizing multimodal pain regimens have the potential to reduce exposure to opioids without compromising pain control. This article details an ongoing clinical trial comparing two pill-based, opioid-minimizing, multimodal pain strategies.
Methods This is a single-center, parallel-group, randomized, controlled comparative effectiveness trial comparing two multimodal pain regimens in adult trauma patients. All patients 16 years and older admitted to the Red Duke Trauma Institute are eligible unless they are pregnant, a prisoner, under observation status, or a non-acute trauma patient. At admission to the trauma service, patients are enrolled and randomized to one of two multimodal pain regimens. The primary outcome is opioid use, measured by morphine milligram equivalents per patient per day. The secondary outcomes include pain scores, ventilator days, hospital and intensive care unit lengths of stay, occurrence of opioid-related complications, hospital and pharmacy costs, and incidence of hospital discharge with opioid prescription. Outcomes will be compared using Bayesian methods.
Discussion This trial will determine the effectiveness of two multimodal pain treatment strategies on reducing in-hospital opioid exposure in adult trauma patients. Furthermore, it will compare the two strategies on pain control and patient safety. Knowledge gained in this study can improve quality of care at this hospital and other trauma centers regardless of which medication regimen proves superior.
- trauma/ critical care
- injury
- acute pain
- Opioid
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Background
Injury hurts. Opioids have been a pillar of acute pain management after injury for decades, but opioid use after traumatic injuries and surgeries may be a precursor to opioid dependence.1 During the last two decades, 75% of patients seeking treatment for heroin addiction report initial exposure via prescription drugs.2 The incidence of persistent opioid use in opioid-naïve patients after minor and major operations is 6%, although rates that range as high as 24% in surgical subspecialties are reported.3 4 Opioid-related deaths are now more common than motor vehicle-related deaths (figure 1).5
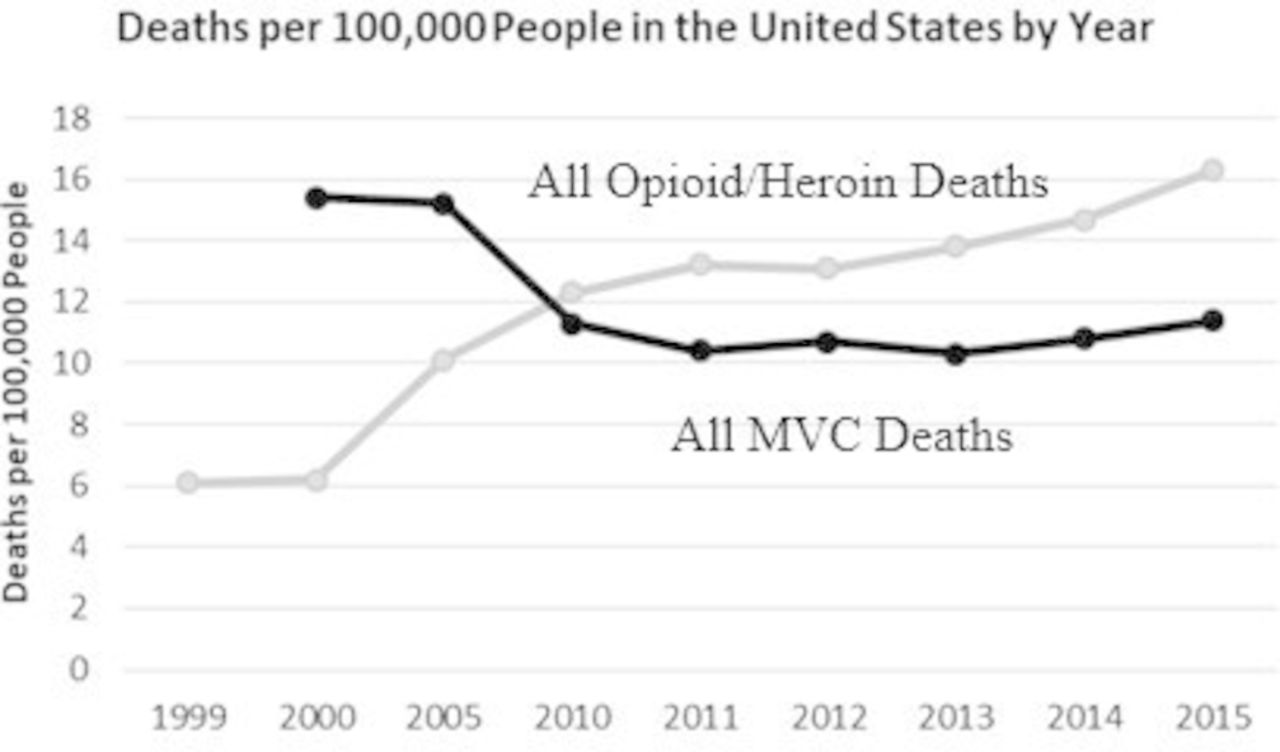
Deaths due to motor vehicle crashes and opioid and heroin overdoses. Opioid and heroin-related deaths exceed those due to motor vehicle collisions (MVC). From the Centers for Disease Control and Prevention and Insurance Institute for Highway Safety.
In 2013, local anesthesiologists and surgeons instituted a pill-based, opioid-minimizing, multimodal pain regimen (MMPR).6 Five different classes of pain medication are given in a scheduled fashion with oral opioids available as needed. The MMPR resulted in an approximately 40% reduction in morphine milligram equivalents (MME) per patient day and a virtual disappearance of patient-controlled analgesia with parenteral opioids (S Wei and JA Harvin, unpublished data).
Although the MMPR was successful in decreasing opioid use in injured patients, it included relatively more expensive drugs, such as pregabalin, celecoxib, and intravenous acetaminophen, because of their more favorable side effects or pharmacologic profiles. Due to costs, some physicians preferred to use the cheaper, generic equivalents.
The Multi-modal Analgesic Strategies for Trauma (MAST) trial is a single-center, parallel-group, randomized, controlled comparative effectiveness trial of admitted adult trauma patients comparing the original MMPR and a less expensive, more opioid-minimizing regimen. We hypothesize that the original MMPR will result in lower opioid consumption by injured patients compared with the more generic version as evidenced by lower MME per day.
Methods/design
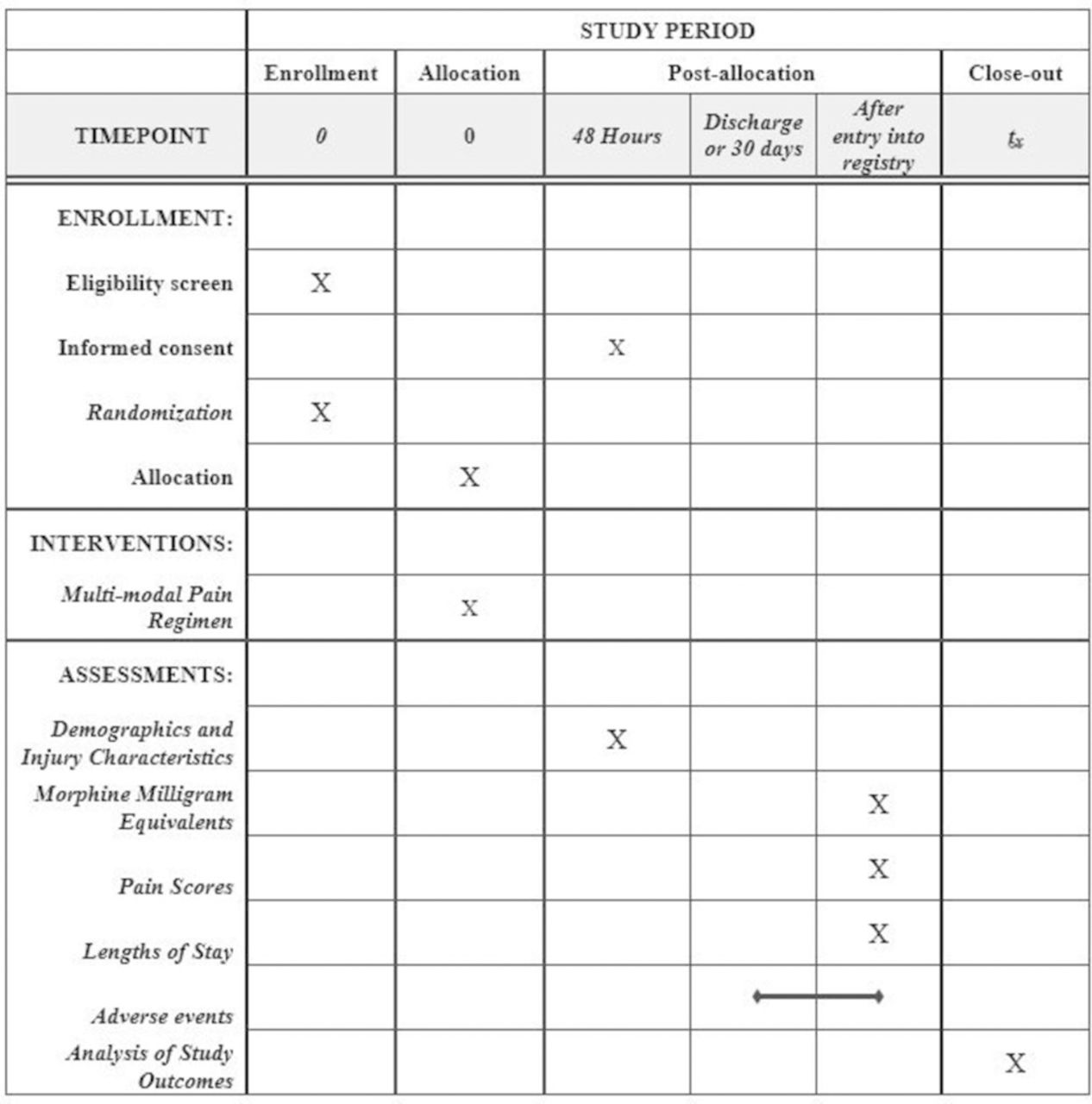
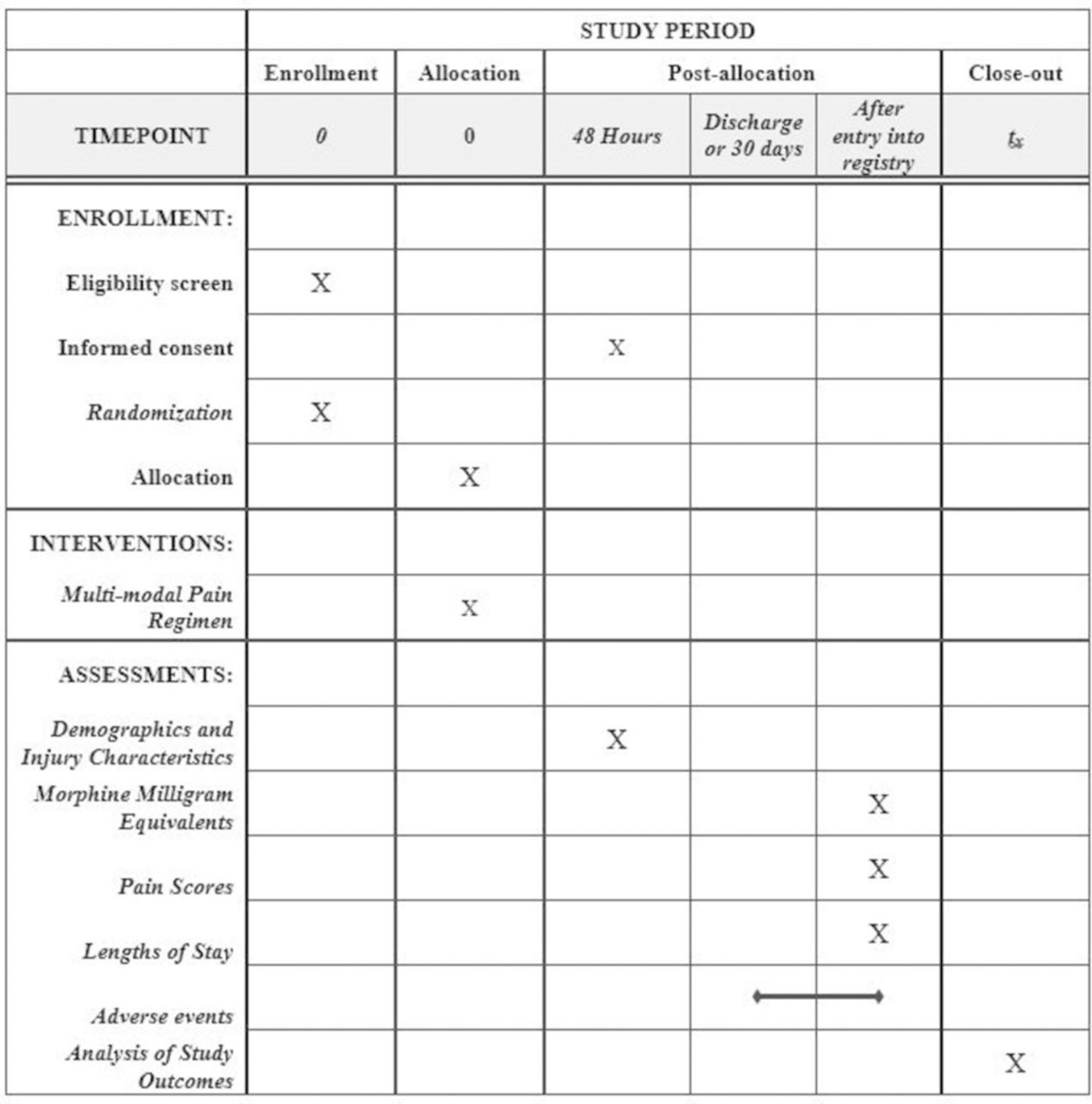
The trial was designed in accordance with the Standard Protocol Items: Recommendations for Interventional Trials 2013 guidelines (figure 2).7
{kind=link}
{kind=link}
Standard Protocol Items: Recommendations for Interventional Trials diagram. The figure details the timing of enrollment activities, intervention allocation, and assessments of outcomes during the course of the clinical trial.
Study setting
This study is being conducted at the Red Duke Trauma Institute (RDTI) at the Memorial Hermann Hospital-Texas Medical Center, which is one of two level 1 trauma centers in Houston, Texas. It is affiliated with the McGovern Medical School at the University of Texas Health Science Center at Houston.
Interventions
Treatment strategy 1
Treatment strategy 1 (table 1) consists of five classes of medication scheduled around the clock: a central prostaglandin inhibitor (acetaminophen), a non-steroidal anti-inflammatory drug (NSAID, ketorolac followed by celecoxib), a weak mu-opioid agonist (tramadol), a gabapentinoid (pregabalin followed by gabapentin), and a local anesthetic (lidocaine patch). Acetaminophen is initially provided intravenously to achieve more rapid therapeutic drug levels; once able to take pills by mouth or at 24 hours, whichever is earlier, patients are administered oral acetaminophen. A single dose of ketorolac is administered in the emergency department followed by scheduled celecoxib for the next 48 hours. Celecoxib is used during this period of increased stress to decrease the theoretical risk of gastrointestinal bleeding. After 48 hours, the patient is transitioned to scheduled naproxen. Pregabalin is scheduled in the first 48 hours as it has improved enteric absorption compared with gabapentin. After 48 hours, the patient is placed on scheduled gabapentin, which can be titrated up as needed. In addition, oral tramadol and lidocaine patches are scheduled. More information on dosing, dose adjustments, and contraindications can be found at https://med.uth.edu/surgery/acute-trauma-pain-multimodal-therapy/.
Treatment strategies 1 and 2
Treatment strategy 2
Treatment strategy 2 consists of four scheduled classes of drugs given in a scheduled fashion around the clock: a central prostaglandin inhibitor (acetaminophen), an NSAID (ketorolac followed by naproxen), a gabapentinoid (gabapentin), and a local anesthetic (lidocaine patch). Acetaminophen is administered orally from the start. A single dose of ketorolac is administered in the emergency department followed by scheduled oral naproxen. Oral gabapentin is titrated as needed. Lidocaine patches are routinely scheduled.
Patients are randomized to one of the two initial treatment strategies in the emergency department. Both regimens can be broadened or narrowed by the bedside physician during hospitalization as indicated. Adjustments may include withholding or adjusting the dosage of a medication due to comorbidities such as kidney or liver disease; withholding a medication due to interactions with other medications; and removing medications once pain control is achieved.
In both regimens, oral medications are also available as needed for breakthrough (moderate and severe) pain—oxycodone in treatment strategy 1 and either tramadol or oxycodone in treatment strategy 2. Either regimen can be titrated up or down depending on the patient’s level of pain. Adjuncts can also be added, including oral methadone for long-acting opioid pain relief, regional anesthesia, lidocaine infusion, and ketamine infusion. Although their use is discouraged, intravenous opioids can be administered as needed.
An order set is available within the electronic medical record to facilitate compliance with correct medication ordering.
Eligibility criteria
All adult patients (≥16 years of age) admitted to the adult trauma service are screened for eligibility. Pregnant women, prisoners, patients placed in observation, and non-acute trauma admissions, including readmissions, are excluded. Patients are not excluded if they have a contraindication to one or more medications in the MMPRs.
Outcomes
The primary outcome is opioid use per day until discharge or 30 days postadmission if still hospitalized, calculated by tallying the MME of all opioids received per day during hospitalization (table 2). This outcome captures the effectiveness of the combined non-opioid medications in achieving pain control and in reducing opioid administration.
MME conversion factors
The following secondary outcomes of the study will be measured until discharge or 30 days postadmission if still hospitalized:
The average of the average daily pain score using a numeric rating scale (0=no pain, 10=worst pain).
Incidence of opioid-related complications, such as ileus, unplanned intubation, unplanned admission to an intensive care unit, and use of an opioid-reversal agent.
Additional secondary outcomes include discharge from the hospital with an opioid prescription, overall and pharmacy costs, and ventilator, hospital, and intensive care unit-free days.
Sample size
The objective of this study is to provide the most precise, unbiased estimate of treatment effect possible. As such, we plan to conduct the largest feasible study in a 12-month period on which to base these estimates. Based on data from the past 3 years, approximately 167 patients are admitted to the adult trauma surgery service per month. We aim to enroll 75% of these patients or 1506 patients in the 12-month period. After 17 weeks of enrollment, 570 patients have been randomized to one of the two treatment strategies.
Randomization
Randomization is in a 1:1 allocation and stratified by unit of admission using a random sequence generated by an independent statistician. Allocation is performed by the inhouse research assistant using REDCap.8
Blinding
Providers and patients are not to be blinded to treatment allocation due to feasibility and cost. To address this issue, the opioid administration and pain score data (entered by nurses during routine clinical care) will be captured directly from the electronic medical record and the majority of outcomes will be obtained using our trauma registry (blinded outcome assessor).
Analysis
Bayesian methods will be used to complement traditional frequentist analyses. Bayesian methods combine estimates of treatment effect based on existing data (prior probability) with observed data from the trial to develop a distribution of potential treatment effects (posterior probability). Such methods offer several advantages. First, Bayesian methods, unlike frequentist approaches, estimate the probabilities that treatment effects of varying magnitudes exist (ie, a 5%, 10%, and 20% difference in MMEs). Second, Bayesian approaches can incorporate new data to continuously update the prior probability. As such, the analyses from the current project may inform the design and analysis of subsequent studies. Third, the process of updating a prior with data provides a mechanism for continued monitoring of an established program for quality control.
Broadly, the data analysis strategy will use generalized linear multilevel modeling with level 2 random effects to account for clustering of participants within the unit of admission and, where applicable, observations within participants. Modeling will use R V.3.4 and Stan V.1.10.9 10 Initial analyses examining group differences for baseline variables will use cross-tabulation, analyses of variance, and examination of correlations between baseline variables and specified outcomes. If group differences in confounders are detected, analyses with and without those relevant variables will allow determination of their effect on estimates of treatment effectiveness.11 12
All analyses will be conducted on an intention-to-treat basis. Bayesian approaches will implement joint modeling of observed outcomes and the missing data which are robust to ignorable missingness.13 Non-ignorable missing data patterns will be addressed through pattern-mixture modeling methods.14 Sensitivity analyses will evaluate the robustness of analytic conclusions to missing data. Convergence of Bayesian analyses on the posterior distributions via Monte Carlo Markov chain will be assessed via graphical (Gelman-Rubin plots) and quantitative (Gelman-Rubin diagnostics and effective sample size) evidence. Evaluation of posterior distributions will permit statements regarding the probability that effects of varying magnitudes exist, given the data. Specification of diffuse, neutral priors will reflect the initial uncertainty regarding effect sizes.
Data and safety monitoring board
As this is a comparative effectiveness of two commonly used regimens, no data and safety monitoring board will be formed. Major adverse events, including death, will be reported to the Institutional Review Board (IRB).
Research approval
The IRB of McGovern Medical School approved the study protocol on March 2, 2018. Enrollment began on April 2, 2018 and is scheduled to continue for 12 months.
Informed consent
As this is a minimal-risk, comparative effectiveness trial of two commonly used regimens, a waiver of consent to randomization was approved by the IRB. When appropriate, research staff approach enrolled patients and/or their legally authorized representatives to inform them of the trial, provide educational materials, and obtain consent for the use of personal health information. If consent to use personal health information cannot be obtained due to death or early discharge, the consent is waived and the patient data included.
Discussion
Adequate pain control without opioids in traumatically injured patients can be challenging for multiple reasons. First, multiple sites of injury may limit the effectiveness of alternative pain control strategies such as regional anesthesia. Second, patients often undergo multiple procedures and operations such that pain may fluctuate during hospitalization. Nonetheless, MMPRs may have a role in achieving adequate pain control while minimizing opioids.
In this pragmatic, parallel-group, randomized, controlled comparative effectiveness trial of two pill-based, opioid-minimizing MMPRs, we hypothesize that treatment strategy 1, including intravenous acetaminophen, pregabalin, and celecoxib, will lead to a reduction in overall MME used per day as compared with treatment strategy 2. The potential benefits of treatment strategy 1 include more rapid achievement of therapeutic levels of intravenous acetaminophen and pregabalin than their generic formulations and decreased concerns about bleeding with celecoxib than with non-selective NSAIDs.15 16
Treatment strategy 1 has several limitations, starting with increased expense. Although the cost of treatment strategy 1 is only $160 more expensive than treatment strategy 2 for hospitalization, the excess costs amount to over $320 000 per year when multiplied by the approximately 2000 admissions per year at the RDTI. However, this estimate does not account for the direct and indirect costs of opioid dependence, which is often a consequence of in-hospital opioid exposure. Second, the strategy may not be generalizable to those institutions with strict formulary controls. Finally, treatment strategy 1 may not be truly opioid-minimizing. Although historically considered to be a “safe” alternative to other opioids, tramadol administered at high doses has effects similar to those of other opioids and can lead to addiction.
The MAST trial is emblematic of a learning trauma care center as we aim to learn from every patient encounter and integrate that knowledge into future clinical care. Additionally, it supports our goal of creating a culture of learning at the trauma center.17 A major focus of the trial is education of all relevant stakeholders. Providers will receive monthly lectures on the use of non-opioid pain medications, calculation of MMEs, and appropriate opioid prescribing. Patient education includes setting realistic expectations of pain control after injury, responsible opioid use, and safe opioid storage and disposal.
In conclusion, the MAST trial is a pragmatic, randomized trial designed to identify the most effective, opioid-sparing MMPR. Furthermore, the trial builds on our culture of learning to educate patients and providers on safe opioid prescribing and increase the use of effective non-opioid pain medications.
Footnotes
Contributors Conception and design: JAH, CG, LEV, KLM, JP, CCM, JET, JBH, CEW, and LSK. Drafting of the article: JAH, CG, and LEV. Critical review of the article: LEV, KLM, JP, CCM, JET, JBH, CEW, and LSK.
Funding JAH is supported by the Center for Clinical and Translational Sciences, which is funded by the National Institutes of Health Clinical and Translational Award UL1 TR000371 and KL2 TR000370 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Competing interests None declared.
Patient consent Not required.
Ethics approval UT Health Committee for the Protection of Human Subjects.
Provenance and peer review Not commissioned; externally peer reviewed.