- Correspondence to Dr John P Sharpe, Department of Surgery, University of Tennessee Health Science Center College of Medicine, 910 Madison Avenue #210, Memphis, TN 38163, USA; jsharpe6{at}uthsc.edu
- Received 23 February 2017
- Accepted 3 April 2017
Abstract
For any trauma surgeon, colon wounds remain a relatively common, yet sometimes challenging, clinical problem. Evolution in operative technique and improvements in antimicrobial therapy during the past two centuries have brought remarkable improvements in both morbidity and mortality after injury to the colon. Much of the early progress in management and patient survival after colon trauma evolved from wartime experience. Multiple evidence-based studies during the last several decades have allowed for more aggressive management, with most wounds undergoing primary repair or resection and anastomosis with an acceptably low suture line failure rate. Despite the abundance of quality evidence regarding management of colon trauma obtained from both military and civilian experience, there remains some debate among institutions regarding management of specific injuries. This is especially true with respect to destructive wounds, injuries to the left colon, blunt colon trauma and those wounds requiring colonic discontinuity during an abbreviated laparotomy. Some programs have developed data-driven protocols that have simplified management of destructive colon wounds, clearly identifying those high-risk patients who should undergo diversion, regardless of mechanism or anatomic location. This update will describe the progression in the approach to colon injuries through history while providing a current review of the literature regarding management of the more controversial wounds.
- trauma/ critical care
- colon
- algorithm
Introduction
Few injuries have reached the advances in management that have been obtained with trauma to the colon. What was once a death sentence for a patient 150 years ago, the majority of patients presenting with colon injuries today are surviving their hospital stay with a relatively low complication rate. With the development of more aggressive operative techniques and improvements in antimicrobial therapy, colon-related morbidity has decreased to just 15%, and the mortality secondary to colon injuries has dramatically declined from as high as 90% during the early Civil War experience to as low as 1% in the most current literature.
Much of the early progress in management and patient survival after colon trauma evolved from wartime experience. These military practices were then transitioned into civilian care. During the past four decades, aggressive trauma surgeons have refined techniques in the management of colon trauma, developing evidence-based approaches to these sometimes difficult injuries, further improving on patient morbidity and mortality.
Despite an abundance of quality evidence regarding management of colon trauma obtained from both military and civilian experience, controversy still exists regarding management of specific injuries. This is especially true with respect to destructive wounds, injuries to the left colon, blunt colon trauma and those wounds requiring an abbreviated laparotomy. For any trauma center, colon trauma is a relatively common occurrence. However, many surgeons still follow dogmatic principles rather than taking an evidence-based approach to these injuries. This update will describe the progression in the approach to colon injuries through history while providing a current review of the literature regarding management of the more controversial wounds.
History of military and civilian experience
The first report of a colon injury occurred during biblical times in the book of Judges, when Ehud killed King Eglon (Book of Judges – Jud 3:21–22). As described here, “And Ehud said, ‘I have a message from God for you.’ And he arose from his seat.21 And Ehud reached with his left hand, took the sword from his right thigh, and thrust it into his belly.22 And the hilt also went in after the blade, and the fat closed over the blade, for he did not pull the sword out of his belly; and the dung came out”.1
Although colon injuries certainly still existed, little was written regarding their management until the Civil War. During this period, colon wounds were almost uniformly fatal with mortality rates greater than 90%.2 3 Patients who did not die to their primary injuries ultimately died from secondary infection and sepsis after expectant management, a practice that would not even be considered today. However, non-operative management was considered reasonable at the time, since any attempts made at operation lead to equivalent mortality rates.
With World War I came the introduction of higher velocity weaponry, and thus, more destructive injuries. Similar to the Civil War experience, early care consisted of expectant management. However, as the war continued, later attempts were made at primary repair or diversion. With this minor advancement in operative technique, mortality rates fell to 60% to 75%.4
By World War II, these mortality rates fell to 22% to 35%. Although this was largely due to advancements in triage, more aggressive resuscitation, improved antibiotics and better blood banking systems, management of the colon wounds themselves became more rigid.5–8 All colon injuries were managed with exteriorization. In fact, William H. Ogilvie, a British surgeon who served in both world wars and provided much of the medical research at the time from his military experience, stated in one of his publications, ‘The treatment of colon injuries is based on the known insecurity of suture and the dangers of leakage. Simple closure of a wound of the colon, however small, is unwarranted; men have survived such an operation, but others have died who would still be alive had they fallen into the hands of a surgeon with less optimism and more sense. Injured segments must either be exteriorized, or functionally excluded by a proximal colostomy’.9
Interestingly, scholars maintain Ogilvie's own experience during that time demonstrated equivalent mortality rates between primary repair and diversion.3 9 Nonetheless, as World War II evolved, after Ogilvie's experience with the British forces and the introduction of mandatory diversion, the United States Office of the Surgeon General mandated the punishment for repairing a colon injury was as severe as a court martial. However, it is difficult to find evidence anyone actually received this punishment.2 10
Surgeons returned home from World War II convinced colostomies were the necessary management for all colon trauma. This experience is reflected in an early report from Dr Alton Oschner in New Orleans,7 ‘At the Charity Hospital of Louisiana in New Orleans, 23 cases of colon injury were treated during the years 1945 and 1946. Primary suture was used in 15 of these cases, but during 1947 and 1948, the influences of war surgery became evident, because in 25 cases of colon injury, only five were treated with primary suture. Although exteriorization or proximal decompression proved valuable in the treatment of battle colon injuries, an evaluation of the results obtained in civilian practice is essential’.
Trauma surgeons soon recognized that penetrating civilian colon injuries were different from their military counterparts. Civilian wounds were far less destructive and thus amenable to less aggressive surgical management. Nonetheless, for several decades, diversion remained the standard of care for all colon trauma until 1979, when Stone and Fabian performed the first randomized clinical trial to compare primary repair and exteriorization of colon injuries.11 The authors randomized 139 patients with colon wounds to either primary repair or colostomy. Interestingly, patients randomized to primary repair had a lower intra-abdominal infection rate compared with those patients randomized to colostomy and those with mandatory colostomy. The authors had confirmed the safety of primary closure for colon wounds in selected cases. Thus, a more aggressive approach to repair of less destructive colon injuries had begun.
Destructive colon wounds
The initial randomized clinical trial by Stone and Fabian led to further refinement of the standard treatment of colon injuries. Since that time, subsequent randomized clinical trials and prospective observational studies have demonstrated that primary repair can be successfully performed in most civilian colon injuries.12–27 Despite continued advancements in the operative management of penetrating colon injuries, optimal management of destructive colon wounds requiring resection remains controversial.
Indicators of a destructive penetrating colon injury
Wounds >50% of colon wall circumference
Complete transection
Devascularized segments
The well-accepted criteria for a penetrating destructive injury includes those wounds involving greater than 50% of the colon wall circumference, complete transection of the colon itself and devascularized segments (box 1).28 In 1994, Stewart et al used this criteria to evaluate 60 patients with destructive colon wounds during exploration. The authors noted those destructive wounds associated with significant comorbidities or transfusion requirements >6 units packed red blood cells (PRBCs) had a suture line failure rate of about 42%, whereas those destructive wounds in otherwise healthy patients with fewer transfusion requirements had a suture line failure rate of about 3% (Table 1).28
Stewart et al: risk factors for suture line failure
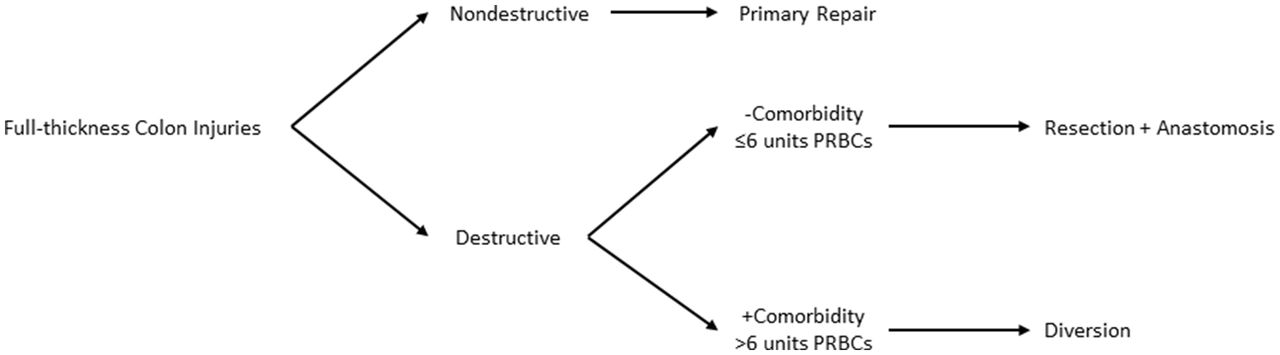
From the results of Stewart's study, the Memphis group developed a management algorithm for colon wounds (figure 1). The patient is evaluated in regard to type of colon injury. All non-destructive injuries are treated with primary repair. Those patients with destructive colon injuries are then evaluated with respect to significant medical illness and transfusion status. If the patient has a significant comorbidity or transfusion requirement >6 units PRBCs, the patient is managed with a diverting ostomy. However, if the patient has a destructive colon injury with no significant comorbidities and transfusion requirement ≤6 units PRBCs, the patient is managed with resection and anastomosis.
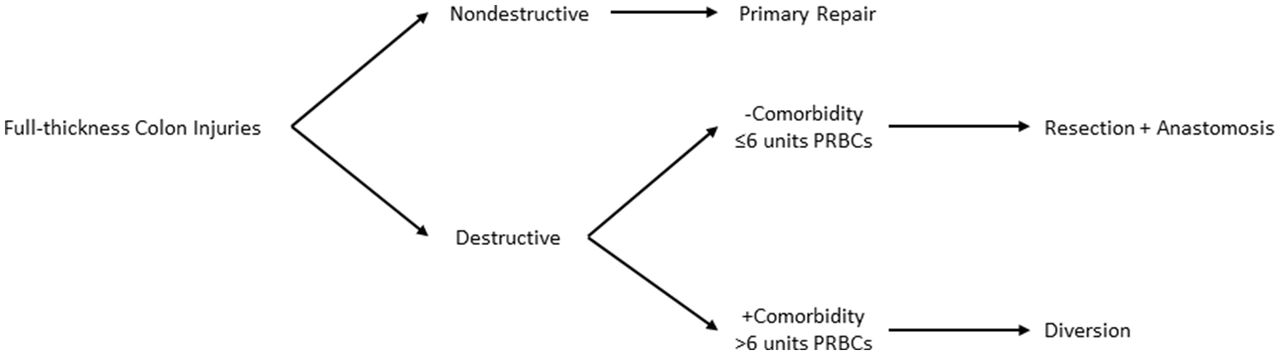
Defined management algorithm for penetrating colon injuries. PRBCs, packed red blood cells.
After Stewart's study and the development of the algorithm, other programs began to recognize the dangers of resection and anastomosis of destructive injuries and began to seek out their own risk factors for complication. In 1998, Cornwell et al evaluated 25 patients who underwent resection and anastomosis after penetrating colon injury.29 The authors noted suture line failure in two (8%) of those patients, both of whom developed sepsis and a colon-related death. Closer analysis of these patients revealed they suffered higher Penetrating Abdominal Trauma Index (PATI) scores and had larger transfusion requirements. Based on these results, the authors concluded that a high PATI and multiple blood transfusions reliably identify those patients at high risk of septic complications after penetrating colon injuries and thus, there is still room for consideration of fecal diversion in the management of these patients.
In 2002, the Memphis group then performed a follow-up study nearly 8 years after the development of their management algorithm.30 The authors evaluated 56 patients with destructive colon injuries managed after the implementation of the algorithm and compared them with the patients from Stewart et al. The authors found a decreased abscess rate from 37% to 27%, a decreased suture line failure rate from 14% to 7%, and colon-related mortality decreased from 12% to 5%.28 30 Furthermore, the authors demonstrated there was no association between level of contamination and development of suture line failure. These results further confirmed the results from a prospective study of colon injuries by George et al. In 1989, George and colleagues demonstrated the level of associated contamination was directly related to the development of intra-abdominal abscess but had no association with the development of suture line failure.31
Other institutions continued to try to identify their own risk factors for morbidity after destructive colon wounds. In 2001, an American Association for the Surgery of Trauma multi-institutional study was performed, evaluating 297 penetrating colon injuries requiring resection from 19 different trauma centers.32 The authors performed a regression analysis that identified severe fecal contamination, transfusion ≥4 units PRBCs and single agent antibiotic prophylaxis as independent predictors of complication. Despite these findings, the authors concluded primary anastomosis should be considered in all such patients secondary to the reduced quality of life and the need for subsequent operation in colostomy patients.
Recognizing the potential selection bias that exists with multi-institutional studies in which each different trauma center may perform different management schemes for destructive colon injuries, the Memphis group further evaluated the durability of their single management protocol during a two-decade experience. In 2012, the authors evaluated 102 penetrating destructive colon wounds since the 2002 study.33 The results were notable for a linear decrease in abscess formation from 37% in the Stewart's study to 18%. Furthermore, the rate of suture line failure consistently declined to just below 5%. Colon-related mortality also steadily decreased, from as high as 12% in the original study to 1% (figure 2).28 33

{kind=link}
{kind=link}
Colon-related morbidity and mortality after implementation of a defined management algorithm for penetrating colon injuries. The percentage of abscess formation, suture line failure and mortality is represented along the vertical axis. The solid line represents abscess formation, the dots represent suture line failure and the dashes represent mortality.
Of the 102 destructive injuries observed in the 2012 study, 92 patients were managed according to the clinical pathway, allowing a greater than 90% compliance with the management algorithm. Of the 92 patients that followed the pathway, 69 received resection and anastomosis. Two of these patients developed suture line breakdown. Therefore, the authors concluded with strict adherence to the algorithm for those patients undergoing resection plus anastomosis, the overall suture line failure rate would have decreased to 2.7%, a rate similar to, if not less than, that reported in the current literature for elective colon resections.34–39 Among the institution's 10 deviations from the algorithm, three patients received diversion in the absence of high-risk criteria, and seven patients who met criteria for diversion underwent resection plus anastomosis. Of these seven patients, two developed suture line breakdown, generating a 29% suture line failure rate, similar to that seen for high-risk patients receiving resection and anastomosis in Stewart's original study (42%).28 33
Colon wound location
Although specific risk factors for suture line failure after resection and anastomosis remain inconsistent between institutions, selective use of diversion for destructive colon injuries results in low morbidity. Despite evidence-based reports leading to more well-defined risk factors, the concern that left-sided colon injuries treated with resection plus anastomosis carry an increased risk of complications remains unproven.3 This perception originated from historic autopsy studies demonstrating a tenuous collateral circulation between the ascending branch of the left colic artery and the left branch of the middle colic artery in almost half of cadavers.40 41
Although previous reports have failed to identify location of colon injury (right sided vs left sided) to be a risk factor for complications, results of some retrospective studies demonstrate that location may continue to dictate management at some institutions. In one study of penetrating colon injuries, diversion was performed in only 31% of right-sided wounds as opposed to 88% of the left-sided injuries, with no eventual difference in colon-related outcomes.42 In the American Association for the Surgery of Trauma's 2001 multicenter prospective trial involving 297 patients with destructive colon injuries, one-third of the right-sided wounds were managed with diversion compared with over half of the left-sided wounds.32 The discrepancy was further demonstrated in military data. From one report of 175 colorectal injuries from Operation Iraqi Freedom, diversion was performed for only 19% of right colon wounds compared with 36% of left-sided injuries.43 However, most institutions do not have defined protocols for management of colon injuries and choice of repair is left to the discretion of the operating surgeon. Therefore, the retrospective nature of these studies cannot allow for us to elucidate the exact reasons for this inconsistency based on location.
In 1981, a review of 105 patients with penetrating colon injuries was the first study to primarily investigate outcomes of right-sided versus left-sided wounds. The authors found similar rates of diversion, morbidity and mortality between right-sided and left-sided injuries.44 Despite these promising results, some argue colon wounds should be stratified into more anatomically distinct groups rather than just ‘right’ and ‘left.’ Dente et al identified 217 patients with penetrating colon injuries, comparing characteristics and management between wounds to the ascending colon, transverse colon, descending colon and sigmoid. Baseline characteristics, injury severity and method of repair were similar between the four groups. Although specific analysis of outcomes between the four distinct regions was not performed, a detailed review of the seven patients who developed suture line failure revealed three occurred in the distal transverse colon and four in the splenic flexure. The authors concluded that management of even simple wounds to the splenic flexure should be treated with caution, yet further prospective data need to be obtained.45
In a majority of the previous reports, operative management was left to the discretion of the surgeon, which can create a selection bias. As stated earlier, based on the results of Stewart et al,28 the Memphis group centers operative decisions for colon injuries on the previously defined management algorithm, regardless of injury location (figure 1). In 2012, Memphis performed a study of 469 colon wounds to evaluate the impact of injury location on outcomes in patients managed with this algorithm.46
Similar to Dente et al, the study stratified wounds into four groups based on anatomic location. Patient characteristics, injury severity and management were not equivalent between the different locations. Sigmoid colon injuries were associated with a larger transfusion demands (mean 8.8 units). As the patients were managed according to an algorithm that bases operative decisions on transfusion requirements, it is not surprising that a larger proportion of sigmoid injuries (17%) received diversion compared with the other injury locations. Stab wounds caused more injuries to the transverse colon (18%) than the other anatomic regions, explaining the lower incidence of destructive injuries (23%) within this group and thus, the higher proportion of transverse colon injuries managed with primary repair as well.46
Colon-related morbidity (suture line failure and abscess) and colon-related mortality did not differ between the injury locations in the Memphis study. However, discrepancies associated with repair technique and proportion of destructive wounds between the anatomic regions could potentially mask these differences in outcome. Therefore, the authors performed a multivariable logistic regression analysis to account for potential confounding variables. After adjusting for variables related to degree of shock at presentation, injury severity and operative management, location of injury was still not associated with adverse colon-related outcomes (table 2).46
Adjusted ORs for suture line failure, colon-related morbidity and colon-related mortality in all patients based on anatomic location of injury
Blunt colon wounds
Wounding of the colon as a result of blunt mechanism of injury occurs rarely, with a reported incidence of only 0.1%–0.5% of all trauma evaluations.47 48 Not surprising, the current literature is relatively sparse concerning the management of blunt colon injuries. The massive deceleration force or crush injury associated with the blunt mechanism makes these colon wounds more susceptible to ischemia from mesenteric compromise. Therefore, traditional management schemes for penetrating colon injuries may not apply to blunt injuries, putting these patients at a higher risk for suture line failure.
In 2013, the Memphis group once again performed a study to evaluate the impact of their management algorithm on outcomes after blunt colon injury.49 The authors recognized that blunt colon injuries are obviously different from penetrating injuries, as these wounds are more prone to ischemia. Determination of destructive injuries was based on intraoperative observational criteria different from those used for penetrating wounds. Indicators of blunt destructive colon injuries were serosal wounds involving > 50% of the colon wall circumference, mesenteric devascularization and full-thickness perforations (box 2).
Indicators of a destructive blunt colon injury
Serosal tear >50% colon circumference
Full-thickness perforation
Mesenteric devascularization
The authors identified 151 blunt colon injuries during a 13-year experience. Although the defined management algorithm from Stewart's initial study was based on established risk factors originally identified for penetrating injuries,28 in Memphis, operative decisions for all colon injuries have followed that protocol. This is demonstrated by the fact that adherence to this previously defined algorithm was 95% for the 151 blunt colon injuries in this study.49 All 75 patients with non-destructive injuries underwent primary repair. Out of 76 destructive injuries, 44 underwent resection plus anastomosis, 29 underwent diversion, and 3 patients who met criteria for resection and anastomosis underwent primary repair. Of the 44 patients who underwent resection plus anastomosis, five required preoperative or intraoperative transfusion >6 units of PRBCs and were considered protocol violations because they did not receive diversion.
Of the 75 patients undergoing primary repair and 44 patients undergoing resection plus anastomosis, three developed suture line failure. On further analysis of these patients with suture line failure, two occurred in patients that were managed according to the algorithm, demonstrating a leak of around 1.7% in that group. Within the institution's eight protocol violations, there was one leak, demonstrating a 12.5% leak rate for those patients not managed according to the algorithm. Although patients not managed according to the algorithm had almost a 10-fold higher rate of suture line breakdown, the low number of protocol violations in this study failed to demonstrate this difference as significant.49
For those patients that met criteria for resection plus anastomosis in the study, the authors compared demographics and injury characteristics between those who developed suture line failure and those who did not. Although patients that developed suture line failure trended towards a higher Abdominal Abbreviated Injury Scale (Abd-AIS), this difference was not statistically significant (4 vs 3, p=0.06). In general, the Memphis group demonstrated a suture line failure rate of 2%, abscess formation rate of 5% and a colon-related mortality of 2.8%. These rates are lower than that reported in other series of blunt colon trauma50 51 and are comparable with those demonstrated with penetrating injuries managed with the algorithm.33 Therefore, the authors concluded adherence to the defined management algorithm, originally defined for penetrating colon injuries, was efficacious for the management of blunt colon wounds.49
Abbreviated laparotomy
Contemporary management of critically injured patients after abdominal trauma associated with shock involves initial control of hemorrhage and gastrointestinal contamination, followed by temporary abdominal closure and transfer to the intensive care unit (ICU). Stone et al originally described this innovative strategy of an ‘abbreviated laparotomy’ and was later referred to as ‘damage control laparotomy’ by Rotondo et al. The concept of the abbreviated laparotomy has demonstrated improved survival in the face of coagulopathy, acidosis and hypothermia.52–58 This strategy allows for optimal resuscitation in the ICU and return to the operating room under more favorable conditions.
Destructive colon injuries managed in the setting of an abbreviated laparotomy are initially resected and the bowel is left in discontinuity. After resuscitation, at subsequent laparotomy, the surgeon is left with the decision regarding how to safely manage the resected segment (delayed anastomosis vs diversion). Unfortunately, existing management guidelines for these injuries were defined prior to the widespread use of abbreviated laparotomy and do not necessarily address the issue of delayed anastomosis after resuscitation. The risk factors identified for suture line failure after resection and anastomosis of destructive colon wounds after single laparotomy may not apply to the same injuries in those patients managed with an abbreviated laparotomy. As a result, relatively limited data exist to specifically guide the management of these injuries after abbreviated laparotomy.59–65
In 2007, Miller et al reported the first series of patients with destructive colon injuries managed with an abbreviated laparotomy.59 In their study of 11 patients that underwent initial resection with delayed anastomosis, the authors found no suture line failures, concluding delayed anastomosis is safe in the setting of an abbreviated laparotomy. However, almost half of the patients (45%) in the delayed anastomosis group died prior to hospital discharge, with one identified colon-related death.
In 2009, the groups from Alabama and Denver both reported their experience with these injuries.60 61 Weinberg et al 60 evaluated 56 patients with colon injuries managed with abbreviated laparotomy during a 7-year period. Of these patients, 33 underwent resection with delayed anastomosis. For these patients undergoing resection plus delayed anastomosis, 12% developed suture line failure. In addition, the rate of colon-related complications in patients managed with delayed anastomosis was significantly higher than among those managed with a single laparotomy. With these findings, the authors concluded that anastomosis in the setting of an abbreviated laparotomy should be undertaken with caution, and diversion may be a safer alternative. Kashuk et al 61 reported a similar experience with 25 patients undergoing delayed anastomosis after abbreviated laparotomy. Although the authors’ suture line failure rate of 16% was higher than that of the Alabama group, they concluded delayed anastomosis was safe in most patients managed in the setting of damage control.
Ott et al reported the largest single institutional experience of patients managed with delayed anastomosis.62 Of 44 patients undergoing delayed anastomosis, the authors noted a suture line failure rate of 27%. Given the considerable increased risk of anastomotic dehiscence in these patients, the authors concluded anastomosis in the setting of an abbreviated laparotomy should not be routinely performed. A handful of other publications have reported series of colon injuries managed with an abbreviated laparotomy, all of which provided mixed conclusions.63–66
In 2014, Memphis evaluated the applicability of their defined management algorithm to destructive colon injuries after abbreviated laparotomy, recognizing this protocol was never set in place for this damage control technique. The authors reported a 17-year experience of 149 patients with colon wounds managed with abbreviated laparotomy, of which 42 were managed with resection and delayed anastomosis.67 When comparing patients who developed suture line failure to those who did not, they were unable to identify any additional significant risk factors. However, when applying the previously defined management algorithm for destructive colon injuries to those patients who underwent delayed anastomosis, the group noted over half (55%) of the patients were managed according to the protocol set in place for a single laparotomy. Analysis of these patients further demonstrated a substantial decrease in colon-related morbidity compared with those patients not managed according to the algorithm (table 3). In fact, suture line failure after delayed anastomosis decreased from 32% in those patients not managed according to the algorithm to 4% in those patients managed according to the algorithm (p=0.03), a rate comparable with that demonstrated with colon injuries managed with the algorithm for a single laparotomy.33 49 The Memphis group then concluded that for destructive injuries, delayed anastomosis may be performed at the subsequent exploration in patients without significant transfusion requirements or comorbidities with an acceptably low morbidity and mortality. A comparison of suture line failure rates from the studies evaluating delayed anastomosis after abbreviated laparotomy is demonstrated in table 4.
Comparison of patients that underwent delayed anastomosis managed according to the algorithm versus patients not managed according to the algorithm
Comparison of suture line failure across series evaluating delayed anastomosis after abbreviated laparotomy
Conclusions
Colon injuries remain a relatively common, yet sometimes challenging, clinical problem for a trauma surgeon. The remarkable evolution in the management of these injuries during the past two centuries is clearly demonstrated by the improvements in both morbidity and mortality. What was once considered a fatal wound during the Civil War, colon injuries now carry a mortality rate less than 1%. Multiple evidence-based studies during the last several decades have allowed for more aggressive management, with most wounds undergoing primary repair or resection and anastomosis with an acceptably low suture line failure rate. Unfortunately, there remains some debate among institutions regarding which patients are at increased risk for colon-related morbidity, especially for those patients left in colonic discontinuity after an abbreviated laparotomy. Some programs have developed data-driven protocols that have simplified management of destructive colon wounds, clearly identifying those high-risk patients that should undergo diversion, regardless of mechanism or anatomic location.
Footnotes
Contributors Drafting of manuscript: JPS.
Critical revision: LJM, TCF and MAC.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/