Article Text

Abstract
Background Patients with trauma are at risk for renal dysfunction from hypovolemia or urological injury. In austere environments, creatinine values are not available to guide resuscitation. A new portable device, the Stat Sensor Point-of-care (POC) Whole Blood Creatinine Analyzer, provides accurate results in <30 s and requires minimal training. This device has not been evaluated in trauma despite the theoretical benefit it provides. The purpose of this study is to determine the clinical impact of the POC device in trauma.
Methods 40 patients with trauma were enrolled in a prospective observational study. One drop of blood was used for creatinine determination on the Statsensor POC device. POC creatinine results were compared to the laboratory. Turnaround time (TAT) for POC and laboratory methods was calculated as well as time elapsed to CT scan if applicable.
Results Patients (n=40) were enrolled between December 2014 and March 2015. POC creatinine values were similar to laboratory methods with a mean bias of 0.075±0.27 (p=0.08). Mean analytical TATs for the POC measurements were significantly faster than the laboratory method (11.6±10.0 min vs 78.1±27.9 min, n=40, p<0.0001). Mean elapsed time before arrival at the CT scanner was 52.9±34.2 min.
Conclusions The POC device reported similar creatinine values to the laboratory and provided significantly faster results. POC creatinine testing is a promising development for trauma practice in austere environments and workup of a subset of stable patients with trauma. Further study is warranted to determine clinical impact, both in hospital-based trauma and austere environments.
- laboratory
- Creatinine
- Point-of-care testing
- renal function
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Trauma patients are at risk for renal dysfunction from hypovolemia or urological injury. In austere environments, however, creatinine values are typically not available to guide resuscitation. A new portable device, the Stat Sensor Point-of-care (POC) Whole Blood Creatinine Analyzer (Nova Biomedical, Waltham, Massachusetts, USA), has been evaluated in other fields, including monitoring resuscitation in burn surgery,1 ,2 trending post-operative renal function in patients with renal transplant,3 and in radiology departments to screen for renal failure prior to contrast administration.4 It provides accurate results4–6 in <30 s and requires minimal training. This device has not been evaluated in the trauma setting despite the theoretical benefit it provides. This device can potentially be used for rapid creatinine results in austere environments7 that historically do not have access to renal function tests.
The purpose of this study is to determine the potential clinical impact of this POC creatinine analyzer in the trauma setting. Our hypothesis is that the POC creatinine device can be integrated into the existing trauma system and will result creatinine values similar to the hospital laboratory, but significantly faster.
Methods
The present study was approved by the Institutional Review Board. We performed a prospective observational study of adult patients who came into the emergency room at a single Level I trauma center coded as major traumas, based on prehospital triage criteria. Prisoners, pediatric patients (<18 years old), and pregnant women were excluded. Patients were also excluded if their planned workup did not include creatinine testing. Enrollment occurred between 6:00 and 18:00, on weekdays between January and April of 2015, in a population of convenience. The primary outcome was POC creatinine level, compared to the laboratory value. The secondary outcomes were turnaround time (TAT) of the POC and laboratory creatinine levels and the time elapsed for the patient to arrive at the CT scanner, when applicable.
For each enrolled patient, a single drop of blood was taken from the same initial sample as the patient's other laboratory tests. The blood sample was tested using the POC whole blood creatinine meter. The creatinine value, the time it was obtained, and the patient's arrival time were recorded. The creatinine and time information was not provided to the managing trauma team and did not impact clinical decisions. Informed consent was obtained within 24 hours of arrival, prior to further data abstraction from the medical record.
The electronic medical record was used to obtain the laboratory creatinine value, the time it became available, and the time the patient arrived at the CT scanner, when applicable. POC creatinine results were compared directly to the laboratory value. TATs for POC and laboratory methods were calculated as well as time elapsed to CT scan when applicable. Creatinine values and TATs were calculated using a standard t-test.
Results
Forty patients were enrolled between December 2014 and March 2015. The mean age was 71.2 years. Thirty per cent were women. Ninety-five per cent had sustained blunt trauma and 20% required operative management. The median hospital length of stay was 2 days. The median injury severity score was 4 (range 0–36). Please see table 1 for demographics.
Demographics
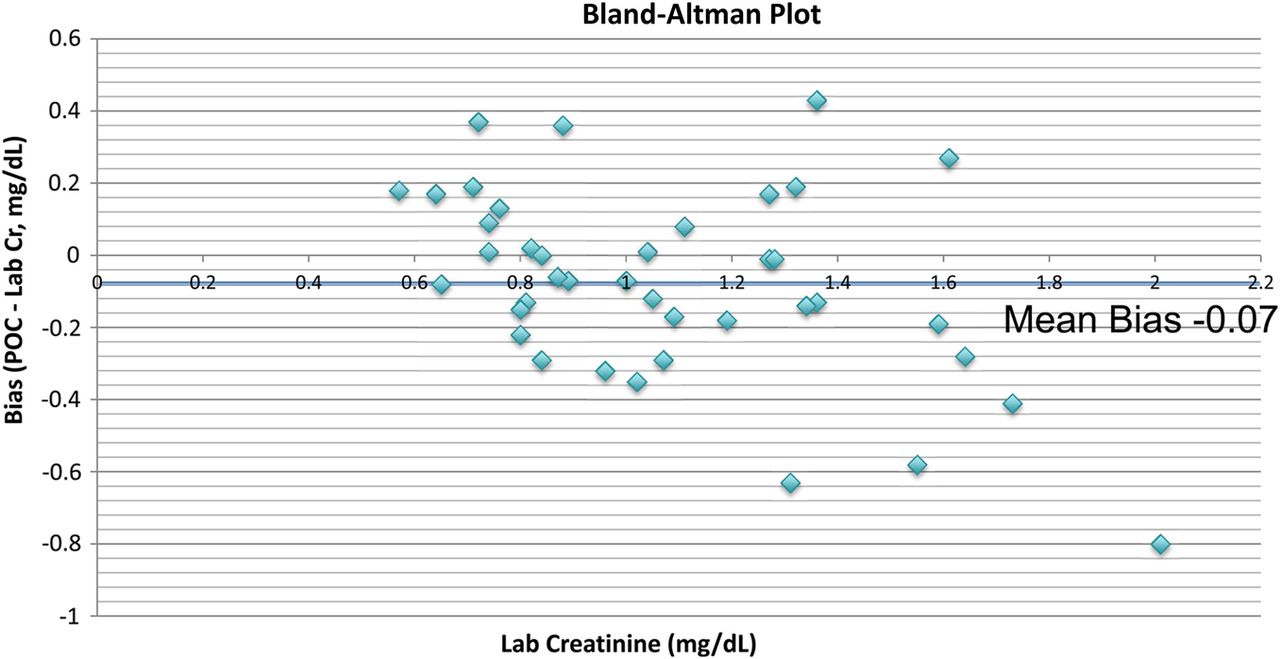
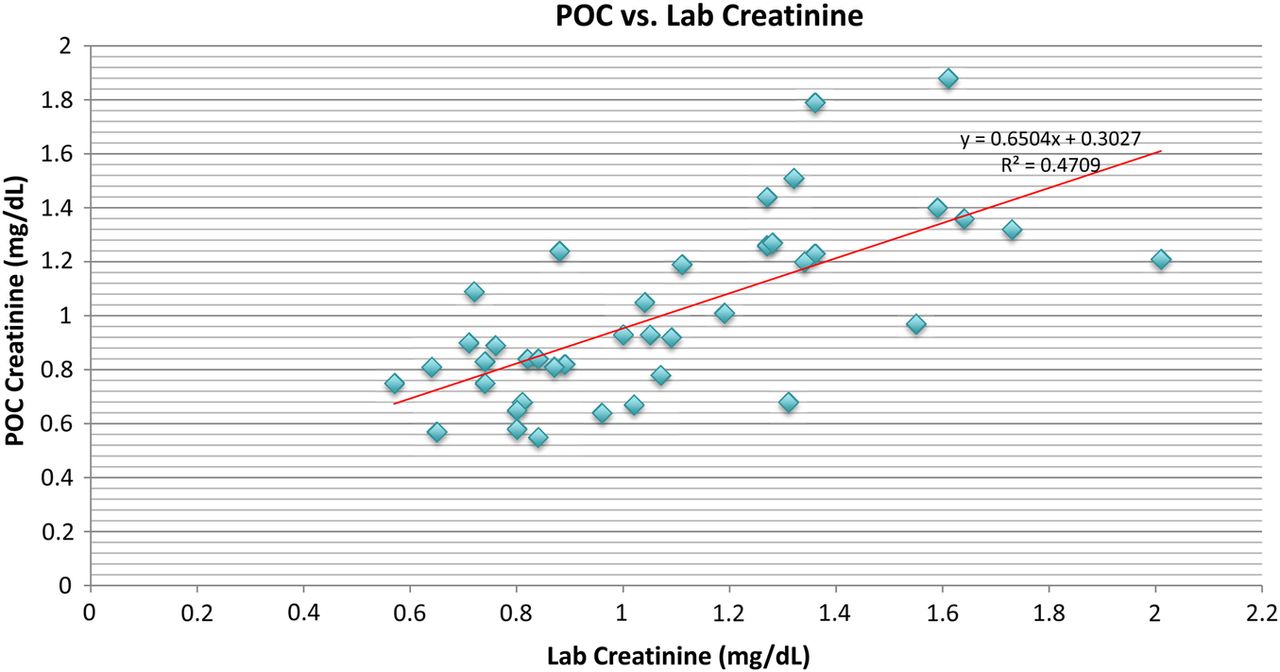
Mean POC creatinine values were 1.01±0.33, compared to 1.08±0.34 for laboratory creatinine. The difference between these values was not statistically significant, with a mean bias or difference between POC and laboratory values, of 0.075±0.27 (p=0.08). Figure 1 is a Bland-Altman Plot, which shows the laboratory creatinine value on the x axis and the bias on the y axis. Figure 2 plots laboratory creatinine on the x-axis and POC creatinine on the y-axis.
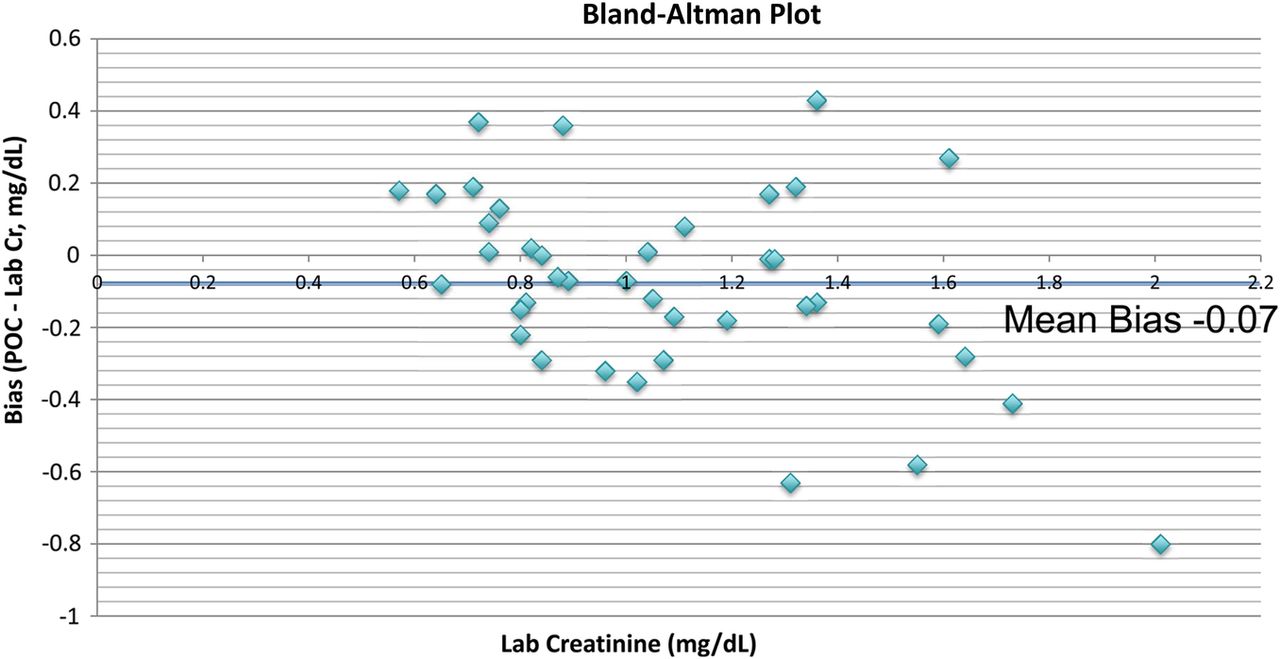
Bland-Altman plot. POC, point-of care.

POC versus laboratory creatinine. POC, point-of care.
Mean analytical TATs for the POC measurements were significantly faster than the laboratory method (11.6±10.0 min vs 78.1±27.9 min, p<0.0001). The mean elapsed time before arrival at the CT scanner for the 30 patients who underwent CT imaging was 52.9±34.2 min. At the time of CT scanning, 29 of 30 had POC creatinine values available, while only 5 of 30 had laboratory creatinine values available. Please see table 2 for these results.
Creatinine data
Discussion
The purpose of this prospective observational study is to determine the potential clinical impact of this POC creatinine analyzer in the trauma setting. While its accuracy was known in other settings, it was important to know if the device could be used in a practical manner in the trauma setting. We had three key findings: the device provided accurate creatinine values, the information was available rapidly, typically before contrast was administered for imaging, and it was successfully implemented in our trauma workflow. The study supported the hypothesis that the POC creatinine device can be integrated into the existing trauma system and will result in creatinine values similar to the hospital laboratory, but significantly faster. The strength of this study is that it demonstrates prospectively that the device is functional in the trauma setting. The study design was chosen since the use of this device has not been established in trauma.
This study has several limitations. As a small, prospective observational study, it does not evaluate a specific intervention; neither does it influence the situations in which this device should be used. Further study is needed to determine if obtaining creatinine values truly impacts management in the practical setting, as well as to evaluate the short-term and long-term outcomes of using this information to tailor workup and management of individual patients.
On initial observation, the p value of 0.08 for the difference between POC and laboratory creatinine values is close to our predefined cutoff of 0.05, suggesting that there is a chance there would be a statistically significant difference if a larger sample was evaluated. Despite this, the absolute difference, or bias, of 0.07 is low and is the more critical value to evaluate in laboratory medicine. This tells us that even if there is a systematic difference between the values that is due to more than chance, it is small enough to not be clinically significant. This could be assessed further with a larger study. The difference in values may be explained by the difference in biochemical reactions as the POC device uses electrochemistry to test whole blood and the laboratory uses the kinetic Jaffe reaction on plasma.
The vast majority of patients in this study had normal creatinine values. Therefore, while the data support the accuracy of the creatinine values for patients with normal creatinine, the accuracy outside of the normal range was not demonstrated. A larger study or a different patient population would be necessary to look at the device in patients with renal failure.
This device may affect practice in austere environments, where determination of creatinine values with a small, inexpensive device could prove beneficial. There is a precedent for POC creatinine determination in an austere environment;7 more research would be needed to determine its role in the care of trauma and surgical patients. Potential uses include resuscitation and management during prolonged transport and management of perioperative patients without access to a full laboratory. Forward surgical teams in role II settings may benefit by having an easily portable device that can be transported to each destination. Additionally, development is underway for similar devices that measure other important values, including hemoglobin.
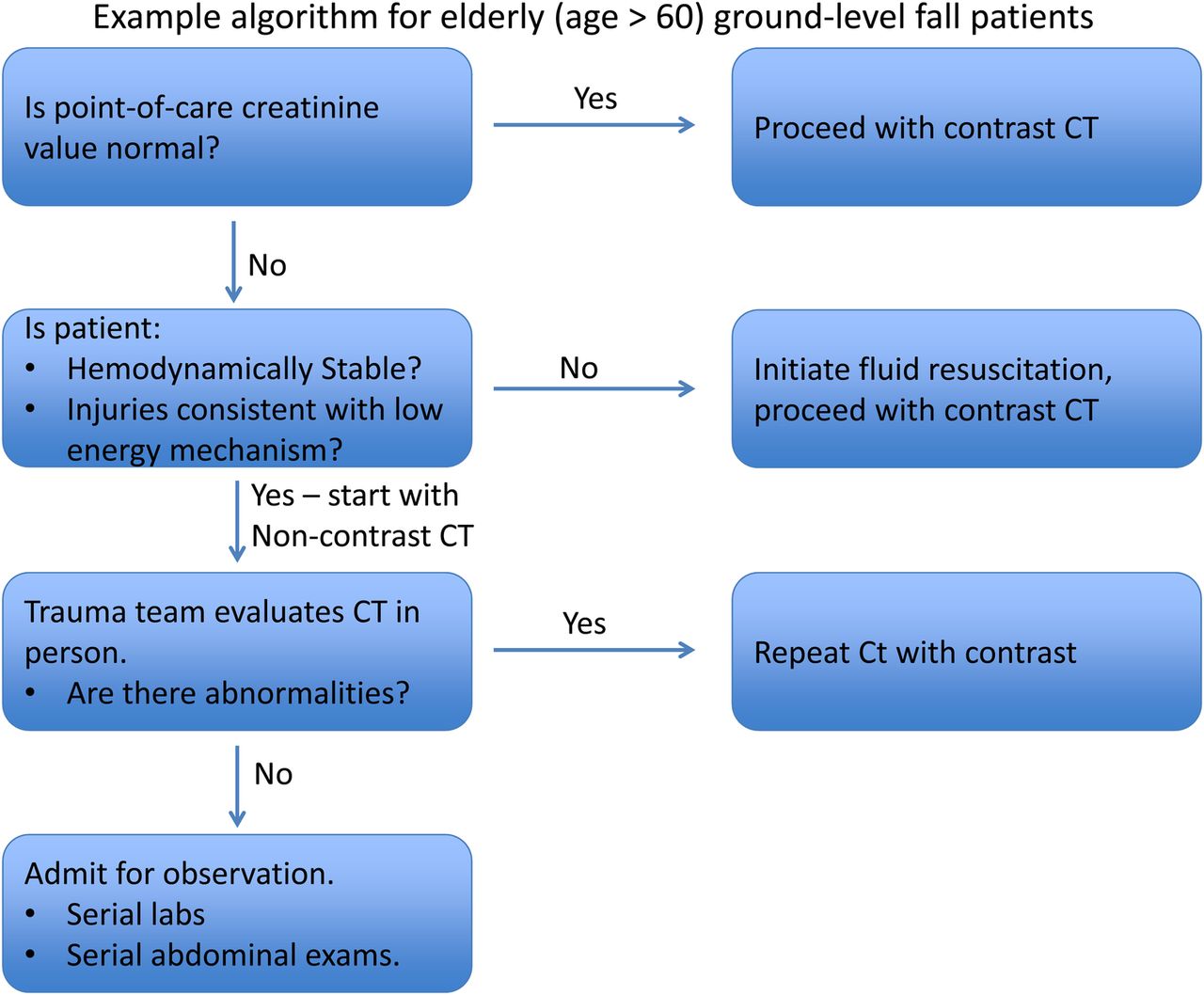
This study also has the potential to affect a subset of trauma patients who have a low probability of critical findings on CT scanning, but have an increased likelihood of developing contrast-induced nephropathy. Examples of patients who may benefit are elderly patients who sustain a ground level fall requiring CT imaging and patients who are found down and at risk for rhabdomyolysis. The elderly portion of the trauma population is steadily growing, and even low energy mechanisms can cause significant injury in these patients. If found to have elevated creatinine, elderly patients could be resuscitated prior to a delayed CT scan with contrast, or an algorithm could be used to initially scan without contrast. Notably, the fact that creatinine values were available prior to contrast administration in this study means that this algorithm could potentially be implemented with minimal delay of care.
Determination of creatinine values with a POC device is feasible in a major trauma center. More research would be necessary to determine its feasibility in an austere environment. The device is quite portable; however, the test strips must be refrigerated in the long term.
Our outcome of obtaining similar creatinine results sooner than laboratory values is likely reproducible in further clinical practice or research. It required no change to the structure of our trauma service. Further research will be necessary to determine if obtaining creatinine values faster leads to improvements in outcomes such as rate of contrast-induced nephropathy or time markers such as time to CT scanner, time to operating room, or time to admission.
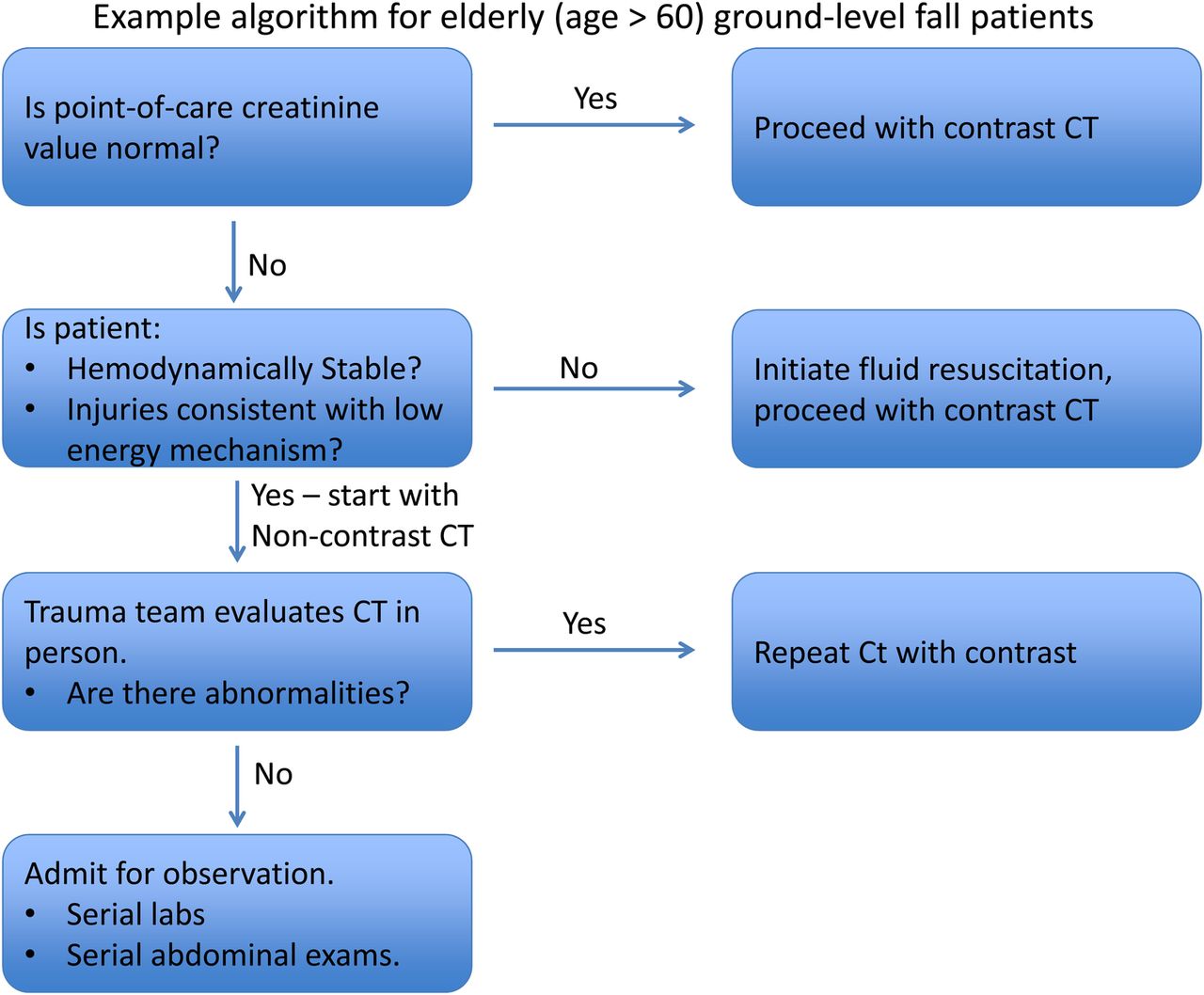
A randomized controlled trial would be beneficial to determine if POC creatinine determination, coupled with a protocol for managing select patients with a low energy trauma mechanism, can achieve better outcomes. Please see figure 3 for a sample algorithm for use in elderly ground level fall patients.
{kind=link}
{kind=link}
{kind=link}
Example algorithm for elderly (age>60) ground-level fall patients.
This device also has the potential to be used in austere environments due to its small size and inexpensive cost. Rapid determination of renal function can tailor resuscitation efforts during extended transport, or in the field. A rigorous study to establish feasibility can be followed by determination of the patient populations likely to benefit and the algorithms that can incorporate rapid creatinine values. Results of the POC testing also need to be tested in patients with profound shock and high ISS.
POC creatinine testing is a promising development for trauma practice in austere environments and workup of a subset of stable trauma patients with trauma. Further study is warranted to determine the clinical impact, both hospital-based trauma and austere environments.
Acknowledgments
The study was supported in part by a National Heart Lung and Blood Institute (NHLBI) Emergency Medicine K12 award (Scholar: Nam Tran, Award number 5K12HL108964, PI: Nathan Kuppermann). Point-of-care creatinine testing devices and reagents were donated by Nova Biomedical (Waltham, MA, USA).
Footnotes
This project was presented at ASC in Jacksonville, FL, on 2 February 2016.
Contributors AJC contributed to study design, was the study coordinator, data analysis, primary role in manuscript writing and created figures. ESS and JMG contributed to study design, data evaluation and interpretation, critical review of manuscript. NKT was involved in study design, technical device expertise, data evaluation and interpretation, critical review of manuscript. EG contributed to study design, resource coordination and critical review of manuscript. JM and JS were involved in data acquisition.
Funding Nova biomedical, National Heart, Lung and Blood Institute, 10.13039/1000000505K12HL108964.
Competing interests None declared.
Ethics approval UC Davis IRB.
Provenance and peer review Not commissioned; externally peer reviewed.