- Stacy A Drake1,
- Dwayne A Wolf2,
- Janet C Meininger1,
- Stanley G Cron3,
- Thomas Reynold4,
- Charles E Wade5,
- John B Holcomb5
- 1 Systems Department, The University of Texas Health Science Center, School of Nursing, Houston, Texas, USA
- 2 Pathology Department, Harris County Institute of Forensic Sciences, Houston, Texas, USA
- 3 Center for Research, The University of Texas Health Science Center at Houston School of Nursing, Houston, Texas, USA
- 4 Institute for Health Policy, The University of Texas Health Science Center at Houston School of Public Health, Houston, Texas, USA
- 5 Surgery Department, The University of Texas Health Science Center, McGovern School of Medicine, Houston, Texas, USA
- Correspondence to Dr Stacy A Drake, The University of Texas Health Science Center School of Nursing, 6901 Bertner Ave., #748, Houston, Texas 77054, USA; Stacy.A.Drake{at}uth.tmc.edu
- Received 3 April 2017
- Accepted 4 April 2017
Abstract
This article describes a methodology to establish a trauma preventable death rate (PDR) in a densely populated county in the USA. Harris County has >4 million residents, encompasses a geographic area of 1777 square miles and includes the City of Houston, Texas. Although attempts have been made to address a national PDR, these studies had significant methodological flaws. There is no national consensus among varying groups of clinicians for defining preventability or documenting methods by which preventability is determined. Furthermore, although trauma centers routinely evaluate deaths within their hospital for preventability, few centers compare across regions, within the prehospital arena and even fewer have evaluated trauma deaths at non-trauma centers. Comprehensive population-based data on all trauma deaths within a defined region would provide a framework for effective prevention and intervention efforts at the regional and national levels. The authors adapted a military method recently used in Southwest Asia to determine the potential preventability of civilian trauma deaths occurring across a large and diverse population. The project design will allow a data-driven approach to improve services across the entire spectrum of trauma care, from prevention through rehabilitation.
- trauma
- preventable death rate
- methods
- medicolegal autopsy
- consensus panel
Introduction
A 2016 National Academy of Science report1 focusing on decreasing the trauma preventable death rate (PDR) to zero estimated a civilian trauma PDR of 20% or about 30 000 deaths per year. Although trauma systems have long worked to improve the care of patients before, during, and after hospitalisation,2 3 traumatic injury continues to be among the top five leading causes of death in the USA4 and the leading cause of death for individuals 44 years. The World Health Organization (WHO) projects that by 2030, trauma will be the third leading cause of disability-adjusted life loss.5
To improve patient outcomes, trauma centers accredited by the American College of Surgeons are required to review all in-hospital trauma-related deaths and determine whether those deaths were preventable (P), potentially preventable (PP) or non-preventable (NP).2 ,6–9 These trauma centers must also use data to evaluate how to improve quality, safety, and medical interventions at the organizational level. However, trauma centers frequently only evaluate patient deaths within their respective in-hospital setting. These outcomes are rarely, if ever, shared or openly discussed among trauma centers at local levels and even less frequently reviewed at regional or state levels. Furthermore, injury-related deaths occurring in prehospital settings are often excluded from the same rigorous evaluation, whereas deaths occurring at non-trauma center hospitals usually are completely excluded from any analysis. Without combining these three data sources, opportunities for systematic quality initiatives and interventions to address P deaths after injury are limited.
In contrast, the Department of Defense published four articles addressing combat PDR with subsequent data-driven interventions that contributed to a 20% reduction in combat deaths.10–13 The authors formed a multidisciplinary team and translated the results of their near 100% autopsy rate findings and then focused efforts into immediate life-saving interventions for trauma mortality reduction. The process developed over that decade of work laid the foundation for the civilian effort described herein.
The purpose of this article is to describe the method and processes developed to establish a regional PDR in Harris County, Texas, a large, geographically diverse area with a high population density. The processes are described only: data collection is ongoing with consensus panel sessions planned and results are not presented herein. The processes undertaken to determine PDR are expected to result in an evaluation of the various circumstances of death, including emergency medical service (EMS), police, and hospital responses, in a retrospective fashion to determine potential areas in which interventions, equipment, new technology, policy, urban planning, or other factors could potentially change outcomes.
Methodology
Setting
Harris County is the third most populous county in the USA and is home to >4 million residents. The county encompasses a geographic area of 1777 square miles and includes the City of Houston, the third largest county in the USA. Harris County has a mature trauma system with 15 trauma centers, including 2 adult and 2 paediatric level 1 trauma centers, approximately 30 acute non-trauma hospitals, numerous urgent care centers, >90 ground EMS agencies and 2 helicopter EMS agencies. Harris County has over 75 law enforcement agencies as the county has 50 towns with local police forces as well as the office of the Sheriff and various state and federal agencies.
The Harris County Institute of Forensic Sciences (IFS), which includes the Office of the Medical Examiner, investigates all non-natural, sudden, or unexpected deaths in the county. The Harris County medical examiner performs autopsies on >80% of the bodies examined (see figure 1). Complete autopsies are performed on all acutely occurring traumatic scene deaths, including motor vehicle crashes and deaths of hospitalised trauma patients where the cause of death is unclear (unexpected deaths) or where hospital evaluation was incomplete (eg, incomplete radiologic workup).
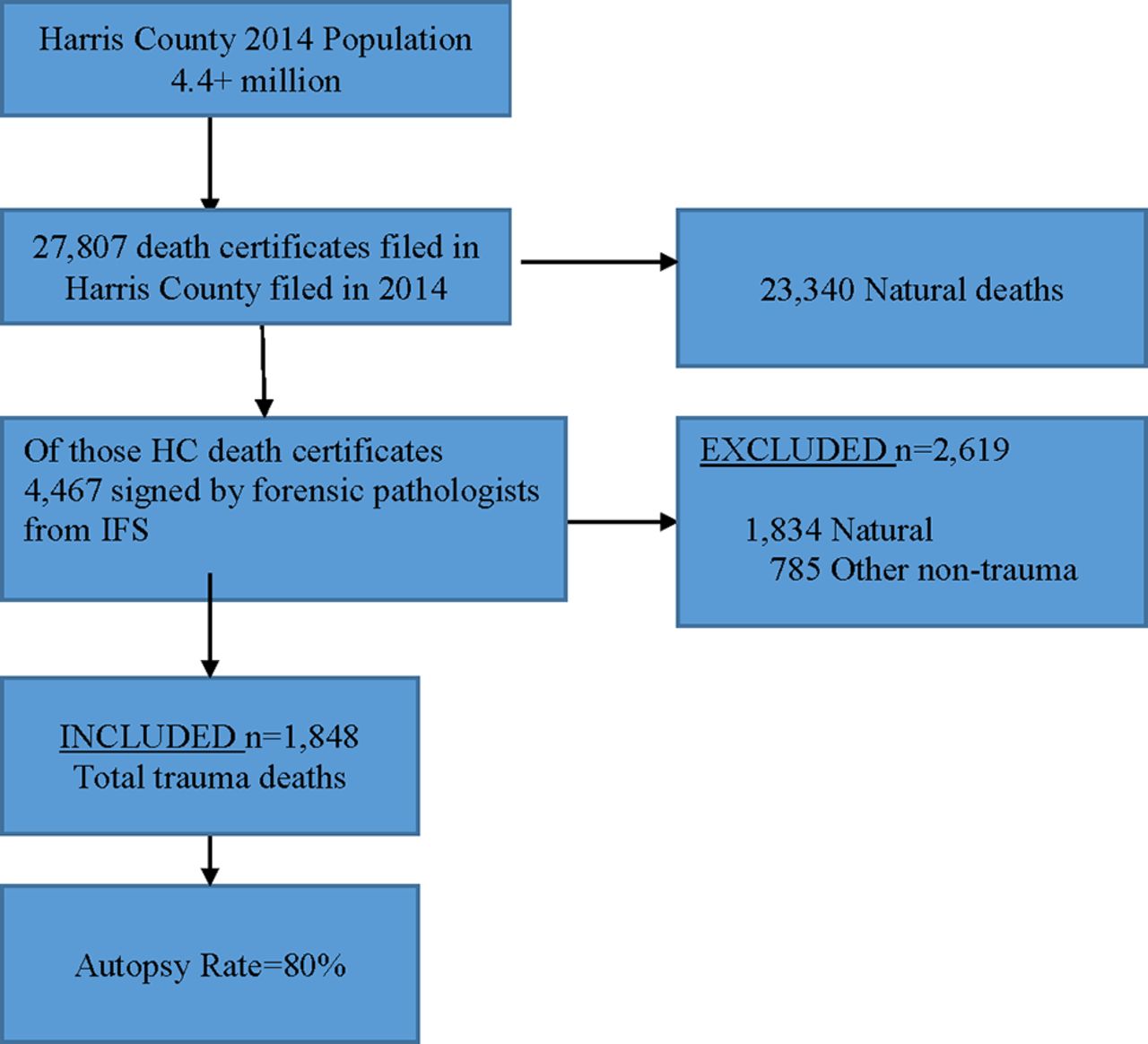
Flow diagram. IFS, Institute of Forensic Sciences.
Design
The design for data collection is based on a 1-year population-based review of medicolegal death investigation records of individuals who died from traumatic causes in Harris County. The records, evaluated retrospectively, include medicolegal and autopsy reports, EMS, medical, and police reports completed during routine death investigations. An interprofessional consensus panel of experts actively involved all aspects of trauma care determines the level of death preventability (P, PP and NP). Once data are collected, spatial analysis and inferential statistical analysis are used to provide information for improving the trauma care system.
Methods phase 1: identify the trauma population
Sample
Traumatic deaths from homicide, suicide, accident, and undetermined manners, including blunt/sharp/firearm/asphyxia or other forms of traumatic injury, within the jurisdiction of the IFS constitute the sample. Records of a single year (2014) are to be reviewed to determine the level of preventability. Excluded from review are deaths occurring from natural manners, drug toxicity, drowning, hanging, and environmental conditions (eg, hypothermia and hyperthermia). Figure 1 provides a detailed illustration of the study cohort.
Measures
The data sources for measurement include autopsy reports, medicolegal death investigative reports, prehospital records, hospital records from both trauma and non-trauma centers and morbidity and mortality preventability quality outcome decisions regarding the preventability of deaths occurring in a trauma center. Data collected are linked and de-identified before analysis. Quality reports are linked using medicolegal death investigation case numbers, date of death, and date of admission. EMS records are linked using the injury address, date and time of injury, and location of transport. Hospital records are linked using unique medical record numbers, date of injury, sex, race, and age. Institutional Review Board approval (when required) is obtained from The University of Texas Health Science Center and Baylor.
The domains and variables to be collected and measured are described in table 1. For the geospatial analysis, the geographical unit of analysis is a census block group, the smallest geographical area for which the US Census Bureau releases socioeconomic data.14
Domains and variables collected
Data management
Data management is to be via an electronic data capture system hosted by The University of Texas Health Science Center at Houston. The system, Research Electronic Data Capture, is a secure, web-based application designed to support data capture studies. Data are assigned unique identifiers, and a code sheet maintained in a separate file. After every 100 cases, 5% of the records are selected for a duplicate abstraction by a different team member to assess inter-rater reliability. Inter-rater reliability for categorical variables is assessed with the kappa statistic, with intraclass correlation coefficients used for continuous variables.
Methods phase 2: determine the level of preventability
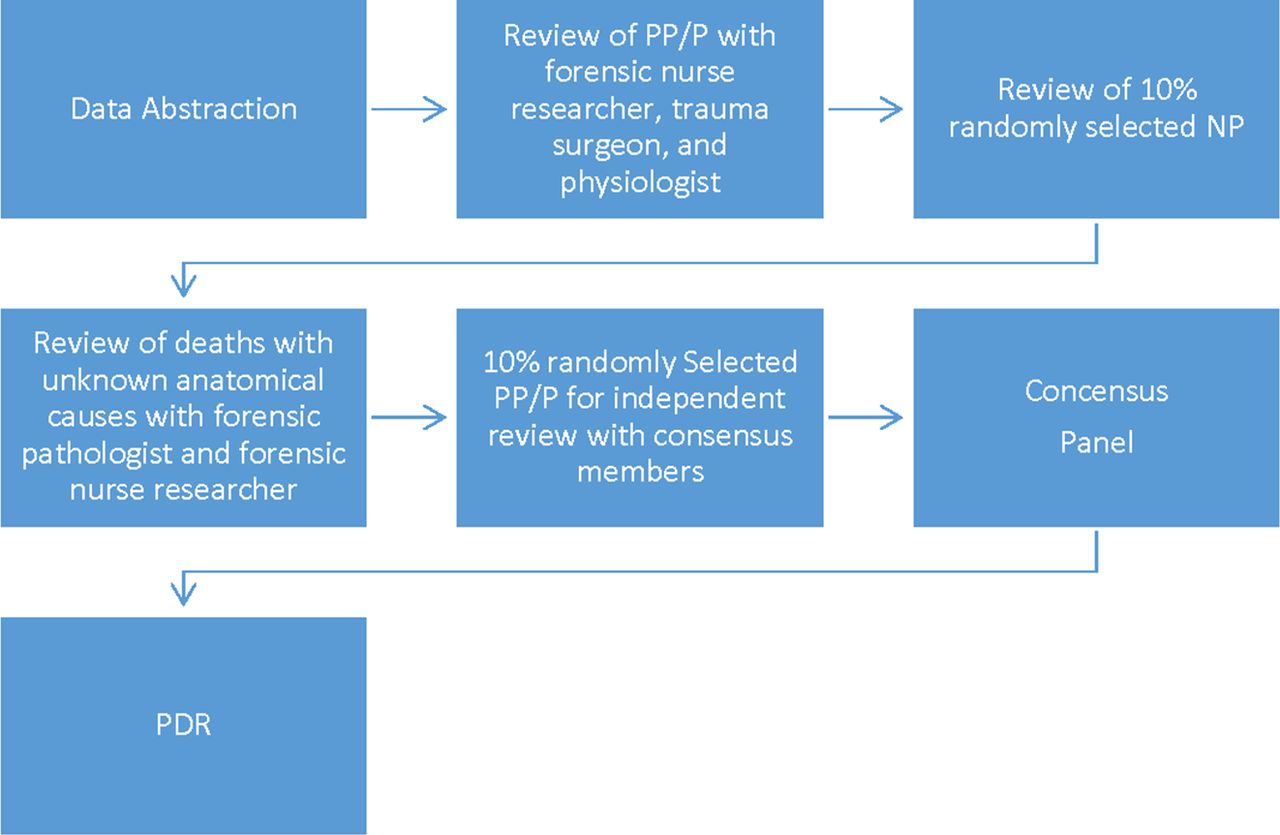
The overall process of data flow from data collection through various phases and ending with the establishment of a PDR is shown in figure 2. Explanations and definitions of terms are presented in the following paragraphs.

Process of date flow. NP, non-preventable; P, preventable; PDR, preventable death rate; PP, potentially preventable.
During the data collection and coding phase, a doctorate level research nurse and baccalaureate nursing students serve as initial data abstractors. The student nurses are trained in injury coding and participate in monthly inter-reliability meetings with level I trauma centre personnel. In addition, a certified injury coder conducts an inter-rater reliability of 10% of those deaths in which injury severity scores (ISS) or new ISS from a trauma centre were not received. The principal investigators meet bi-weekly to ensure anatomic injuries initially abstracted as P and PP are being described and categorized appropriately. Cases in which questions regarding anatomical causes of death will be reviewed bi-weekly by the principal investigator (PI)/forensic nurse and pathologists. A randomly selected subset of 10% of the NP deaths will undergo a second review by the PI and trauma surgeons to ensure appropriate categorization.
For purposes of categorisation, P deaths are anatomic injuries and sequelae clearly considered survivable if appropriate steps had been taken, including divergence from standard of care that directly or indirectly caused the patient’s death.5 14 PP deaths are anatomic injuries that are severe but survivable under optimum prehospital and hospital care.5 10–14 NP deaths include those with anatomical injuries of torso dismemberment, catastrophic brain injury (ie, brain avulsion, transcranial penetrating brain injury involving deep nuclei or critical vascular structures and brain stem injury), cervical spinal cord transection (above cervical level 3), major airway transection within the thorax, perforating/penetrating cardiac injury (>1/2 inch), free bleeding from a thoracic aorta injury, major pulmonary artery injury with free bleeding, hepatic avulsion with free bleeding, and catastrophic abdominal pelvic injury (lower extremity amputations with open pelvis and large soft tissue loss/traumatic hemipelvectomy).13 Also, anatomical injuries included in the NP category are any mechanism of asphyxia (including strangulation), atlanto-occipital disarticulation, charred remains, air embolism, and C1 to C4 fractures with spinal cord involvement verified via autopsy. NP will also include those deaths in which the cause of death was attributed to significant co-morbid conditions. Deaths identified as NP, after being reviewed by the individual hospital trauma department or principal investigators, are excluded from further review provided no system issues are identified.
The consensus panel applies a consensus-oriented decision-making model.15 The consensus panel, composed of general, neurological, paediatric, a surgeons; emergency physicians; nurses; forensic pathologists; prehospital providers; and trauma programme managers, is responsible for resolving cases where unanimity minus two is not reached. A potential concern is panel adherence to established criteria for determining PP and P deaths. To minimize variation, 15 sample cases (5 per category) are presented as a training guide.16
In summary, using all available data, the principal investigators independently categorizes deaths as PP or P using predetermined preventability guidelines. Following independent review, cases with non-unanimous categorizations of preventability are reviewed using a consensus model.15 The consensus meetings are to be recorded to capture variables of interest for future analysis.
Methods phase 3: identifying opportunities for reducing P death
An adaptation of a social-ecological model serves as the framework for understanding the interrelationships among individual, interpersonal, organisational, community, and societal factors that may be associated with trauma deaths.17 18 This model allows for a broader understanding of the range of factors that place people at risk of trauma death. In addition, the model permits a deep understanding of how different levels of variables interact. Variables of interest specific to organisation and community include census tracts, hospital locations, level of trauma expertise based on trauma designation of hospital, and prehospital EMS or fire department locations. Finally, societal variables include a collection of national, state, and local prehospital and hospital guidelines that drive trauma care within the region.
Statistical analysis
To assess the inter-rater reliability of data abstraction, after every 100 cases, 5% of the records will be randomly selected for a duplicate abstraction by a different member of the team. Inter-rater reliability for categorical variables will be assessed with the kappa statistic, whereas the intraclass correlation coefficient will be used for continuous variables. Inter-rater reliability between panel members for the level of preventability of death will be evaluated using the kappa statistic. Frequencies and descriptive statistics will be calculated from the sample data to address aim one. The consensus decision rule will be the supermajority or unanimity minus two.15 Those cases not reaching supermajority will be excluded from the prediction analysis. Logistic regression analysis will be used to determine those factors significantly associated with preventability. A sequential method will be used to enter variables into the model in blocks, beginning with demographic factors. Investigative and autopsy variables will be added to those variables that are found to be significant (p<0.05) in the initial model. The final model will include only those factors with a p<0.05. Statistical analyses will be conducted with IBM SPSS Statistics V.24.0 and SAS V.9.4 for Windows. Triage decisions, and specifically an under-triage rate, are determined by identifying those PP and P deaths that were taken to a non-trauma center. The target rate is considered to be <1%.2 In addition, determination is made of how many major trauma patients (ISS >16) were transported incorrectly to a non-trauma. The target rate is set at 5%.2
Discussion
Although many trauma clinicians are aware of processes and outcomes at their respective trauma centers, the ability to evaluate the entire regional trauma system and thus the nation in a comprehensive fashion is lacking. By virtue of their statutory role, medicolegal death investigation agencies are the repository of data on trauma deaths within a geographic area. However, in the USA, these agencies rarely interact with trauma centers or regional/state trauma systems. In contrast, in the UK and New Zealand, the medicolegal death investigation system has established entire departments that exclusively work with clinicians for the sole purpose of identifying, discussing, and addressing P deaths.8 9 19 20 Linking the two systems, clinical trauma care and death investigative services, is crucial to establishing an accurate regional PDR.
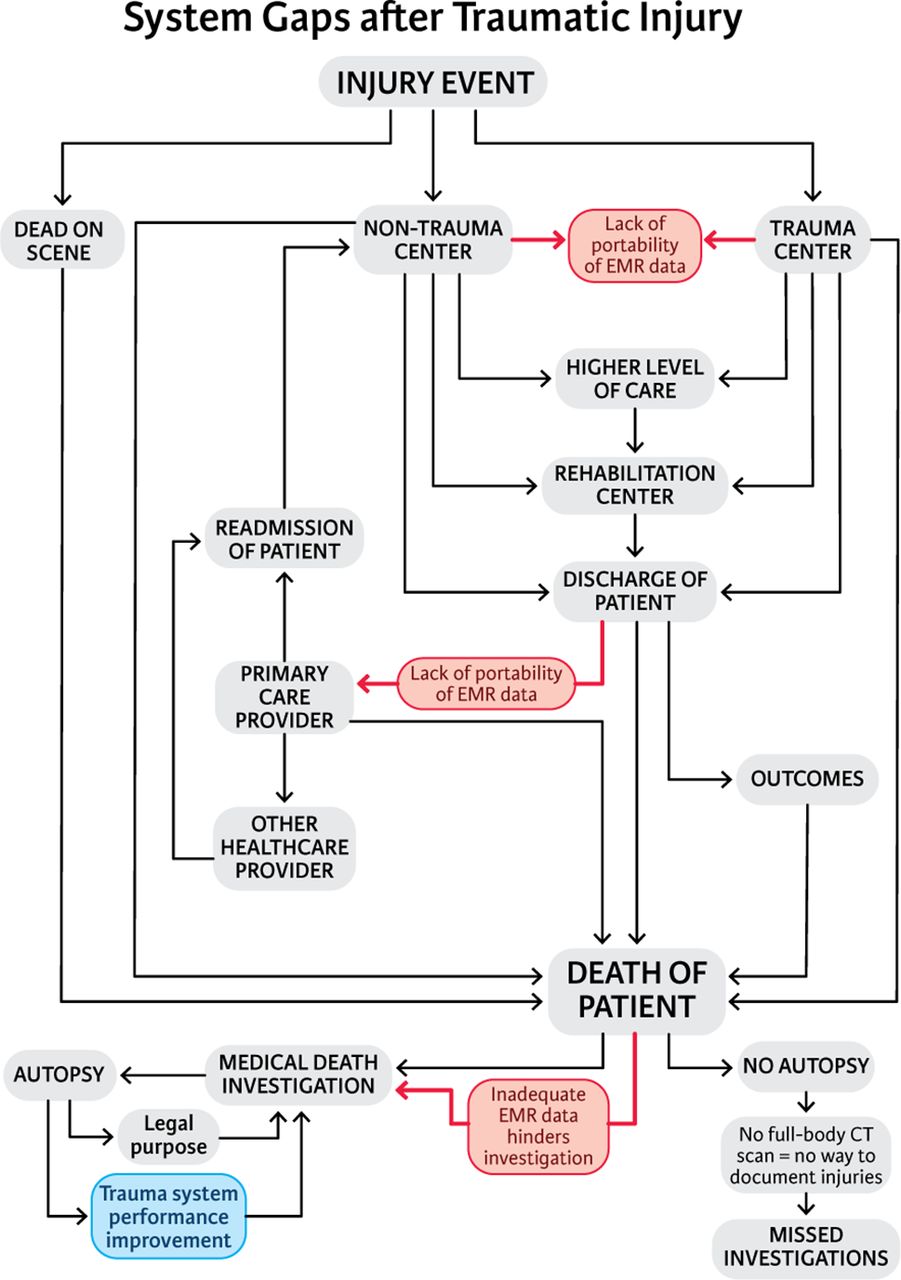
In developing this study design, several unique opportunities for improving data gathering within the trauma system were discovered and should be considered for future studies. These challenges include the following: longitudinal perspective of trauma deaths, nontrauma center deaths, deaths with confounding medical factors, readmissions within 30 days, patients who visited multiple hospitals or urgent care or primary care providers for initial points of contact, and linkages between the multiple different data sets. Sharing the outcome of these and similar studies on potential preventability with local, regional, and state officials should aid in improving trauma system outcomes. Figure 3 illustrates the various system gaps that offer opportunities for system improvements within trauma care.
{kind=link}
{kind=link}
{kind=link}
System gaps after traumatic injury. EMR, Electronic Medical Record
A longitudinal perspective of trauma deaths (ie, deaths from remotely sustained injuries and often years after the acute event) presents challenges in data collection and abstraction simply because of the often complex course of care that may occur after the initial hospitalization. Although trauma systems address the spectrum of acute patient care (eg, prehospital, hospital and rehabilitation), frequently long-term outcomes of the course of care and patient progression after discharge are not always known. This project is expected to provide data as to decedents who died due to complications from injuries sustained months or years in the past.
While collecting data from non-trauma hospitals and factoring in care from free-standing clinics is a challenge, this evaluation provides an immediate tangible benefit: namely, an evaluation of triage by EMS of trauma patients to non-trauma centers and subsequent decision to transfer to a trauma center. Given the large number of non-trauma centers, numerous urgent care or free-standing clinics, and even primary care physicians identified as the first point of care providing trauma care services, over/under triage is a key indicator of how well a trauma system is working. Expansion of this study will inform EMS of crucial areas for improvement in this regard.
Although 30-day readmissions are tracked at a state level and frequently within healthcare systems as indicators of quality, this information is usually not shared or even linked between hospitals. If a patient is readmitted to a different system either by choice or EMS decision, the initial treating hospital or clinician is often unaware of this potentially missed opportunity for improving care. This project will attempt to place timelines on each death, including readmissions or discharge from a hospital with subsequent death at home. This approach has potential value for improving population-level trauma care by identifying gaps in appropriate post-discharge interpersonal or community-level support for trauma patients.
Unlike previously published studies assessing survivability in military settings with study populations that composed of primarily young, physically fit males who died predominately from explosion or gunshot injuries,10–13 this project addresses a demographically diverse population crossing the lifespan with the multiple underlying natural pathological changes associated with the natural aging process. For example, the data include a large proportion of blunt traumatic brain injury deaths resulting from falls in the elderly population. Geriatric patients who fall multiple times and are cared for at multiple disconnected hospitals before finally succumbing to a fatal fall composed of a unique population at a great risk and potential benefit.
The US Military used a similar scheme to drive improvements in their trauma system during the most recent war. These improvements are largely centered on extremity and truncal hemorrhage control, resuscitation and trauma system implementation. Similar haemorrhage control opportunities exist in the civilian system, but because of different demographics it is likely that data-driven prevention and triage strategies will also greatly improve outcomes in the civilian arena.
Finally, the linkage of data in efforts to improve trauma care is critical.1 This project may demonstrate that those who die from complications of remote trauma or geriatric falls often do not receive their care within one system. Thus, improvements in managing the care of trauma patients throughout the larger regional system, that is, from trauma prevention, EMS transport, acute care and through rehabilitation to death, may be needed.
Future directions
Future directions should address policies to support and encourage linkages of data from law enforcement agencies, primary care providers, prehospital setting, free standing emergency rooms, hospitals, rehabilitation facilities, and medical examiners/coroners. Several system-level quality and safety opportunities may be identified within the actual analysis of the data. Importantly, the availability of real-time reporting of autopsy-determined cause of death in regard to preventability within weekly morbidity and mortality conference can lead to rapid improvements in care. In addition, an economic analysis of the current state of both Harris County and state-level trauma systems should be prioritized. This analysis should include a comparative cost analysis of trauma care provided between trauma and non-trauma centers and the cost to implement the regionalization of medicolegal death investigation systems. The inclusive trauma system should embrace the forensic service, so that prevention, prehospital, acute, rehabilitation, and long-term care can be optimised. Taking the lead from our military colleagues, establishing a reliable civilian trauma PDR and methods that can be replicated across different regions is a growing priority in light of increasing unintentional and intentional trauma-related deaths. Finally, it is only through the analysis of all the data from all the agencies constituting a truly comprehensive trauma system that innovative, data-driven interventions be implemented.
Footnotes
Contributors SAD: c
onception and design of the study, interpretation of the data, acquisition of data and drafting and revising manuscript.
DAW: a
cquisition of data, interpretation of data and revising the manuscript.
JCM: r
evising the manuscript.
SGC and TR: a
nalysis of data and revising the manuscript.
CEW: c
onception of the study and revising the manuscript.
JBH: c
onception of the study, interpretation of the data and revising the manuscript.
All authors approved the version of the manuscript being submitted.
Competing interests None declared.
Ethics approval The University of Texas Health Science Center and Baylor University.
Provenance and peer review Not commissioned; internally peer reviewed.
Author note The authors acknowledge Meghan Rock, scientific editor, for contributing to the artwork of Figure 3. Additionally, the authors wish to acknowledge Caitlin Thetford, Morgan Brock, and Lauren Myers for data abstraction.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/