- Correspondence to Dr Peter C Jenkins, Department of Surgery, Indiana University School of Medicine, Indianapolis, IN 46202, USA; pjenkins1{at}iuhealth.org
- Received 23 May 2017
- Revised 28 September 2017
- Accepted 29 September 2017
Abstract
Background Several hemodynamic parameters have been promoted to help establish a rapid diagnosis of hemorrhagic shock, but they have not been well validated in the pregnant population. In this study, we examined the association between three measures of shock and early blood transfusion requirements among pregnant trauma patients.
Methods This study included 81 pregnant trauma patients admitted to a level 1 trauma center (2010–2015). In separate logistic regression models, we tested the relationship between exposure variables—initial systolic blood pressure (SBP), shock index (SI), and rate over pressure evaluation (ROPE)—and the outcome of transfusion of blood products within 24 hours of admission. To test the predictive ability of each measure, we used receiver operating characteristic (ROC) curves.
Results A total of 10% of patients received blood products in the patient cohort. No patients had an initial SBP≤90, so the SBP measure was excluded from analysis. We found that patients with SI>1 were significantly more likely to receive blood transfusions compared with patients with SI<1 (OR 10.35; 95% CI 1.80 to 59.62), whereas ROPE>3 was not associated with blood transfusion compared with ROPE≤3 (OR 2.92; 95% CI 0.28 to 30.42). Furthermore, comparison of area under the ROC curve for SI (0.68) and ROPE (0.54) suggested that SI was more predictive than ROPE of blood transfusion.
Conclusion We found that an elevated SI was more closely associated with early blood product transfusion than SBP and ROPE in injured pregnant patients.
Level of evidence Prognostic, level III
- pregnancy
- shock management
- hemorrahgic shock
Introduction
Hemorrhagic shock accounts for up to 40% of all trauma mortality, making it the foremost cause of preventable death among injured patients.1–4 Hypotension, defined as a systolic blood pressure (SBP) ≤90 mm Hg, has been widely used to identify patients with hemorrhagic shock.5 6 However, hypotension secondary to hemorrhage is a late finding that occurs only after considerable blood loss has occurred. In an effort to promote more prompt recognition and treatment of hemorrhagic shock, recent studies have examined the use of alternative hemodynamic parameters. Two alternative measures, the shock index (SI), defined as heart rate divided by SBP, and the pulse rate over pressure evaluation (ROPE), defined as heart rate divided by pulse pressure, have been found to be more sensitive than SBP alone for the detection of acute blood loss.7 8 These measures, however, have not been well validated in the injured obstetric population.2
Recognition of hemorrhage in obstetric patients is complicated by the normal physiological changes that occur during pregnancy. Mean blood pressure usually decreases 4 to 6 weeks after conception, primarily due to maternal systemic vasodilation and, to a lesser extent, from the high-flow, low-resistance circuit in the uteroplacental circulation. Later in pregnancy, during the second trimester, blood pressure tends to increase to normal levels.2 In addition to hemodynamic changes in vascular tone and resistance, circulating blood volume increases by as much as 40% to 50% above non-pregnant volumes, further confounding the diagnosis of acute hemorrhage.9 Therefore, based on the current body of evidence, it remains unclear how physiological changes influence the hemodynamic parameters that clinicians use to detect occult hemorrhage in obstetric patients.
In this study, we examined the relationship between three hemodynamic parameters—SBP, SI, and ROPE—and traumatic hemorrhage among injured pregnant patients. Our goal was to analyze which measure best predicted the need for transfusion of blood products in the early post-trauma period.
Methods
The study is designed as a retrospective case–control study, using trauma registry data from a single institution.
Data source and study population
We performed a retrospective cohort study of all pregnant trauma patients admitted to a level 1 trauma center between January 2010 and January 2015. First, we identified all trauma patients entered in the hospital trauma registry. Trauma registry inclusion criteria included an International Classification of Diseases, Ninth Revision (ICD-9) injury code (800–959.9) and hospital admission ≥24 hours. Exclusion criteria included injuries more than 30 days old, admission to undergo an elective procedure, patients admitted for reasons other than their injuries and minimal injuries, with an abbreviated injury score of 1.
Using the medical record number of each patient with trauma in the trauma registry, we queried the hospital administrative data using the electronic medical record system to identify patients with the ICD-9 diagnosis codes for pregnancy, 630–679.14 or V22.0–V23.9. Once pregnant trauma patients were identified, a chart review was performed for each patient to verify diagnoses and determine gestational age by trimester.
Analysis
Descriptive analyses compared demographic and clinical characteristics of patients who received a blood transfusion with those who did not receive a blood transfusion using Χ2 and Student’s t-tests. All tests were two tailed with α=0.05. We initially examined the relationship between clinical parameters of hemodynamic stability and hemorrhagic shock using unadjusted logistic regression models. Continuous hemodynamic variables were converted to dichotomous variables with cut-off points based on previously published work on transfusion requirements and physiological derangement: SBP≤90, SI≥1, and pulse ROPE>3.10 We used the outcome of transfusion of blood products within 24 hours as a surrogate for the diagnosis of hemorrhagic shock. After performing unadjusted analysis, we included trimester as a covariate in the regression models. We then examined the effect of gestational age on the hemodynamic parameters by testing for interaction effect between each parameter and gestational trimester. We generated receiver operating characteristic (ROC) curves to examine the predictive ability of the primary exposure variables alone to determine transfusion requirement.
To better characterize the patient population, we performed a chart review of all patients. We identified baseline hemoglobin levels and calculated the change in hemoglobin documented within the first 24 hours period after admission. We compared those values between the transfusion and non-transfusion cohorts using Student’s t-tests. Finally, we identified injury patterns and sources of blood loss among patients who received transfusions.
Results
During the study period, 18 438 patients were entered into the trauma registry, and 83 of those patients had ICD-9 codes indicating pregnancy. Subsequent chart review revealed that two of the patients were postpartum, leaving 81 patients in the study cohort. Eight patients (10%) were transfused blood products within the first 24 hours of hospital admission. Table 1 depicts patient and injury characteristics. Of note, no statistical differences in mechanism of injury, gestational age, and baseline hemoglobin level existed between the two cohorts. However, the transfusion cohort demonstrated a greater decrease in hemoglobin level and a significantly higher injury severity score (p<0.001).
Patient characteristics (n=81)
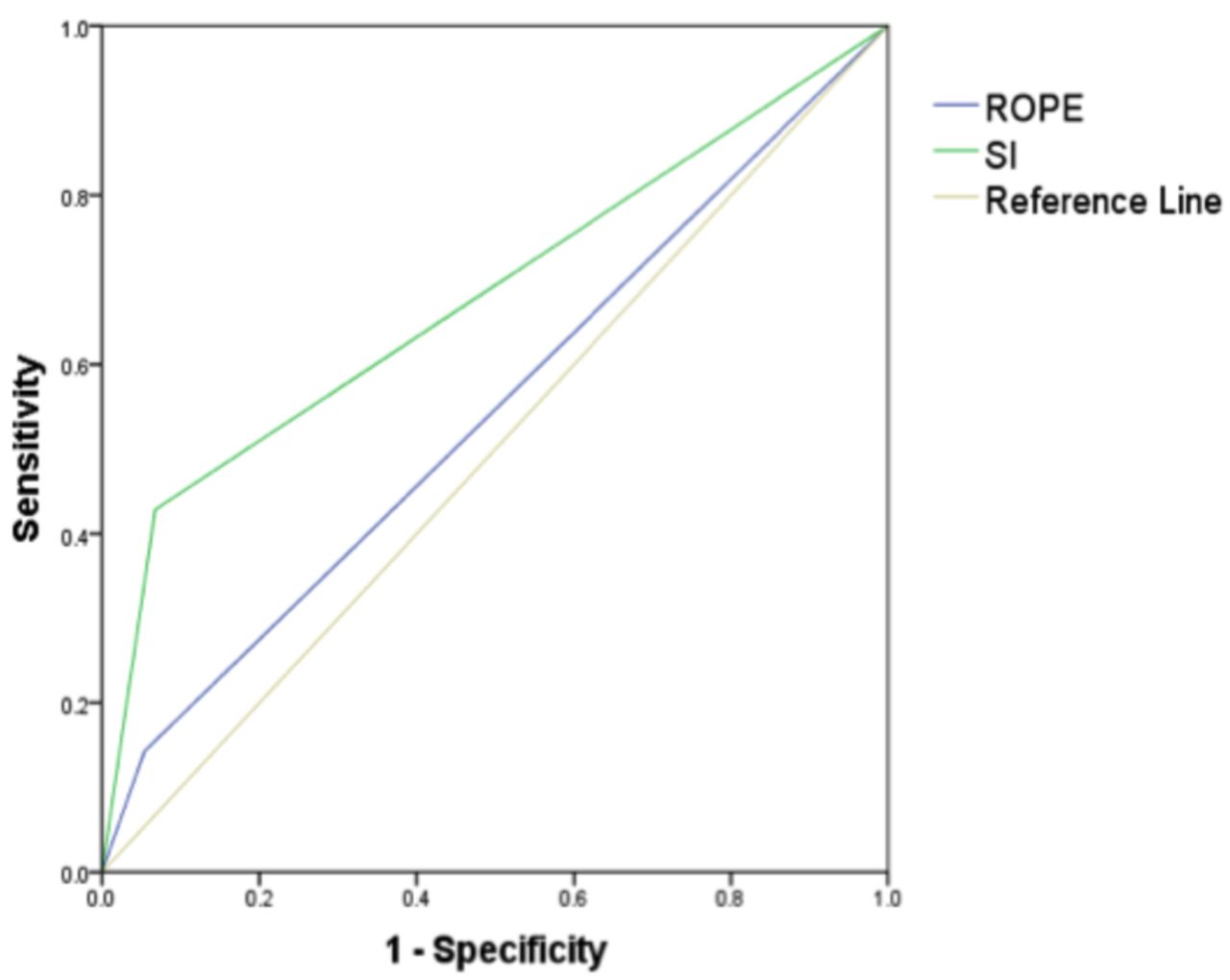
We found that no patients presented with an initial SBP<90 and therefore excluded the measure from further analysis. SI>1 was significantly more likely to receive blood transfusions compared with SI<1 (OR 10.35; 95% CI 1.80 to 59.62). However, the ROPE>3 had no significant association with blood transfusion compared with ROPE<3 (OR 2.92; 95% CI 0.28 to 30.42). During multivariable logistic regression, trimester had no significant influence on the outcome or were any significant interactions detected between trimester and the three measures of shock. Finally, the area under the ROC curve for SI and ROPE was 0.68 and 0.54, respectively, suggesting that SI was more predictive than ROPE of receiving a blood transfusion (figure 1).
{kind=link}
Comparison of area under the receiver operating characteristic curves for shock index (SI) and rate over pressure evaluation (ROPE), n=81.
We observed considerable variation in injury patterns and sources of blood loss among patients who received transfusions. All but one of the patients had multiple documented injuries. One patient had a knee dislocation that, on reduction, required lower extremity vascular bypass to re-establish perfusion and fasciotomies; four patients had solid organ injuries (grade III–V) as well as an intrauterine fetal demise requiring laparotomy in one patient; two patients had considerable orthopedic injuries (pelvic and femur); and one patient experienced chest trauma resulting in acute respiratory distress syndrome, requiring extracorporeal membrane oxygenation.
Discussion
Hemorrhagic shock is the foremost cause of preventable death among injured patients, and early recognition of this condition is necessary to treat it effectively. For injured obstetric patients, that diagnostic challenge is confounded by the normal physiological changes associated with pregnancy. The SI and ROPE have been promoted as alternatives to SBP alone to diagnose hemorrhagic shock in the general trauma population. However, these measures have not been well validated among injured obstetric patients.
Our results suggest that SI is more predictive of patients receiving an early blood transfusion than ROPE. Recent studies have discouraged the use of SBP alone as inadequate; however, we also found that ROPE was less predictive of blood transfusion than SI in the pregnant population. We hypothesize that among obstetric patients, ROPE is lower in non-pregnant patients, due to the vasodilation that normally occurs during early pregnancy. Of note, this study did not detect an interaction effect between gestational age and the clinical indicators, so it does not appear that SI—or either of the other two measures—is more predictive of transfusion requirement at any particular gestational age.
This study has limitations. We use transfusion of blood products as a surrogate for the existence of hemorrhagic shock. However, blood transfusion could be subject to the clinical judgment of the providers who resuscitated the patient. Therefore, transfusion of blood products may be influenced by practice variation. More objective measures of shock such as serum lactate and base deficit were not routinely drawn among our patient population, but these values could serve to both validate and enhance our findings in future studies. Second, this study lacks data regarding the prehospital care provided to our cohort. Several factors, such as the administration of intravenous fluids and analgesics, could confound our initial vital signs. Detailed clinical data, including prehospital information, would allow future studies to control for such potential confounders. Finally, this study is limited to a single institution and includes a small sample size. Multi-institutional studies are needed to validate our findings, and larger study cohorts may be able to detect an effect of trimester on clinical signs of hemorrhagic shock.
The identification of occult hemorrhagic shock in the injured obstetric patient represents a diagnostic challenge. As one may expect, we found that decreases in hemoglobin levels correlated significantly with the administration of blood products, yet such trends in hemoglobin are not readily apparent on hospital admission. Although an SI>1 alone may not prompt immediate transfusion at admission, clinicians should consider close hemodynamic monitoring for patients with this finding. This study adds to the limited body of evidence supporting the use of SI in this vulnerable patient population, and it provides the rationale for further, multi-institutional studies of this important clinical topic.
Acknowledgments
none
Footnotes
Contributors Each author has made substantial contributions to the conception, intellectual content and design of the this review; has contributed substantially to the drafting of the manuscript as well as revisions; and each author has had final approval of the manuscript version that is enclosed and is in agreement with submission to trauma surgery and acute care open.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data will be made available on request.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/