Article Text

Abstract
Lower extremity compartment syndrome is a devastating complication if not rapidly diagnosed and properly managed. The classic symptoms of compartment syndrome can be deceiving as they occur late. Any concern for compartment syndrome based on mechanism, or the presence of pain in the affected extremity, should prompt a compartment pressure check. Both absolute compartment pressures above 30 mm Hg and a pressure differential of less than 30 mm Hg are used to make the diagnosis. The treatment goal is first to save the patient’s life and second to salvage the affected limb. Fasciotomy is the only accepted treatment of compartment syndrome and should be performed quickly after the diagnosis is made. Outcomes after fasciotomy are best when there is no delay in treatment.
- compartment syndrome
- lower extremity trauma
- lower extremity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Importance/background
Lower extremity compartment syndrome is not uncommon and has the potential to cause devastating morbidity for patients and a high-risk medical-legal environment for physicians. Rapid diagnosis and prompt, accurate treatment lead to the best outcomes.
The sequela of compartment syndrome left untreated was first described by Volkmann in 1881. His landmark article detailed ischemia to a limb that when left untreated for several hours led to paralytic contracture.1 The prevailing theory at the time was that tight bandages caused the ischemic insult. Bywaters and Beall better2 defined the disease of compartment syndrome in a case series of British World War II victims in 1941. Labeled initially as a crush injury with impairment of renal function, the authors describe a swollen limb developing into shock, diminished pulse in the injured extremity, impending limb gangrene, progressive renal failure, and ultimately death. This was further elucidated and better characterized by Carter et al3 in 1949 as muscle trauma leading to increased pressure within a muscular compartment that impairs blood supply, leading to necrosis.
Compartment syndrome occurs when the pressure within a defined compartmental space increases past a critical pressure threshold, thereby decreasing the perfusion pressure to that compartment.4 Intracompartmental bleeding leads to increased intracompartmental pressure, which increases venous capillary pressure. Capillary collapse occurs when the compartment pressure surpasses the capillary perfusion pressure, leading to cellular ischemia and necrosis. Interstitial edema develops from tissue necrosis and further worsens compartmental swelling.5
In general, longer periods of compartment syndrome and ischemia correlate with worse outcomes. Tissue ischemia of only 1 hour is associated with reversible neuropraxia, whereas ischemia of 4 hours can induce irreversible axonotmesis.5 Ischemia of up to 6 hours is associated with irreversible necrosis and more likely to produce functional impairment.6 7 Vaillancourt et al8 retrospectively correlated the total time of ischemic insult to tissue with subsequent tissue necrosis seen on fasciotomy. In patients brought to the operating room within 3 hours, 50% had evidence of muscle necrosis. Interestingly, a cohort of 11 patients had an injury-to-fasciotomy time of >24 hours and did not develop any tissue necrosis, so likely the degree of intracompartmental pressure is also a factor in determining outcomes.8
Compartment syndrome can occur in any area of the body with closed compartments. The below knee leg is the most likely compartment to develop acute compartment syndrome, followed by the forearm, thigh, and arm.9 The specific location of injury is important in predicting development of compartment syndrome. In a study evaluating their institutional experience with compartment syndrome, Gonzalez et al10 showed that no patients with distal below knee penetrating injuries developed compartment syndrome, whereas 27% of patients with a proximal below knee penetrating injury eventually required fasciotomy. Similarly, Meskey et al11 demonstrated that proximal tibial and fibular fractures had a significantly higher rate of associated compartment syndrome than middle or distal fractures. Abdominal compartment syndrome is also quite common and has been well described. Gluteal, hand, foot, paraspinal, and mediastinal compartment syndrome are also possible and should be monitored for.12
No comprehensive accounting of the prevalence of acute lower extremity compartment syndrome has been published. In part, this is secondary to the many different causes and descriptions of the disease process. It has been estimated that the average annual incidence is 0.7 per 100 000 women and 7.3 per 100 000 men.13 Roughly 2.8% of patients who sustained extremity trauma will require a fasciotomy.9 When Farber et al14 analyzed the National Trauma Data Bank for patients sustaining lower extremity arterial trauma, the number requiring fasciotomy rose to 41.7%.
Causes of compartment syndrome are varied. Trauma is the most likely precipitating factor, with fracture of the extremity leading the greatest number of cases of compartment syndrome.13 Among trauma patients, the incidence of compartment syndrome varies with mechanism. In the largest single center review, Branco et al evaluated trauma patients who developed compartment syndrome for both mechanism and type of injury. Gunshot wound, followed by stab wound, motorcycle crash, and pedestrian struck by automobile are the most likely mechanisms to lead to compartment syndrome.9 Patients who sustained a combined arterial and venous injury had a 41.8% likelihood of developing compartment syndrome, whereas the likelihood was 5.9% for an open fracture and 2.2% for a closed fracture.9 Exertion and drug overdose leading to prolonged pressure on an extremity are also well-documented causes of compartment syndrome.8 Additionally, compartment syndrome can develop in the non-injured extremity from a large systemic inflammatory response and capillary leak.15 Although rare, group A streptococcal infections that are associated with exotoxin release, and tissue swelling can also trigger compartment syndrome.5
A missed diagnosis of compartment syndrome is important because of direct morbidity to the patient and because it creates a high-risk medical-legal environment for the provider. Bhattacharya et al evaluated 19 closed malpractice claims, the most extensive review to date on the medical-legal aspects of compartment syndrome in the USA. The total liability for the 16 patients involved in their analysis was $3.8 million, and the average time to case closure was 5.5 years. Just over half the claims, 52.6%, resulted favorably for the physician. The mean cost of defending a case, even if found in favor of the physician, was $29 500.16 The most prominent risk factor for an indemnity payment was a delay of more than 8 hours from the onset of the disease.16 Marchesi et al evaluated 66 cases in Italy and found even more startling results. Overall, 72% of cases resulted in verdicts against the physician with an average total payment of $574 680. They noted that 32% of the cases found against the physician were for an inappropriate delay in diagnosis.17
Diagnosis
A delay in the diagnosis of acute compartment syndrome can have devastating consequences for the patient. Early suspicion of the disease should invoke an immediate response.
The classic signs of acute compartment syndrome include the 6 ‘P’s’: pain, paresthesia, poikilothermia, pallor, paralysis, and pulselessness. Pain is usually the initial complaint and should trigger the workup of acute compartment syndrome. All patients at risk should have early and frequently repeated physical examinations to assess for pain in the muscle compartments. A clinical diagnosis of compartment syndrome can be followed by prompt surgical decompression; however, the diagnosis is often unclear, and pressure monitoring is commonly required. Because of its subjective nature, although unlikely, the absence of pain cannot negate the possibility of compartment syndrome. Several case reports describe patients with acute compartment syndrome who never experienced pain.18 19 Paralysis, pulselessness, and parasthesias present late in the disease process, often after irreversible nerve and muscle damage, and should not routinely be part of the diagnostic criteria for acute compartment syndrome.
A clear distinction must be made between the evaluable and non-evaluable patient. Obtunded patients cannot communicate early symptoms of acute compartment syndrome, specifically pain. Although a physical examination can still be performed on these patients, this relies on recognizing a more advanced disease state and portends poor outcomes. Compartment pressure monitoring should be used liberally in these patients. Regional anesthesia techniques, such as epidural catheters or more localized nerve blocks, can also block symptoms of compartment syndrome, rendering otherwise evaluable patients non-evaluable.20
For both evaluable and non-evaluable patients, pressure measurement is invaluable in the diagnosis of compartment syndrome. In a landmark 1975 article, Whitesides et al21 introduced the concept of compartment pressure as a diagnostic tool. Because the presentation of compartment syndrome can vary drastically with each patient, compartment pressure provides an objective data point with which to make a clinical decision. Whitesides followed his original article with a detailed description of his technique.22 In his method, an air pressure system is created by connecting a mercury manometer to intravenous extension tubing and a needle, which is inserted into the muscle compartment. A minute amount of saline is injected into the compartment, which transmits air pressure to manometer, and a compartment pressure is obtained.
In contemporary practice, a commercially available device such as the Stryker system is often used. After being zeroed, the needle is inserted perpendicular to the skin, then into the muscle compartment in question. A total of 0.3 mL of sterile saline is injected through the needle into the compartment. Equilibrium is reached in a few seconds, and the compartmental pressure is then read on a digital screen (figure 1). If the Stryker system is not available, a pressure transducing system, like that used for an arterial line and similar to Whitesides’ original description, can be used.

Side-port needle, diaphragm chamber, and prefilled syringe assembled and placed in the Stryker device.50
Traditionally, an intramuscular compartment pressure of >30 mm Hg was used as a diagnostic threshold for diagnosing compartment syndrome, although the absolute pressure value has been debated.23–25 However, the accuracy of using single compartment pressure data points has been called into question.26 27
Tissue perfusion pressure, or delta pressure, which is calculated as diastolic blood pressure minus the compartment pressure, has been studied as an alternative trigger for compartment release. Because this value takes into account the dynamic blood pressure of each patient, it has been argued to be a more accurate value to use in diagnosis.21 28 In a prospective study, McQueen et al examined the use of a pressure differential as diagnostic criteria for acute compartment syndrome. They showed no missed diagnoses of compartment syndrome when a perfusion pressure of less than 30 mm Hg was used as criteria for surgical decompression.29
Concerns remain over consistently elevated intramuscular compartment pressures, despite adequate perfusion pressure. In response, White et al designed a study to examine long-term muscular function after prolonged periods of elevated intramuscular pressure.30 In their study, patients with adequate perfusion pressure above 30 mm Hg were grouped into intramuscular pressures above or below 30 mm Hg for more than 6 hours. Patients then underwent both muscular function and neurologic testing at 3, 6, and 12 months. Isolated compartment pressures even as high as 70 mm Hg were seen to be tolerated as long as the perfusion pressure remained above 30 mm Hg. There was no statistical difference in outcomes between the groups, and no patients had lasting neurologic deficit or contracture, irrespective of the isolated pressure as long as adequate perfusion pressure was maintained.30
Continuous compartment pressure monitoring has been suggested as an alternative to spot compartment pressure checks. A slit catheter is inserted into the compartment in question and connected to a continuous pressure transducer. An obvious limitation to this technique is that it is best suited for measuring one compartment at a time. Still, the sensitivity of continuous monitoring has been shown to be 94% with a specificity of 98%.31 The use of continuous compartment monitoring is currently being studied with the goal of creating a validated prediction tool for acute compartment syndrome.32
A delay in the diagnosis of acute compartment syndrome can have devastating consequences for the patient. Fasciotomies performed more than 8 hours after injury are associated with a significantly higher risk of infection.33 There is no doubt that frequent examinations should be performed on patients at risk of developing compartment syndrome. To this end, some groups have advocated for screening protocols. One group instituted a compartment syndrome screening system for high-risk trauma patients, including those with Swan-Ganz catheter-guided resuscitation, open or closed tibial fracture, major vascular injury below the aortic bifurcation, abdominal compartment syndrome, or an abdominal or pelvic crush injury. The protocol included physical examination and compartment pressures, when indicated, every 4 hours for the first 48 hours. Their study showed a high rate of acute lower extremity compartment syndrome, 20%, in the patient population that underwent screening. Despite high injury severity score and massive resuscitation, no patients in the screening protocol lost a limb.34
It is of utmost importance to measure all muscular compartments, not only the compartment thought to be at highest risk. In the below knee leg, all four compartments must be checked, even though the anterior compartment has the highest risk of compartment syndrome. A common pitfall is to assume that a patient with an open fracture has already decompressed. However, patients with open fractures are at risk of developing compartment syndrome.9 Because compartment syndrome is a dynamic process, even if the initial compartment pressure is normal, it is imperative to repeat frequent examinations and pressure checks to not delay the diagnosis.
Treatment
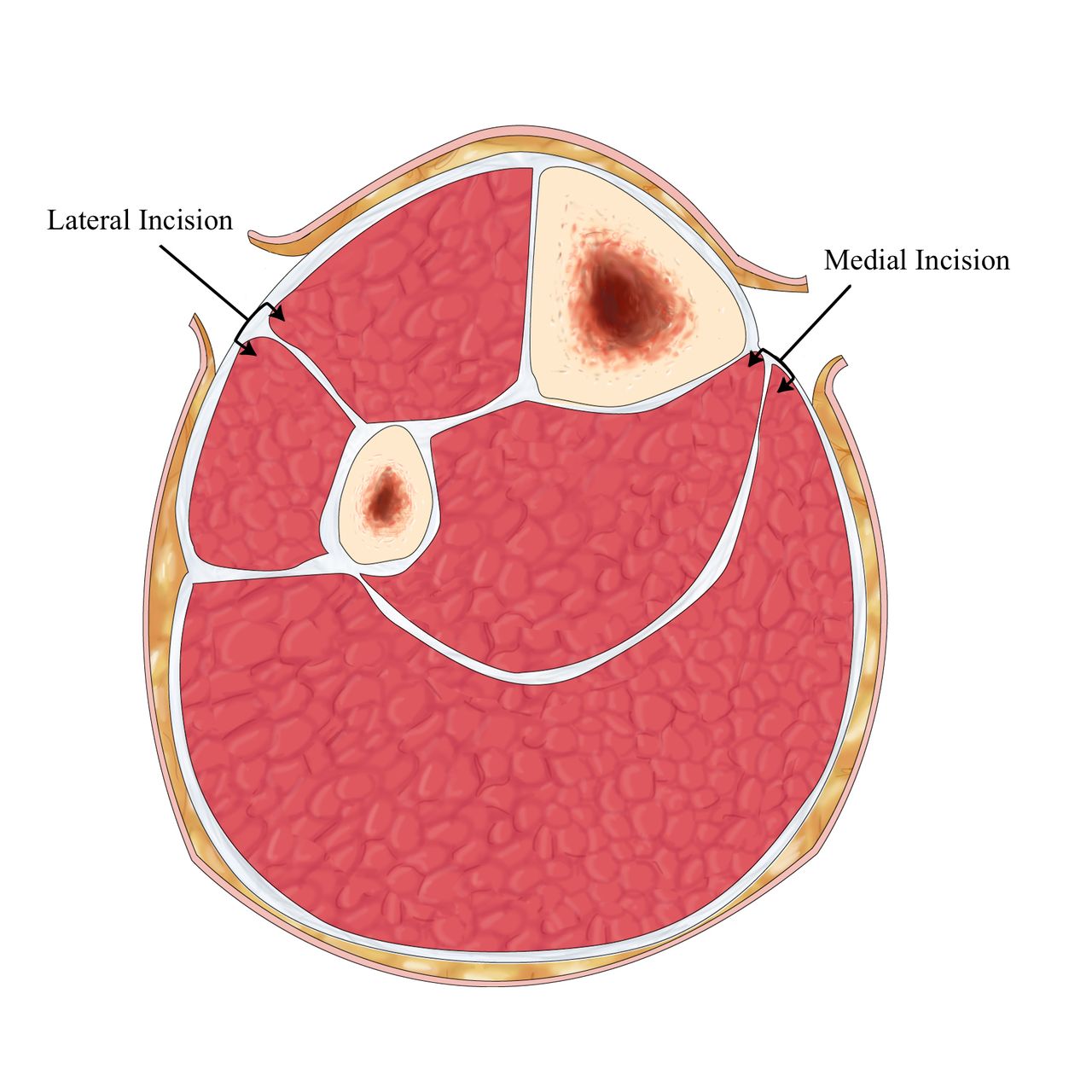
The traditional treatment for lower extremity compartment syndrome is a two-incision, four-compartment fasciotomy and has been well described in the literature.35 36 The lateral incision decompresses the anterior and lateral compartments, whereas the medial incision decompresses the superficial and deep posterior compartments (figure 2). A complete fasciotomy is of utmost importance. Incomplete fasciotomies do not adequately release a muscular compartment, contribute to continued compartment syndrome, and lead to worse outcomes.37
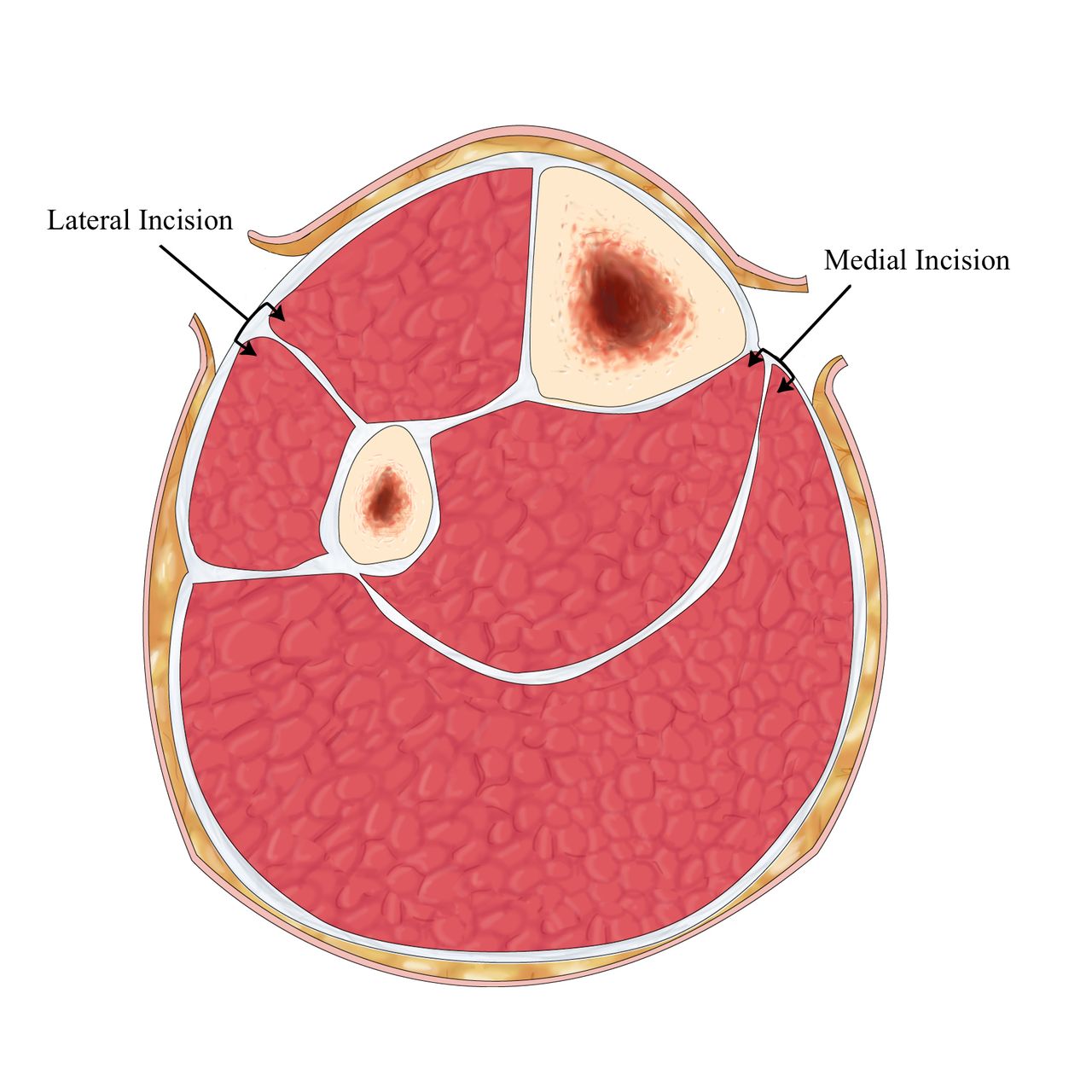
Four-compartment fasciotomy of the right leg through two incisions. The lateral incision decompresses the anterior and lateral compartments, and the medial incision decompresses the superficial and deep posterior compartments.50
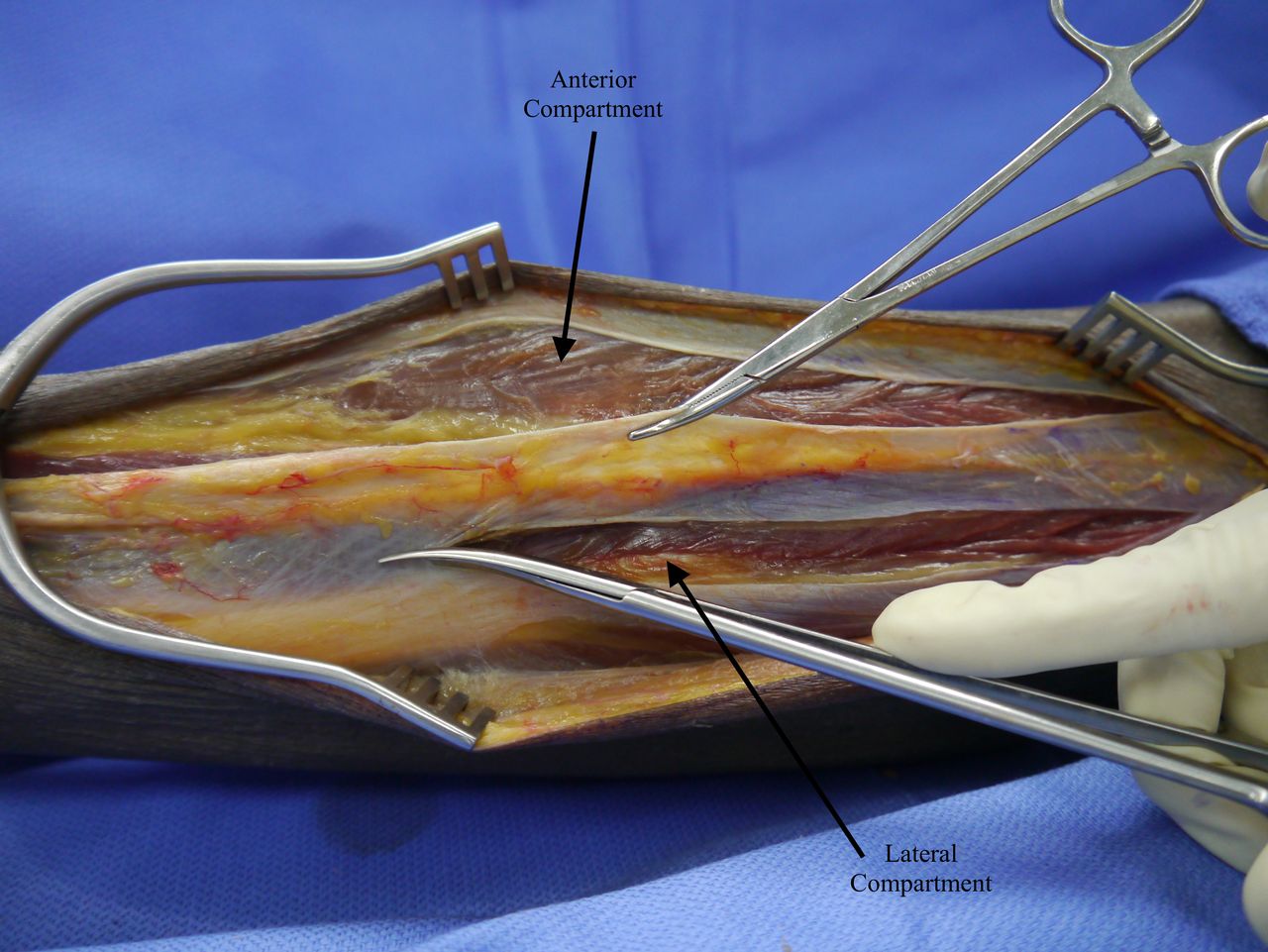
The lateral incision is made from the tibial tuberosity to just above the lateral malleolus. The incision is continued through the subcutaneous tissue, and a fasciotomy is performed to enter the anterior compartment. This is extended via a longitudinal incision along the entire length of the fascia with blunt-tipped scissors. The intramuscular septum is identified from its perforating vessels. Alternatively, the surgeon can make a transverse incision over the suspected site of the septum to confirm the location of the anterior and lateral compartments. A longitudinal incision is made behind the intercompartmental septum to open the lateral compartment, taking care not to injure the superficial peroneal nerve (figure 3).38
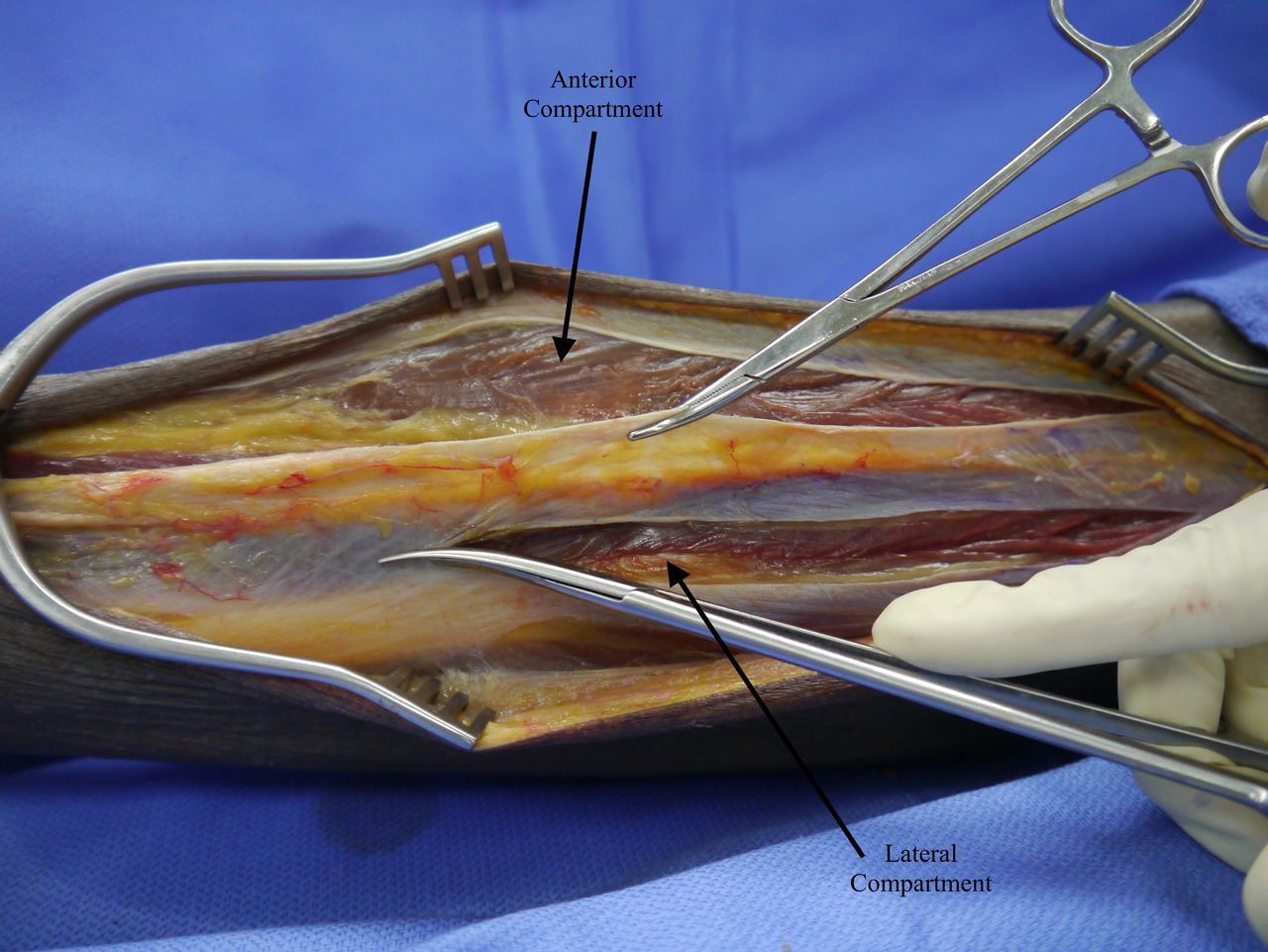
Identification of the septum, which separates the anterior and lateral compartments. The lateral compartment is decompressed with long scissors.50
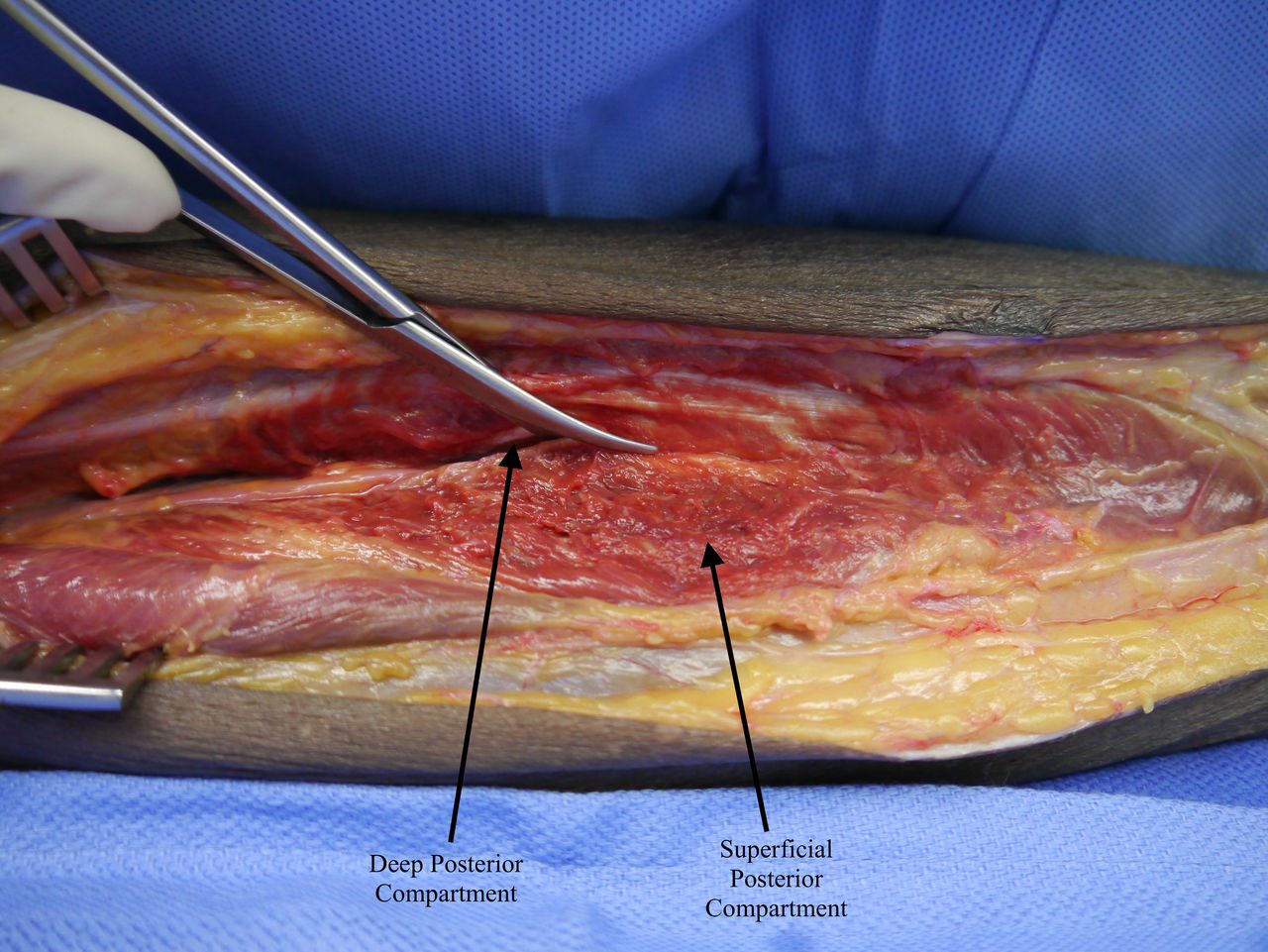
The medial incision is made two fingerbreadths posterior to the tibia from just distal to the knee to just proximal to the medial malleolus. Again, the incision is carried through the subcutaneous tissue, without injuring the saphenous vein. The superficial posterior compartment is opened first. The deep posterior compartment is entered by taking the soleus muscle off of the posterior edge of the tibia. The deep posterior compartment is the most commonly missed compartment, so it is important to identify the underside of the tibia to ensure entry into the deep posterior compartment (figure 4).38

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left leg fasciotomy, medial incision. The superficial compartment is decompressed with a fascial incision, made about two fingerbreadths posterior to the tibia. The deep posterior compartment is decompressed through a fascial incision just behind the edge of the tibia.50
Although we do not advocate this, some groups have described using a single incision fasciotomy to decompress all four compartments of the lower leg.39 40 In this approach, the skin incision is made laterally between the tibia and fibula. The anterior and lateral compartments are entered in the routine fashion. The superficial peroneal nerve is retracted anteriorly, and the posterior intermuscular septum is found inside the lateral compartment. The superficial posterior compartment is decompressed by incising the posterior intermuscular septum. The deep posterior compartment can be entered via the anterior compartment by retracting the tibialis anterior laterally and incising along the lateral tibia, through the interosseous membrane.39 A retrospective case series has shown no difference in deep infection rate, bone nonunion, and length of follow-up between patients with tibial fractures receiving either a single or dual incision fasciotomy, although this study did not evaluate for missed compartment syndrome requiring repeat fasciotomy.40 Further literature on the single incision fasciotomy technique is very limited.
At the index operation, if non-viable muscle is encountered, it should be debrided. Any questionable muscle can be re-examined at a planned second look operation within 24 hours from the index operation.
Multiple techniques can be used for closing or dressing fasciotomy wounds. Immediately after a fasciotomy, it is advisable to use a loose, non-constricting dressing to allow the muscle to fully expand, especially if there is ongoing resuscitation. Kerlix or gauze dampened with sterile normal saline should be placed over the wound, covered with abdominal pads, and lightly covered with additional kerlix. After the index operation, both traditional wet-to-dry dressings and tension-based dressings, such as a shoelace technique or a vacuum-assisted-closure dressing, can be used. The goal with any type of fasciotomy dressing is to facilitate delayed primary closure of the wound.
Weaver et al examined fasciotomy dressing practice patterns in two urban level one trauma centers. Overall, 18% of patients in their study were able to be primarily closed on the first return to the operating room and 40% underwent split-thickness skin graft. Only 3% of patients were primarily closed on the second return to the operating room. Among the 38% of patients who underwent more than two wound washouts and debridements, none of the patients were able to undergo delayed primary closure.41 When patients are subcategorized into early or late fasciotomy, defined as less than or greater than 8 hours from injury to fasciotomy, there is a significantly higher rate of eventual primary closure in patients receiving an early fasciotomy.34
There is evidence that the use of a vacuum-assisted closure dressing is associated with significantly higher rates of primary closure than traditional dressings.42 Conversely, Kakagia et al found that patients who received a vacuum-assisted closure dressing had a significantly longer time to wound closure than patients who received a shoelace technique.43 Vacuum-assisted closure dressing was also associated with significantly more expense than the shoelace technique.43 Patients that receive split thickness skin graft early in their course have a significantly shorter length of stay than patients treated with traditional dressings.41 It is clear that with lack of consensus in the data, at this time much of the decision regarding the fasciotomy dressing will rest with the culture of the institution and the preferences of the individual surgeon.
Complications/outcomes
Unfortunately, complications after fasciotomy are not rare. Nearly one-third of patients receiving fasciotomies will end up with a postoperative complication: soft tissue necrosis, wound dehiscence, skin graft infection or necrosis, or need for tissue debridement.34 Underlying vascular injuries leading to fasciotomy are associated with a significantly higher rate of complications than patients without vascular trauma.34 When Feliciano et al35 evaluated a large series of compartment syndrome that led to amputation, 75% were associated with a delay in appropriate treatment.
One of the biggest pitfalls surrounding fasciotomy for compartment syndrome is missing or inadequately opening a compartment. A missed compartment is a critical technical error as irreversible muscle and nerve may damage occur. In a study of military patients, Ritenour et al37 showed that the need for a fasciotomy revision was associated with significantly higher rates of muscle necrosis and fourfold increase in mortality. Postoperatively, the patient must be frequently examined and the creatine kinase (CK) levels followed. Failure to clear CK or any other concerns of a missed compartment must trigger immediate re-exploration.
Rhabdomyolysis may result from the muscle necrosis secondary to compartment syndrome, with ischemic cellular contents spilling into the circulation. The released myoglobin can lead to acute kidney injury and kidney failure. Because the cytokine release associated with rhabdomyolysis causes swelling, it can also precipitate and worsen compartment syndrome. In some instances, rhabdomyolysis is the precipitating factor in causing compartment syndrome. The rate of rhabdomyolysis after acute compartment syndrome has been reported as 44.2%.44 Of the patients that develop rhabdomyolysis, 14.4% to 39.1% develop acute kidney injury (AKI).44 45 Risk factors for rhabdomyolysis include patients using drugs and alcohol and presenting with pulselessness in the affected extremity.44 Of the patients who develop traumatic compartment syndrome-related AKI, the need for dialysis is high, in one series documented at 44.4%.44
Loss of limb is, arguably, the most devastating complication of compartment syndrome. The reported amputation rate after compartment syndrome is 5.7% to 12.9%.18 46 47 Risk factors for amputation include male gender and associated vascular injury.47 A delay in the time to fasciotomy has also been associated with the need for amputation.18 Patients who do not require amputation can still develop tremendous disability. Up to 18.2% of patients develop foot drop,47 10.2% to 84.6% have chronic lower extremity pain,47 48 and in one series only 69.2% returned to work.47 Patients who reported the appearance of their limb as problematic had overall significantly worse quality of life than patients who did not find their fasciotomy scar to be a problem.49 Mortality after compartment syndrome has been reported to be as high as 15% in one case series, although a causal link is not clear.46
Conclusion
Vigilance is key when evaluating and treating patients with lower extremity compartment syndrome. The classic signs of compartment syndrome, the ‘6 P’s’ can be deceiving. If there is any concern for compartment syndrome, especially when a patient has pain out of proportion to an injured extremity, compartment pressures should be checked immediately. Fasciotomy is a simple, straightforward treatment that is highly effective if performed early.
References
Footnotes
Contributors JC wrote the article. KI organized, reviewed, and edited the article.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.