Article Text

Abstract
Background Awareness of the magnitude of contact sports-related concussions has risen exponentially in recent years. Our objective is to conduct a prospectively registered systematic review of the scientific evidence regarding interventions to prevent contact sports-related concussions.
Methods Using the Grading of Recommendations Assessment, Development, and Evaluation methodology, we performed a systematic review of the literature to answer seven population, intervention, comparator, and outcomes (PICO) questions regarding concussion education, head protective equipment, rules prohibiting high-risk activity and neck strengthening exercise for prevention of contact sports-related concussion in pediatric and adult amateur athletes. A query of MEDLINE, PubMed, Scopus, Cumulative Index of Nursing and Allied Health Literature, and Embase was performed. Letters to the editor, case reports, book chapters, and review articles were excluded, and all articles reviewed were written in English.
Results Thirty-one studies met the inclusion criteria and were applicable to our PICO questions. Conditional recommendations are made supporting preventive interventions concussion education and rules prohibiting high-risk activity for both pediatric and adult amateur athletes and neck strengthening exercise in adult amateur athletes. Strong recommendations are supported for head protective equipment in both pediatric and adult amateur athletes. Strong recommendations regarding newer football helmet technology in adult amateur athletes and rules governing the implementation of body-checking in youth ice hockey are supported.
Conclusion Despite increasing scientific attention to sports-related concussion, studies evaluating preventive interventions remain relatively sparse. This systematic review serves as a call to focus research on primary prevention strategies for sports-related concussion.
Level of evidence IV.
PROSPERO registration number #42016043019.
- Brain Concussion
- mild traumatic brain injury
- athletic injuries
- injury prevention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Concussion in sports has come to the forefront of both scientific and public awareness, manifested by the exponential increase in research from less than 100 articles published annually during the 1980s to over 900 during 2016.1 Concomitantly, numerous evidence-based guidelines have been generated,2–7 focusing on topics such as sideline assessment, diagnostic evaluation, management, and prevention of secondary concussion.
A major tenet of modern trauma care is primary prevention of injury. However, as it relates to sports-related concussion, interventions promoted in existing guidelines have not been critically examined for efficacy. A recent, comprehensive systematic review and meta-analysis published in 2017 by Emery et al 8 added significantly to the body of knowledge on this topic. Our goals were to complement this work using the validated Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology to create specific a priori questions, limit our literature review to publications which meet predefined criteria, and develop recommendations for practitioners.
Our objective was to systematically evaluate the scientific evidence regarding preventive interventions promoted in existing guidelines, such as protective headgear, concussion education, neck mass exercise, and rule modification for pediatric and adult amateur athletes. We focused on two distinct populations in whom the issue of concussion prevention is relevant: pediatric athletes (age 14 or younger) and adult amateur athletes (non-professionals aged 15 years and older), maintaining the results broadly applicable to the general population. Our single, critical outcome was the incidence of contact sports-related concussion.
PICO questions
PICO 1: In pediatric athletes, should players, parents, and coaches receive concussion education (vs no such education) to reduce the incidence of sports-related concussion?
PICO 2: In adult amateur athletes, should players and coaches receive concussion education (vs no such education) to reduce the incidence of sports-related concussion?
PICO 3: In pediatric athletes, should a particular type of head protective equipment be worn to reduce the incidence of sports-related concussion?
PICO 4: In adult amateur athletes, should a particular type of head protective equipment be worn to reduce the incidence of sports-related concussion?
PICO 5: For pediatric athletes, should rule modifications governing high-risk activity (vs no such activity restriction) be instituted to reduce the incidence of sports-related concussion?
PICO 6: For adult amateur athletes, should rule modifications governing high-risk activity (vs no such activity restriction) be instituted to reduce the incidence of sports-related concussion?
PICO 7: In adult amateur athletes, should exercises to increase neck mass be performed (vs no such directed exercise) to reduce the incidence of sports-related concussion?
Methods
A workgroup from the Injury Control and Violence Prevention Committee of the Eastern Association for the Surgery of Trauma (EAST) conducted a systematic review of the evidence addressing prevention of contact sports-related concussions.
Our seven questions were formulated a priori in the PICO format (patient population, intervention, comparator, and outcome) per the GRADE methodology9 10 over three rounds using a modified Delphi method. This systematic review was prospectively registered with PROSPERO (#42016043019).
Identification of references
The literature search was performed by a university-affiliated research librarian. A preliminary query revealed no pertinent articles prior to 1985. Therefore, a comprehensive search of the literature from January 1, 1985 to November 30, 2017 was conducted using MEDLINE, PubMed, Scopus, Cumulative Index of Nursing and Allied Health Literature, and Embase (online supplementary appendix A). The references of all publications directly addressing prevention of sports-related concussion were reviewed to identify additional potentially pertinent articles.
Supplemental material
Inclusion and exclusion criteria for systematic review
Studies were included if they reported original data, were published in English, and evaluated the relationship between the designated interventions and contact sports-related concussion. Articles containing no original data, expert opinion only, or evaluating non-contact-sports-related concussions were excluded. No unpublished data were reviewed. In instances of disagreement on inclusion, thorough discussion of each viewpoint occurred and the final consensus was followed. There were no studies for which a consensus was not reached.
Data extraction
All studies were reviewed by each member of a subgroup consisting of five to six members dedicated to a specific PICO question. Extracted data included study methodology, intervention, and outcome measures. Discrepancies in extracted data were resolved by the primary author.
Results
The search returned 1053 references. Titles were screened for relevance, identifying 37 potentially pertinent articles. The references of these articles were reviewed, identifying 106 additional potentially pertinent articles. Abstracts for these 143 articles were reviewed by the working group, narrowing articles for full-text review to 54. Subgroups then undertook a detailed review of all articles relevant to individual PICO questions, identifying 31 articles for inclusion (figure 1). These include three randomized control trials, all of which contain significant methodologic flaws. The remaining 28 studies were uncontrolled retrospective cohort or prospective observational studies. The number of pertinent studies per PICO question ranged from 1 study evaluating concussion education in adult amateur athletes to 14 studies evaluating various aspects of head protective equipment in adult amateur athletes.

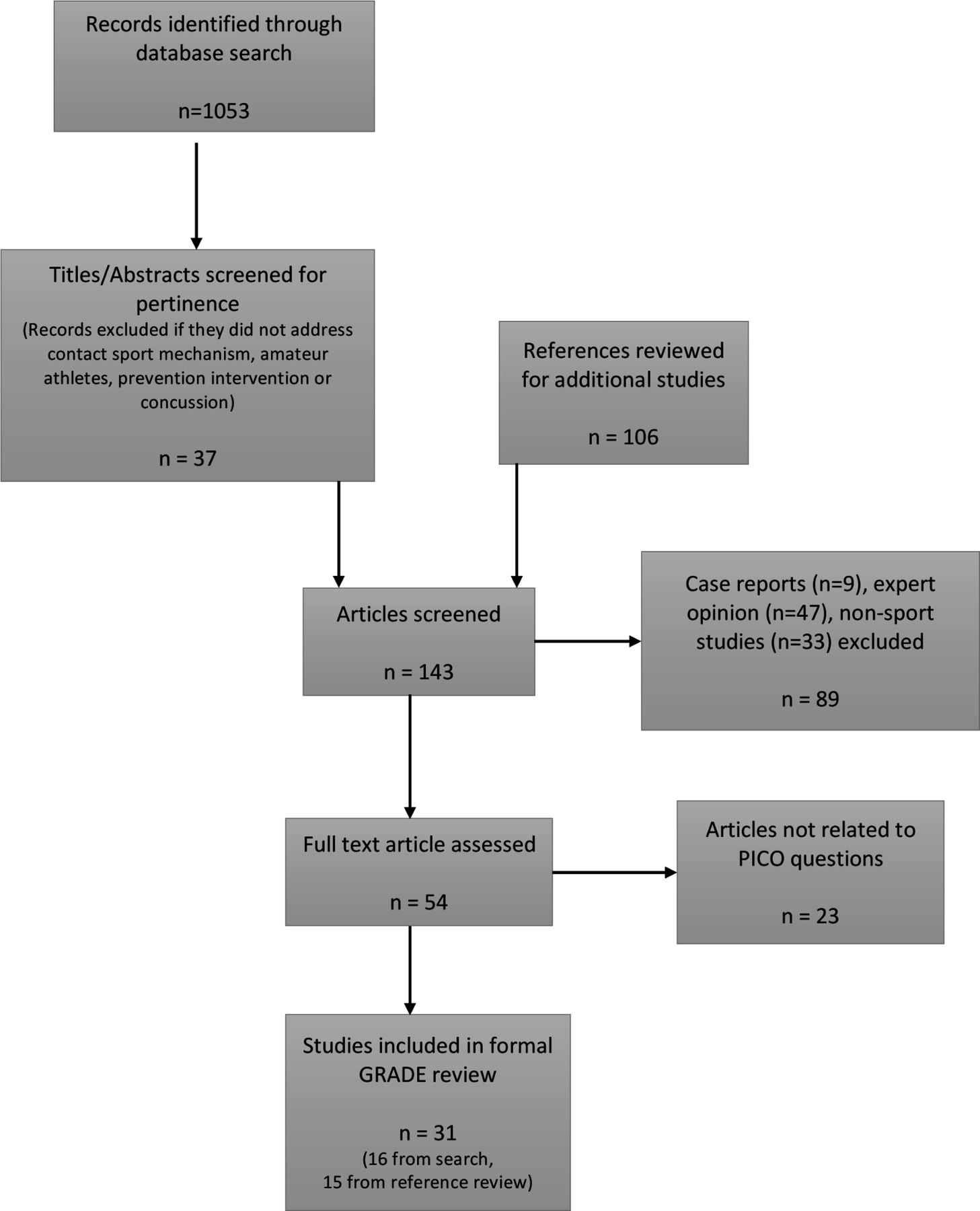{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram. GRADE, Grading of Recommendations Assessment, Development, and Evaluation; PICO, population,intervention, comparator, and outcomes.
Quality assessment
Each reviewer independently evaluated article quality with regard to study design, risk of bias, inconsistency, indirectness, imprecision, publication bias, size of effect, dose response, and minimization of confounding variables as per the GRADE methodology.11
Table 1 summarizes the design, outcome and quality results of the systematic review.
Strength of evidence for primary prevention of sports-related concussion
Discussion
Formulation of recommendations
In formulating recommendations, the GRADE methodology identifies four factors that contribute to the strength of a recommendation: quality of the evidence, balance between desirable and undesirable effects of intervention, values and preferences of the population, and cost of intervention.12 A strong recommendation is made if, in considering these four factors, most people to whom the recommendation would apply would want the recommended intervention and only a small proportion would not, whereas a conditional recommendation is given if many people would want the recommended intervention but many would not.
Concussion education in pediatric athletes (PICO 1)
Concussion education has been suggested as a primary preventive intervention13 14 and several programs have been developed, such as the Centers for Disease Control and Prevention’s (CDC) ‘HEADS UP’ program.15 16 Presently, all 50 states and the District of Columbia have some form of youth sports concussion law, many mandating concussion education.
Our review identified four studies evaluating education programs in pediatric athletics. Cook et al 17 demonstrated a significant reduction in the high-risk activities of cross-checking and checking from behind among hockey players after one mid-season showing of ‘Smart Hockey’ by the ThinkFirst Foundation of Canada. Covassin et al 18 demonstrated improved attitude toward and ability to identify concussion among youth coaches after use of the CDC’s ‘HEADS UP’ program but did not evaluate impact on concussion incidence. Cusimano et al 19 found that hockey players who viewed the educational video ‘Smart Hockey’ demonstrated an increase in concussion-specific knowledge but found no significant change in behavior or aggression. Kerr et al 20 demonstrated a significant reduction in risk of concussion during practice but not in overall rate of concussion with implementation of the USA Football program ‘Heads Up Football’ in youth football.
The increased awareness and knowledge among athletes, parents, and coaches and the possible decrease in high-risk activities are desirable effects of concussion education programs. Undesirable effects of implementing a concussion education program would be minimal and would include time taken away from practice and inattention among athletes for an activity not involving participation in the sport. Considering these factors, the consensus is that many involved in pediatric athletics would choose a concussion education program versus no formal education as a strategy for the primary prevention of concussion, although many may not.
Recommendation: Conditional recommendation for concussion education as a primary preventive intervention against concussion in pediatric athletes.
Concussion education in adult amateur athletes (PICO 2)
One study was found which considered athletes 15 years of age or older. Kerr et al 21 demonstrated a significant reduction in risk of concussion using the ‘Heads Up’ program in high school football.
The additional factors discussed for pediatric athletes would also apply to adult amateur athletes. Our consensus is that many adult amateur athletes would choose a concussion education program versus no formal education as an intervention for the primary prevention of concussion, although many may not.
Recommendation: Conditional recommendation for concussion education as a primary preventive intervention against concussion in adult amateur athletes.
Head protective equipment in pediatric athletes (PICO 3)
For primary concussion prevention, the most intuitive strategy would be protective headgear. Helmets are effective in decreasing the incidence of severe head trauma in bicyclists22 23 and recreational skiers and snowboarders.24–26 There also exists evidence suggesting a decreased risk of concussion among recreational bicyclists with the use of protective helmets.27
Our review found three studies evaluating padded headgear use in pediatric contact sports. All three included athletes over 14 years of age in their analysis.
McIntosh and McCrory28 compared the use of padded headgear versus none in rugby and found no difference in concussion incidence, possibly influenced by a high rate of non-compliance with randomization. McIntosh et al 29 randomized rugby players to wear standard thickness headgear (10 mm thick padding), modified headgear (16 mm thick padding), or no headgear, again with substantial non-compliance among subjects. Analysis, per protocol and by intention-to-treat, demonstrated no difference in concussion incidence.
Delaney et al 30 surveyed soccer players to evaluate the correlation of padded headgear use with self-reported symptoms of concussion, arguably an indirect and imprecise measure, and found a relative risk (RR) of 2.65 in players not wearing headgear (p<0.0001).
The desirable effects of definite reduction in severe head injury in athletic and recreational activities22–26 and literature suggesting a similar effect for concussion compare very favorably with the undesirable effects of increased cost of equipment and a possible negative impact on athletic performance. The acceptance of head protective equipment in a wide variety of activities reflects the value placed on injury prevention by the general population. The balance of these factors would lead to the conclusion that most pediatric athletes and their parents would want to use head protective equipment as primary prevention of concussion, and only a small proportion would not.
Recommendation: Strong recommendation for head protective equipment as a primary preventive intervention against concussion in pediatric athletes.
Head protective equipment in adult amateur athletes (PICO 4)
Protective headgear reduces the risk of severe head injuries in adult athletes22 23 as well as in recreational winter sports.24 26 31 A trend toward decrease in mild traumatic brain injury in rugby players wearing headgear has been suggested.32 Our review yielded 14 studies evaluating head protective equipment and concussion in adult amateur athletes engaging in contact sports.
The three studies discussed in PICO 3 included athletes older than 14, but did not separate out data based on age.28–30
Zemper33 in 1989 evaluated concussion incidence relative to the brand of helmet in college football and identified no significant difference. A later study by Zemper34 in 1994 compared concussion rates for 10 models of collegiate football helmets over a longer time frame. Two models were shown to have a higher than expected rate of concussion and one model to have a lower than expected rate. The outlier models were not identified and there was no discussion of what might account for the difference.
Historically, impacts in laboratory helmet testing were not allowed to be delivered distal to the basic plane of the head (the plane defined by the external auditory meatus and inferior orbital notch). In 2003, it was demonstrated that 36% of live impacts resulting in concussion occurred distal to this plane.35 This led to change in helmet design in which the exterior shell was extended distally over the zygoma and mandible with increased padding beneath the shell. Collins et al 36 found a significant decrease in concussion incidence with this newer helmet technology compared with the older design, 5.3% versus 7.6% (p<0.027), representing a 31% decrease in risk (RR=0.69).Risk reduction was also observed in the subgroup with no prior concussion, 3.7% versus 6.2% (p<0.009) with a relative risk of 0.59. Rowson et al 37 similarly demonstrated a risk reduction of 0.46 (0.28–0.76) when comparing the newer with older design in collegiate football.
Benson et al 38 in 1999 showed no difference in concussion risk but identified increased concussion severity, defined as playing time lost due to concussion, associated with half versus full face shields in collegiate hockey. Benson et al 39 later in 2002 demonstrated no difference in incidence of concussion, but increased playing time missed for concussions associated with half face shields. This remained significant when comparing game versus practice, forward versus defense positions, new versus recurrent concussion, and rookie versus veteran experience level. The authors concluded that the severity of concussion is significantly greater with half versus full face shields.
Stuart et al 40 evaluated the impact of no versus half versus full face shields in adult amateur hockey players, finding incidences of concussion of 12.2, 8.2 and 2.9 per 100 player hours, respectively (p=0.11).
Marshall et al 41 investigated injury prevention effectiveness of padded headgear and mouth guards in rugby players and demonstrated no protective effect of either against concussion.
McGuine et al 42 found no difference in concussion incidence between helmet brands in high school football. Collins e t al 43 demonstrated a non-significant difference between helmet brands and no significant difference in the rate of concussion between new and recertified football helmets.In evaluating helmet liners, Greenhill et al 44 demonstrated increased rate and severity of concussion for air bladder compared with foam or gel liners in high school football.
Consideration of factors similar to the discussion for pediatric athletes together with the more definitive demonstration of the benefit of head protective equipment in adults led us to conclude that most adult amateur athletes would want to use head protective equipment as a primary preventive intervention against concussion, and only a small proportion would not.
Recommendation: Strong recommendation for head protective equipment as a primary preventive strategy against concussion in adult amateur athletes. The evidence also supports a specific strong recommendation for newer football helmet technology as an effective strategy for the primary prevention of concussion in adult amateur football players.
High-risk activity regulation in pediatric athletes (PICO 5)
The most common cause of concussion in sports is player-to-player contact.45 Rule changes have been implemented to prohibit certain high-risk forms of contact, such as helmet-to-helmet tackling in football, allowable player-to-player contact in soccer, and specific forms of checking in ice hockey. The Consensus Statement on Concussion in Sport from the Fourth International Conference on Concussion in Sport states that ‘rule enforcement may be a critical aspect of modifying injury risk’.7 Our search of the literature revealed 10 articles addressing rule changes and incidence of concussion in pediatric athletes.
In the 1990s, several instances of rule changes occurred lowering the age at which body-checking was permitted. These changes were partially based on the argument that learning proper technique to deliver and receive contact would lead to reduced injuries at older ages. Cusimano et al 46 in 2011 evaluated injuries before and after the rule change. The odds of sustaining a body-checking injury increased for all age groups, except for the most novice group, which was not impacted by the rule change. Specifically, it was shown that the odds ratio (OR) for concussion was 10.08 (2.35–43.29, p=0.01) for the age group that had gone from prohibiting to allowing body-checking. The OR for all older age groups was not significant, arguing against a reduced risk of concussion for older groups when body-checking is introduced at an earlier age.
Emery and Meeuwisse47in 2006 demonstrated an increased risk of concussion in leagues which permit body-checking in younger age groups. Subgroup analysis based on age showed the age group for which checking is first allowed had a non-significant RR of 3.4 (0.93–18.61), but significant increases were observed for players aged 13 to 14 years old, with RR=4.04 (1.17–21.54), and those aged 15 to 16 years old, with RR=3.41 (1.02–17.87).
Emery et al 48 in 2010 examined the risk of concussion in players aged 11 to 12 years old compared between leagues that did and did not allow body-checking and found an increased incidence rate ratio (IRR) for concussion of 3.88 (1.91–7.89) when body-checking was allowed.
Emery et al 49 in 2011 evaluated whether earlier experience with body-checking impacted the risk of concussion, comparing players aged 13 to 14 years old being exposed to checking for the first time against players of the same age who carried 2 years of exposure to checking and found the risk of concussion was not significantly different: IRR=0.87 (0.51–1.50).
Hagel et al 50 evaluated risk of concussion for athletes aged 10 to 12 years old before and after the age of introduction of checking was lowered from 12 to 11. They found a significantly higher risk for concussion in athletes aged 11 years old, with RR=3.4 (1.4–8.4), but no difference in risk for players aged 10 or 12 years old.
A similar study by MacPherson et al 51 compared the risk of concussion in the 11-year-old groups in which body-checking was allowed or prohibited and also evaluated the risk among players aged 14 to 15 years old based on the extent of prior experience with body-checking. It revealed a trend toward increased risk for concussion in players aged 11 years old, with an OR=1.42 (0.98–2.05), and no difference in risk for the older group, with OR=1.6 (0.68–3.81).
Black et al 52 in 2016 demonstrated an increased risk of concussion when body-checking is allowed in youth hockey, IRR=2.83 (1.09–7.31). Black et al 53 in 2017 then compared the year before with the year after implementation of rules prohibiting body-checking in a youth hockey league and demonstrated a significant reduction in concussion risk, IRR=0.34 (0.21–0.56).
Krolikowski et al 54 found that a policy of zero tolerance for head contact did not significantly reduce the risk of concussion in youth hockey. Smith et al 55 found that Fair Play systems, which incorporate sportsmanship and penalties into youth hockey game results, did not decrease the incidence of concussion.
These results demonstrate an increased incidence of concussion associated with body-checking at younger ages and do not support the assertion that earlier introduction translates into decreased risk with increasing experience. A reduction in risk of injury would be a desirable effect of intervention. Potential undesirable effects include negative impact on the perceived quality of competition, disruption of the flow of competition caused by increasing rule infractions, and altering the culture of the game.
Recommendation: Conditional recommendation for rules governing high-risk activity as a primary preventive intervention against concussion in adult amateur athletes. Given the strength of the evidence of the association between body-checking and concussion risk, we also strongly recommend rules that prohibit body-checking at a younger age in ice hockey as an effective intervention for the primary prevention of concussion in pediatric athletes.
High-risk activity prohibition in adult amateur athletes (PICO 6)
In high school athletics 6.4% of injuries are related to prohibited activities. Of injuries caused by prohibited activity, concussion accounts for 25.4%.56 In hockey, rule modifications have been shown to decrease overall injury rate.57 A search of the literature revealed three studies that address rule modification and concussion.
Emery and Meeuwisse47 compared athletes aged 15 to 16 years old for whom body-checking was allowed with those aged 9 to 10 years old for whom body-checking was prohibited, finding a significantly increased relative risk for concussion in the body-checking group, RR=3.41 (1.02–17.87). Cusimano e t al 46 in 2011 evaluated the risk of concussion based on age at which checking is introduced. For the age group 15 to 17 years old, the OR for body-checking-related concussion was not statistically significant at 1.31 (0.44–3.88), leading them to conclude that the risk of concussion at older ages was not associated with the age at which body-checking may be introduced.
A rule implemented in 2001 by the National Rugby League of Australia limited the number of player exchanges that occurred during professional play. This was associated with a lower incidence of injury, which was theorized to be due to decreased aggression in players competing in a more fatigued state.58 Gabbett59 investigated the incidence of concussion in amateur players after the introduction of a similar rule change. A significant decrease was demonstrated in overall risk of injury, with RR=0.70 (0.65–0.75); however, there was no difference in the risk for a composite concussion/open wound variable.As in the discussion of relevant factors for pediatric athletes, many adult amateur athletes would want rules regulating high-risk behavior as an intervention for the primary prevention of concussion, and many would not.
Recommendation: Conditional recommendation for rules governing high-risk activity as a primary preventive intervention against concussion in adult amateur athletes.
Neck mass exercises in adult amateur athletes (PICO 7)
Traumatic brain injury, including concussion, is due to linear and rotational acceleration of the head.60 Cervical muscle contraction is theorized to more rigidly couple the head to the torso, increasing the overall mass being subjected to a force and decreasing the acceleration experienced by the brain.61 62 This theoretical protective mechanism is the basis for exercise to increase neck mass as a preventive strategy to reduce concussion. Several studies have evaluated the relation between neck strength and acceleration in the laboratory,63–66 but did not directly evaluate the impact on incidence of concussion. Only one study was found that evaluated the correlation between neck strength and concussion.
Collins et al 67 compared preseason neck strength measurements in 6704 high school athletes in various sports between athletes who did and did not experience concussion over two academic years. They found significantly lower neck circumference, lower neck to head circumference ratio, and lower mean overall neck strength in athletes who suffered concussions (p<0.001).No evaluation was made of the impact of neck strengthening on concussion incidence. In consideration of increasing neck strength as an intervention for the primary prevention of concussion, many adult amateur athletes would consider it an acceptable intervention.
Recommendation: Conditional recommendation for neck strengthening exercise program as a primary preventive intervention against concussion in adult amateur athletes.
Table 2 summarizes the recommendations for the seven PICO questions.
EAST evidence-based recommendations for the primary prevention of contact sports-related concussions
Limitations
In the GRADE methodology, the literature is one of four factors considered in formulating recommendations.12 Recommendations formulated in this review are primarily limited by the relative scarcity and quality of existing evidence. They serve as the rudimentary foundation for athletes, coaches, governing bodies, and injury prevention/outreach programs to formulate an evidence-based approach to concussion prevention. They also serve to augment existing guidelines addressing diagnosis and management of contact sport-related concussion. But primarily, this systematic review serves as a call for increased scientific focus on identifying and more clearly defining effective primary prevention strategies.
Conclusion
In summary, this represents the first systematic review of the literature pertaining to the primary prevention of sports-related concussion. EAST applauds the advances that have been made in the evidence guiding the diagnosis and management of mild traumatic brain injury-related to sports. However, our greatest opportunity to impact overall injury burden often lies in injury prevention. Future research will serve to more granularly define effective interventions to prevent sports-related concussion in pediatric and adult amateur athletes.
References
Footnotes
Presented at Interim progress delivered as podium presentation at the 29th Eastern Association for the Surgery of Trauma Annual Scientific Assembly, San Antonio, Texas, January 12-16, 2016.
Contributors KB, NB, JC, MC, OKD, TD, TME, GH, HSJ, and FL contributed to project design and PICO question formulation. TME performed literature search. KB, BB, NB, JC, MC, OKD, TD, TME, SF, GH, HSJ, FL, and PV performed reference review to identify additional studies. KB, BB, NB, JC, MC, OKD, TD, TME, SF, GH, HSJ, FL, and PV performed literature review and data extraction. KB, BB, NB, JC, MC, OKD, TD, TME, SF, GH, HSJ, FL, RR, and PV interpreted the results and formulated the recommendations. KB, BB, NB, JC, MC, OKD, TD, TME, SF, GH, HSJ, FL, RR, and PV contributed to drafting and critical revision of the article. This article has already undergone revision through a blind review process by the Practice Management Guideline Committee of the Eastern Association for the Surgery of Trauma.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data associated with this systematic review.