Article Text

Abstract
Background Firearm injury is a major public health burden in the USA. Absent a single, reliable data source, researchers have attempted to describe firearm injury epidemiology using trauma registry data. To understand the implications of this approach, we compared trends in firearm assault incidence and case-fatality in Philadelphia over 10 years from two sources: the Pennsylvania Trauma Outcomes Study (PTOS), Pennsylvania’s state-mandated trauma registry, and the Philadelphia Police Department database (PPD) of firearm assaults.
Methods We included PTOS firearm assault patients treated in Philadelphia County and PPD database firearm assault victims from 2005 to 2014. We calculated counts of fatal and non-fatal incidents using PTOS and PPD data. We used generalized linear models adjusted for seasonality to estimate temporal trends in firearm assault rates and case-fatality for both data sources and compared patient demographics and injury characteristics between the two.
Results A total of 6988 PTOS and 14 172 PPD subjects met the inclusion criteria. In both data sets, firearm assault rates decreased significantly during the study period (PTOS: 5.19 vs. 3.43 per 10 000 person-years, change/year: −0.21, 95% CI −0.26 to –0.16; PPD: 10.97 vs. 6.70 per 10 000 person-years, change/year: −0.53, 95% CI −0.62 to –0.44). PTOS mean case-fatality rate was 26.5% and decreased significantly (change/year: −0.41, 95% CI −0.78% to 0.04%). PPD mean case-fatality rate was 18.9% with no significant change over time (p=0.41).
Discussion Relative to PPD data, PTOS data underestimated firearm assault incidence and overestimated mortality. Trends in case-fatality rates were disparate across the two data sources. A true understanding of firearm injury in the USA requires comprehensive data collection on the incidence, nature, and severity of these injuries. As trauma registry data are by definition incomplete, combining data sources is essential. Local law enforcement data are an important potential source for studying city-level firearm injury.
Level of evidence Level III, epidemiological.
- time trends
- gunshot
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Firearm violence is a major public health problem in the USA. An accurate understanding of firearm injury epidemiology is critical to effectively target and evaluate effects of prevention efforts. Data from national and state trauma registries, hospital registries, government and public health agencies, law enforcement, and the media have been used to report firearm injury epidemiology.1–5 However, there remains no comprehensive, gold standard data source for the study of firearm injury in the USA.
In the trauma surgery literature, researchers have attempted to use trauma registry data to describe the epidemiology of firearm injury and assess potential interventions to reduce firearm injury (including legislation) and improve outcomes for victims.6–11 However, the selection criteria for patient inclusion into trauma registries are not uniform, and trauma registry data do not represent the complete epidemiologic picture of firearm injury. Specific biases associated with the use of trauma registry to describe trends in firearm injury epidemiology are currently unknown, but at minimum, patients can only be included if they are treated in a hospital that participates in the registry. This likely excludes injuries too minor to require medical care, which still may have epidemiologic significance, as well as injuries treated at non-trauma center hospitals and injuries resulting in immediate death at the scene. Millimeters of difference in a bullet’s trajectory can result in a major difference in injury severity, meaning that minor injuries are part of the same larger phenomenon as more serious ones. To be truly meaningful, an epidemiologic resource must identify all firearm injuries.
Recent analyses suggest that non-fatal firearm injuries may be driving a “hidden epidemic” of gun violence.12 13 However, reports have differed regarding trends in firearm injury case-fatality rates during the past decade. Some studies have found an overall decrease in firearm injury case-fatality, whereas others demonstrate relative stability in case-fatality rates.12–14 Debate exists regarding the driving forces behind these epidemiologic trends, with some researchers arguing that firearm injury severity is increasing over time.7 10 15 It is clear that the ongoing lack of reliable data sources, especially for non-fatal firearm injuries, limits our current ability to accurately characterize trends in firearm injury epidemiology.
In Philadelphia, we have identified two potential data sources for both fatal and non-fatal firearm injury: Pennsylvania Trauma Outcomes Study (PTOS), Pennsylvania’s mandated central trauma registry, and the Philadelphia Police Department database (PPD) of firearm assaults. In this study, we compared trends in firearm assault incidence and case-fatality in Philadelphia, Pennsylvania over 10 years using PTOS and PPD data. In the absence of a true gold standard for population-level firearm injury, we sought to evaluate these two very different data sources with the aim of optimizing our understanding of firearm injury epidemiology in Philadelphia.
Methods
PTOS includes patients treated in a trauma center in the state of Pennsylvania meeting the following criteria: intensive care or step-down unit admission, death on hospital arrival or during admission, transfers in or out of the hospital, admission for greater than 48 hours, or admission for greater than 36 hours with an injury severity score of 9 or greater. The PPD data set contains all shootings classified as assaults that result in individual injury or fatality in Philadelphia, with assault defined as non-self-inflicted missile injury. These data are drawn from police reports, which include mandated reporting of firearm injuries by healthcare providers. PPD does not include any measure of injury severity, but does notate the location of wounds. These data are publicly available and searchable from 2015 forward through OpenDataPhilly.16 Earlier data were obtained directly from the police department.
For this analysis, we extracted the individual-level records of PTOS patients sustaining firearm assaults occurring in Philadelphia County (International Classification of Diseases Ninth Revision E-codes E922, E955, E965, and E985 with assault intent) and firearm assault victims from the PPD database from 2005 to 2014. Variables common to both data sets and relevant to this analysis were individual age, sex, race/ethnicity, and mortality.
We aggregated these individual-level data as counts of fatal and non-fatal incidents per month and year for each data set. We then compared the demographic and injury characteristics and injury outcomes of patients recorded in the PTOS and PPD data sets using two-sided Student’s t-tests and χ2 tests. Finally, we evaluated temporal trends in firearm assault rates and fatality for each data source during the study period using generalized linear models adjusting for seasonality. Given stability in the Philadelphia population during the study period, we used 2010 census-derived population estimates.17
Results
From 2005 to 2014, there were 6988 firearm assault patients in the PTOS database and 14 172 firearm assault victims in the PPD database. PPD subjects were younger than PTOS subjects: (27±13 vs. 28±10 years, p<0.001), more likely to be female (7.8% vs. 5.9%, p<0.001), and less likely to be black (84.2% vs. 89.3%, p<0.001).
The incidence of PTOS firearm assaults decreased from 5.19 per 10 000 person-years in 2005 to 3.43 per 10 000 person-years in 2014 (change per year: −0.21, 95% CI −0.26 to –0.16). The incidence of PPD firearm assaults also decreased significantly from 2005 to 2014 (10.97 vs. 6.70 per 10 000 person-years, change per year: −0.53, 95% CI −0.62 to –0.44) (figure 1).
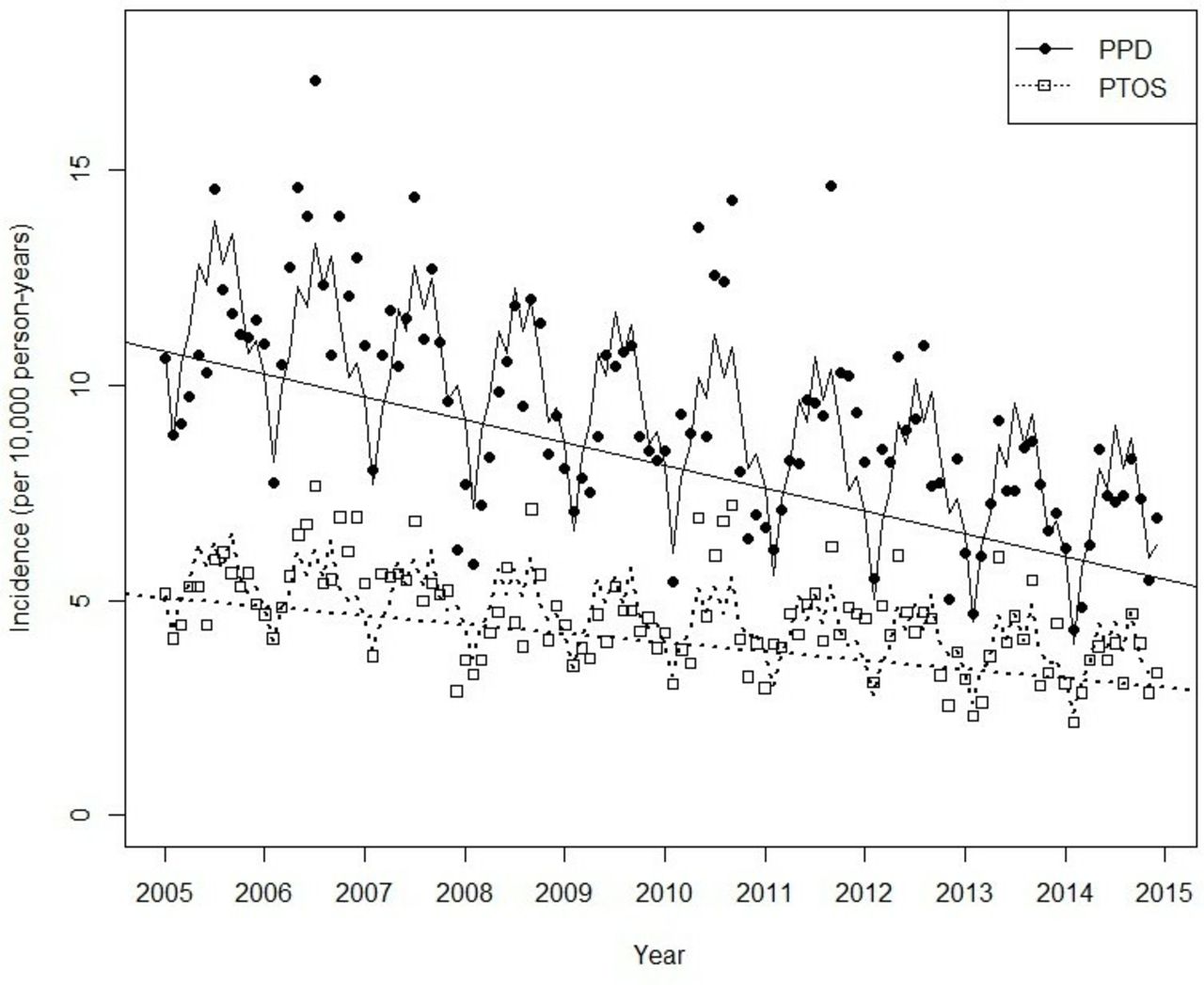
Firearm assault incidence in Philadelphia Police Department (PPD) versus Pennsylvania Trauma Outcomes Study (PTOS) data, 2005–2014.
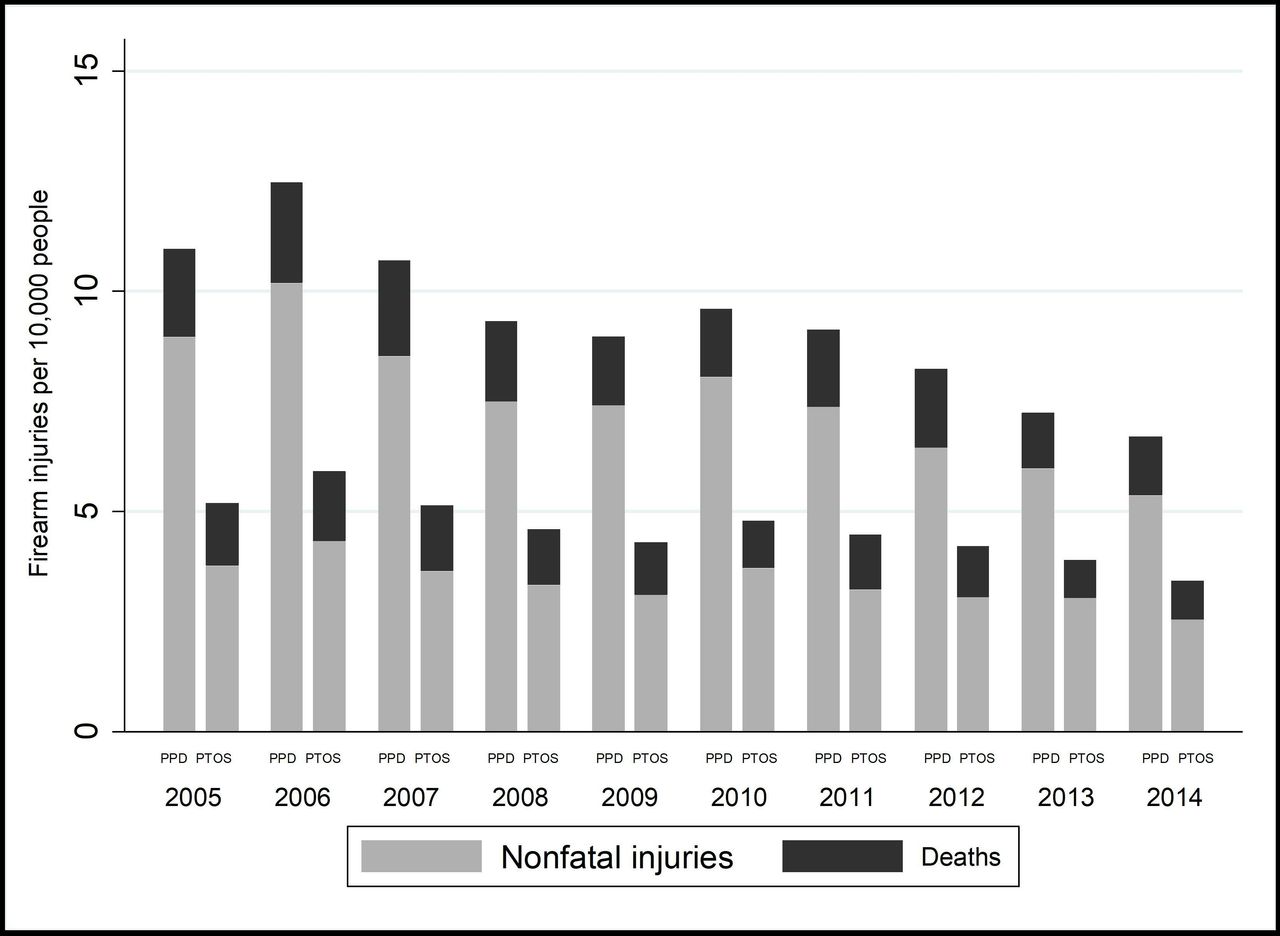
The mean case-fatality rate for PTOS patients was 26.5% and decreased significantly during the study period (change per year: −0.41%, 95% CI −0.78% to −0.04%). The PPD mean case-fatality rate was 18.9% and there was no significant change in firearm assault mortality during the study period (p=0.41) (figure 2). Figure 3 shows the annual rates of fatal and non-fatal injury represented in both data sources.

Firearm assault case-fatality rates in Philadelphia Police Department (PPD) versus Pennsylvania Trauma Outcomes Study (PTOS) data, 2005–2014.
{kind=link}
{kind=link}
{kind=link}
Fatal and non-fatal firearm injury rates in Philadelphia Police Department (PPD) versus Pennsylvania Trauma Outcomes Study (PTOS) data, 2005–2014.
According to the hospital destinations listed by the PPD, 87% of patients went to a Pennsylvania trauma center (PTOS participant) and 5% went to a non-trauma center, as shown in table 1. Among the 8.2% who were not taken to any hospital, 75.8% died (compared with 18.9% overall). Table 2 shows the demographic characteristics and injury locations according to the two data sources. In PPD data, the highest rate of mortality was in patients with injuries to the head and neck (48.9%), followed by those with multiple injuries (32.6% mortality) and torso injuries (21.8% mortality). Those noted to have extremity injuries had a 0.6% mortality rate. Proportions were similar in PTOS data: 45.1% of patients with injuries to the head or neck died, as did 34.0% of patients with torso injuries and 33.7% of patients with multiple injuries. In PTOS data, 23.1% of patients with extremity injuries died, but 98.3% of this group had additional injuries to other body regions, most commonly to the torso (90.0%) and head (48.5%).
Hospital destinations for firearm assault victims listed in Philadelphia Police Department database
Characteristics of firearm assault victims
Discussion
Our analysis of Pennsylvania’s trauma registry data identified only half as many firearm assaults in Philadelphia over a 10-year period and overestimated the case-fatality rate relative to police data. Subject demographics were slightly different across the data sets. We found a decrease in firearm assault incidence in both data sets, although the rate of decrease was lower in the PTOS data. Temporal trends in case-fatality rates differed significantly between the data sets. A possible explanation of our results is that although trauma care for firearm injuries may be improving slightly for hospitalized patients, the overall severity of injury is increasing.
PTOS and PPD data sets measure different phenomena. Although there is no gold standard against which we can verify either data source, in the absence of a single, comprehensive data source covering all gunshot wound injuries and deaths, these two types of data can be used in parallel to provide a more complete understanding of the epidemiology of firearm injury. PPD data contain all shooting victims identified by police, regardless of severity of injury. Because healthcare providers are mandated to report gunshot injuries to the police, we assume that PPD data include all individuals represented in PTOS. However, PPD data also include injuries too minor to require medical care; injuries treated at non-trauma hospitals; injuries treated at trauma centers but not meeting registry inclusion criteria; and deaths on the scene. There may still be people injured by firearms who do not come to police or healthcare attention who are not included in either data set.
Hospital destinations as listed by PPD indicate that 87% of patients were taken to a Pennsylvania trauma center that participates in PTOS, whereas only 4.9% were taken to non-trauma centers. Of the 8.2% who were not transported to any hospital, 76% had fatal injuries, likely deaths at the scene. This suggests that the primary sources of non-inclusion in PTOS were minor injuries treated at trauma centers but not meeting registry criteria. The number of patients in this category was much larger than the number who apparently died at the scene, contributing to the lower case-fatality rates in PPD data.
Patient demographics were similar between the two data sources, as were regions of injury. However, PTOS contains rich clinical detail that is not represented in PPD and therefore has greater potential to contribute to the understanding of injury severity, treatment, and outcomes. Moreover, PTOS data are verified by trained registrars, whereas PPD data are abstracted from police reports without additional verification. Without the rigorous structure of the PTOS clinical registry, risk of misclassification of non-assault or non-firearm injury may be greater. PPD data are likely to give a more accurate view of firearm injury epidemiology and changes over time, although without the clinical depth of PTOS. These data are available publicly and updated daily.
Investigators should be aware of the specific population each data set captures when designing and analyzing studies on firearm injury. Trauma registry data must be used with caution in evaluating epidemiologic trends or effects of firearm policy going forward.
Because we analyzed only two data sources from a single city, our study has limited generalizability. However, PTOS inclusion criteria are similar to those for the American College of Surgeons’ National Trauma Data Bank (NTDB), a widely used, national compilation of registry data from participating trauma centers. NTDB includes all traumatic injury resulting in death, transfer from another hospital, or hospital admission, although individual trauma centers are allowed to define admission according to their own standards.18 In addition, it is possible that the PPD data set omitted or misattributed some cases of firearm injury or contains inherent bias we are unable to measure. We did not include unintentional and self-inflicted injuries in this analysis as they were not included in the PPD data set of firearm assaults. All transfers-in were included in the PTOS data set, which may have resulted in duplication of cases. Moreover, there may be firearm injuries that never come to medical or police attention and cannot be included in either data source. Therefore our findings do not represent a comprehensive epidemiologic picture of all types of firearm injury in Philadelphia. Additionally, we were not able to link firearm victims between data sources, so it is not clear precisely which patients are captured in both sources, or in one source but not the other.
The study of firearm injury epidemiology in the USA remains limited by available sources of data. Local police databases may represent important and underutilized resources for describing city-level firearm injury epidemiology.19 20 Partnerships between health systems and law enforcement, like the Cardiff Violence Prevention Program, have the potential to enhance firearm injury surveillance and identify prevention targets.21 Future research in firearm injury epidemiology should use inclusive or linked data sources, including police data, which contain information on both fatal and non-fatal injuries. A data source that includes both national and granular local data on all types of firearm injury, including geographic data, injury type and severity, outcomes, and cost, would be ideal.
Footnotes
Presented at The abstract of this article was presented at the Pennsylvania Trauma Systems Foundation Annual Conference in Harrisburg, Pennsylvania in October 2016 and at the Society for Advancement of Violence and Injury Research (SAVIR) annual conference in Ann Arbor, Michigan in September 2017.
Contributors JHB and DNH are responsible for study concept. JHB acquired the study data. JHB, EK, WPY, and DNH analyzed the data. JHB and EK drafted the article. EK, DNH, JHB, CS, MS, CNM, DJW, and WPY contributed to the critical review of the article.
Funding The Penn Injury Science Center (CDC R49 CE002474) supported the participation of CNM and SFJ.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Institutional Review Board at the University of Pennsylvania approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.